Transcription
Running Head: IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENTImproving Adherence to Atypical Antipsychotic Agent Screening Guidelinesin Pediatric Patients: A Quality Improvement Project Within anIntegrated Community Mental Health SettingElishia Riffle RN, MSN, CPNP, PMHS, DNP StudentThe University of Texas Arlington College of NursingIn partial fulfillment of the requirements ofN6621 DNP Practicum IIDr. Sharolyn Dihigo DNP, RN, CPNP-PCNovember 30, 20161
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT2Table of ContentsAbstract. . . . . . . . . . . . . . . . . . . . . . . . 3Literature Review . . . . . . . . . . . . . . . . . . . . 4Theoretical Framework . . . . . . . . . . . . . . . . . . . . . . . 7Study Question . . . . . . . . . . . . . . . . . . . 7Methods . . . . . . . . . . . . . . . . . . . . . . . 7Analysis . . . . . . . . . . . . . . . . . . . . 10Results . . . . . . . . . . 11Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Limitations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Implications . . . . . . . . . . . . . . . . . . . . 13Conclusions . . . . . . . . . . . . . . . . . . . . . . . 14References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15Appendix A . . . . . . . . . . . . . . . . . . 18Appendix B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Appendix C . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT3AbstractBackground: Approximately 14% - 20% of children and adolescents have a mental healthproblem (Harrison, Cluxton-Keller, and Gross, 2012). Atypical Antipsychotic Agents (AAA) areused to treat behavioral, emotional, and mental health problems in children and adolescents. Adiscrepancy between best practices and actual practices exist.Objective: To increase adherence, above baseline, to recommended screening guidelines inchildren, ages 4-18, prescribed Atypical Antipsychotic Agents over 12 weeks.Results: Aggregate comparison of the mean ranks of scores were tested with the Mann-WhitneyU test, U 1,087.5, n 1 n2 70, total N 140, p .001. All seven variables were observed andtested using the Chi Square with Fisher's Exact tests and are significant at or above 99%confidence (p 0.01).Conclusion: Educating the Mental Health Provider (MHP) on the recommended screeningguidelines and implementing a checklist had a measurable effect on increasing adherence to therecommended screening guidelines.
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT4Mental health is an integral part of a person's overall wellbeing. Mental health conditionsaffect not only the person living with the condition but the community as a whole and can affectpeople of all ages. Children with emotional and behavioral problems are more likely to haveproblems in school, be involved with the justice system, require special services within theeducation system, and are more likely to become unemployed adults. It is approximated that 14%- 20% of children and adolescents have a mental health problem (Harrison, Cluxton-Keller, andGross, 2012).Atypical Antipsychotic Agents (AAA), also called Second Generation Antipsychotics(SGA), are one drug class used to treat behavioral, emotional, and mental health problems suchas bipolar disorder, Tourette' s syndrome, schizophrenia, and symptoms of autistic disorders.Visits relating to the prescribing of AAA in children increased eight fold between 1995 and2005(0.3 million - 2.4 million) (Alexander, Gallagher, Mascola, Moloney, & Stafford, 2011).Between 1995 and 2002 a fivefold increase was seen in the prescribing of antipsychotic drugs forchildren and adolescents (Cooper et al., 2006). Off label uses of AAA in children increased from55 % to 67 % between 1995 and 2008 (Alexander, Gallagher, Mascola, Moloney, & Stafford,2011).Literature ReviewAll antipsychotic medications have potential concerning side effects. However, AAAhave a lesser chance of causing extrapyramidal side effects than First Generation Antipsychotic(FGA) medications. Two systematic reviews examining the side effects caused by AAA foundweight gain to be a statistically significant common side effect (Almandil et al., 2013; De Hert,Dobbelaere, Sheridan, Cohen, & Correll, 2011). Prolactin, lipids, glucose, and total cholesterollevels were also found to be significantly increased in patients taking AAA (Almandil et al.,
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT52013; De Hert et al., 2011). The significant weight gain related to AAA use contributes toobesity, which in turn leads to hyperlipidemia, diabetes, and increased risk factors forcardiovascular disease (CVD) (Almandil et al., 2013).The American Academy of Child and Adolescent Psychiatry (AACAP) (2011) providedpractice parameters for the use of AAA in children and adolescents. These guidelines reviewevidence regarding the efficacy and safety of AAA, provide suggestions regarding the use ofthese medications in children and adolescents, and make recommendations for the appropriateprescribing and monitoring of side effects. These recommendations support the consensusstatement developed by the American Diabetes Association (ADA), American PsychiatricAssociation (APA), American Association of Clinical Endocrinologists (AACE), and the NorthAmerican Association for the Study of Obesity for monitoring those patients prescribed an AAA(AACAP, 2011).The monitoring protocol as outlined by the consensus statement recommended obtaininga thorough personal and family history, screening for risk factors of CVD, hypertension,diabetes, obesity, and dyslipidemia, along with obtaining a waist circumference (WC) prior toinitiation of an AAA and then annually (Consensus development conference, 2004). Body MassIndex (BMI) is to be obtained prior to initiation of an AAA and at 4 weeks, 8 weeks, 12 weeks,and quarterly thereafter (Consensus development conference, 2004). Blood pressure (BP) and afasting blood glucose should be obtained prior to initiation, at 12 weeks, and annually(Consensus development conference, 2004). A fasting lipid profile is recommended prior toinitiation, at 12 weeks, and then at 5 years (Consensus development conference, 2004). In thosepatients with a positive family history of cardiovascular disease or syncope, an
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT6electrocardiogram should be performed (AACAP, 2011). Additional monitoring may be neededfor those with a higher baseline risk or as clinically indicated.Although practice parameters and recommended screening guidelines are available, adiscrepancy between best practices and actual practices has been shown (Pappadopulos et al.,2002). In a literature review conducted by Bauer (2002) adequate adherence to guidelines wasfound in only 27 % of cross sectional studies and those studies looking at pre and post guidelineimplementations. A systematic review and meta-analysis found a large gap between therecommended screening practices and completed screenings. Mitchell . . concluded routinemetabolic screening in psychiatric practices is insufficient to detect metabolic abnormalities(Mitchell, Delaffon, Vancampfort, Correll, & De Hert, 2012). Bauer (2002) and Mitchell et al.(2012) found Mental Health Providers (MHP) were not consistently adherent to recommendedpsychiatric guidelines.Checklists have been successfully used in other disciplines and have been shown to besuccessful tools in health care (Chaudhary et al., 2015; Hales, Terblanche, Fowler, & Sibbald,2008). A systematic review completed by Ko, Turner, and Finnigan (2011) found checklists canimprove protocol adherence and patient safety. Checklists can be tailored and designed withinput from key stakeholders; therefore, making them valuable tools for guidelineimplementation. Borchard, Schwappach, Barbir, & Bezzola (2012) concluded, "Checklist areeffective and economic tools that decrease mortality and morbidity" (p.925). When checklistsare developed with input from those who will be using the tool, compliance with the use of thetool itself and adherence to the guidelines improved (Borchard, Schwappach, Barbir, & Bezzola,2012).
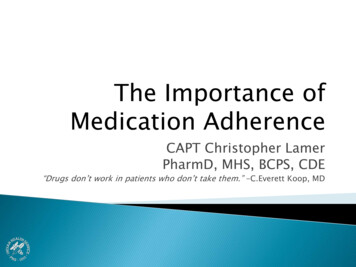
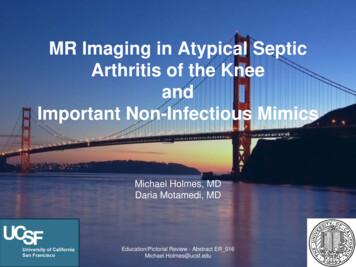
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT7Theoretical FrameworkThe Theory of Change (ToC) was used to collaboratively design a process between allstakeholders. This involved formulating a plan, stating the objectives and goals, and thenthoroughly considering all of the necessary preconditions to make these goals and outcomessuccessful. This process was broken down into the smallest details including gaining input,collaboration, and support from all of the providers at each step. A framework was built showinghow the necessary preconditions, processes, interventions, actions, monitoring, and evaluationsneeded to work together to create a cohesive environment, overcome possible barriers, andachieve the long term goals of the project (Appendix A).Study QuestionDue to the lack of provider's adherence to the recommended monitoring protocols forAAA, this quality improvement (QI) project was conducted to determine whether implementinga checklist would increase adherence to recommended screening guidelines for patientsprescribed AAA among Psychiatric Mental Health Providers treating pediatric patients' ages 418 years. Each screening parameter (personal history, family history, WC, BMI, BP, fastingglucose, fasting lipids) was examined for adherence through a randomized retrospective chartreview prior to implantation of the QI. The same parameters were collected post QI intervention.MethodsSettingThis QI project was implemented in an integrated community mental health centerserving children and adolescents ages 4 to 18 years. The agency is the largest provider of mentalhealth services in the Dallas Forth Worth (DFW) Metroplex with multiple locations providing
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT8services to both adults and children. Last year 15,000 children received services from thisagency. Multiple services are provided within the same location: mental health, pharmacy,primary care, housing, and other social services. This specific location is the busiest center inDFW, serving approximately 1,200 children and adolescents a month. Not all patients receivemedications; some patients receive counseling, skills related therapies, and/or social services.The patients served at this location were seen by one of seven providers (three Child andAdolescent Psychiatrist and four Psychiatric Mental Health Nurse Practitioners (PMHNP)).These providers collectively will be referred to as MHP for the rest of this article. Each MHPsees on average 25-35 patients a day. An Electronic Medical Record (EMR) is used in thissetting and was utilized for data collection purposes.SampleA convenience sample comprised of the seven MHP was used. Chart audit criteria usedincluded established patients, of at least fifteen months, between the ages of 4-18 years,prescribed an AAA. The requirement of fifteen months was established so that recommendedannual screenings could be captured. Charts of patients below the age of 4 years or above the ageof 18 years were excluded. Patients that had not established care for at least fifteen months wereexcluded from this study.Planning PhaseDiscussions for this QI project began at monthly integrated meetings including membersof both the primary care and mental health teams. Providers first identified laboratory processeswere not functioning well within the clinic and were a barrier to following the recommendedscreening guidelines. Members shared other concerns including time constraints, patient volume,
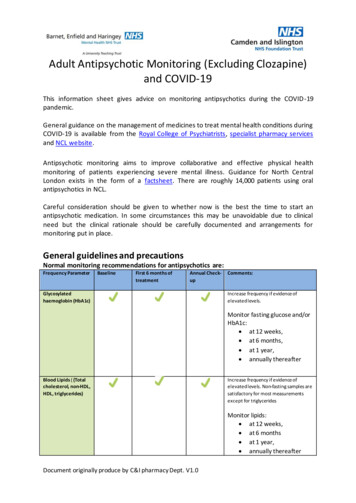
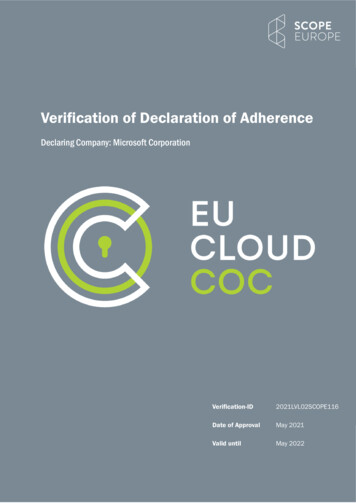
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT9and lack of knowledge of the AACAP guidelines and recommended screening protocols.Staffing shortages were identified as an additional barrier.Next a QI project plan was developed with feedback from key stakeholders. Streamliningof the laboratory ordering and receiving of results had to be resolved prior to the start of the QIproject. A checklist was created, and a two week pilot study was conducted. During pilot study,multiple processes were tested and feedback was received. The checklist and process wasmodified to reflect changes.Education PhaseDuring an integrated meeting, the MHP were provided with the "Practice Parameters forthe Use of Antipsychotic Medications in Children and Adolescents", the "ConsensusDevelopment Conference on Antipsychotic Drugs and Obesity and Diabetes", the checklistlaminated on yellow paper (appendix B), and blood pressure charts showing the systolic anddiastolic BP percentiles for both males and females ages 1-17 years. These documents wheremade available on paper and in electronic formats. Training on the use of the EMR, requireddocumentation, and vital signs assessment, including waist circumference measurements, wascompleted with the MHP and Medical Assistant (MA) staff.Implementation PhaseCollaboration and uniformity were key components to making this QI project successful.The process flow began when the MHP saw a patient and determined what recommendedscreenings were needed. Each MHP had a copy of the checklist to prompt recommendedscreenings (Appendix B). During the visit, the MHP would determine the status of the personaland family history and update as indicated in the EMR. When the MHP determined the vital
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT10signs or labs were needed, the MHP would send the patient to the MA. The MA would obtainand record the needed vital signs in the EMR and give the parent the lab orders (if needed). TheMA was responsible for following up on pending labs results, providing completed labs to theordering provider, and following up with the family via phone call if labs were not completed.MeasurementA randomized retrospective chart review was completed on 70 charts to collect pretestdata. Documentation of the BMI, BP, WC, patient's personal and family history, and theordering of the fasting blood glucose and lipids at the recommended intervals was collected.Documentation of each variable was assessed and given a score of zero if not found and one iffound. A total of seven variables were assessed allowing for a range of zero to seven. Forexample, if none of the variables were found to have been documented a score of zero wouldhave been assigned, if three of the seven variables were found to have been documented a scoreof 3 would have been assigned, and if all seven variables were found to have been documented inthe EMR them a score of seven would have been assigned. Actual values of the vital signs andlab results were not included. A chart review post intervention was completed on 70 randomlyselected charts assessing the same parameters on patients meeting inclusion criteria and seenduring the 12 week intervention time frame.AnalysisData analysis was completed using the IBM-SPSS Statistics software application version20. A summated compliance score was calculated for each of the seven compliance variable: BP,BMI, WC, personal history, family history, fasting blood glucose, and lipids. When the variablebeing observed was recorded and documented during the visit being audited, it was tallied asYes, compliant and encoded in the analysis data set with a value of 1, else it was tallied as No,
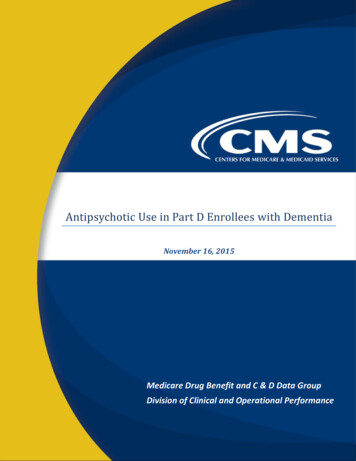
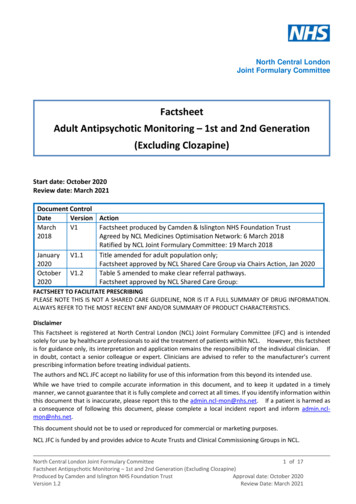
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT11non-compliant and assigned the value of zero. The algebraic sum of these variables per visitchart audited, is the compliance score. The Independent-Samples Mann-Whitney Unonparametric test was used to statistically compare the differences of mean ranks in the pre andpost intervention summated compliance scores. The null hypothesis rejection threshold was set atan alpha error of five percent (p 0.05 two tailed, 95% significance level). Pearson Chi-Squaretests were used to compare the difference in observed versus expected proportions of frequenciesof compliance for each of the seven compliance variables.ResultsData was collected as 70 pre intervention patient observations and 70 post interventionpatient observations for a total of 140 observations. The relative and aggregate compliance of thepre and post interventional groups were compared using nonparametric statistical testingmethods. In the aggregate comparison, the mean ranks of scores with the Mann-Whitney U testreveals the mean rank of scores were 51.04, N 70 (pre) and 89.96 N 70(post). Distributionsof scores in the two groups were significantly different and were aggregated higher in the postintervention group than they were in the pre intervention group, Mann-Whitney U 1,087.5, n 1 n2 70, total N 140, p .001 two tailed (Appendix C). The null was rejected. There is ameasurably higher mean rank of compliance score in the post interventional group and isstatistically significant (p 0.05 two tailed). The discovery of a statistically significant differencethat is higher in the post interventional group is an important clinically significant finding of thisproject. The proportional frequencies of pre versus post compliance for BP, BMI, WC, personalhistory, family history, fasting blood glucose, and lipids were observed and tested using ChiSquare with Fisher's Exact tests. Pre versus Post compliance for each of these variables showedstatistically significant differences (p 0.05) when tested with nonparametric Chi Square tests
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT12and Fisher's Exact tests as displayed in Table 1. The proportion of compliance is significantlyhigher in each of the post intervention groups. All seven variables are significant at or above99% level of significance (p 0.01, 2 tailed) as shown in Table 1.Table 1 Pre vs. Post Compliance Chi Square TestsPre lnteventionVariableNoYesTotalPost Intervention%No %YesNoYesTotal%No %YesCIII Squorct Fisher's Exact 2 SidedS/gnfflc:once { p JBlood Pressure 16547022.9%77.1%367704.3%95.7%0.002BMI 18S27025.7%74.3%l69701.4%98.6%0.000Waist Orcumference 70070100.0%0.0% 59117084.3%15.7%0.001Personal History 6377090.0%10.0% 41297058.6%41.4%0.000Family Historv 6827097.1%2.9% 51197072.9%27.1%0.000Glucose 6468.6% 43277061.4%38.6%0.0001707091.4%Upld Compliance 6998.6%1.4% 41291058.6%41.4%0.000DiscussionThis QI project demonstrates educating the MHP on the recommended screeningguidelines and implementing a checklist had a measurable effect on increasing adherence to therecommended screening guidelines. Each variable demonstrated a statistically significantincrease in proportion of adherence (compliance) to non-adherence (non-compliance) afterimplementation of the checklist. Although there were statistically significant improvements seenin all measured variables, additional improvements can be made. For example the WCmeasurements captured in the random sample prior to implementation of the checklist was zero.Post implementation of the checklist the WC measurements captured was 11 leaving still 59 ofthose sampled not having a WC measurement recorded. Prior to implementation of this project,WC was not being collected; however, the BP and BMI were recorded. This disparity in preversus post frequency counts and proportions of compliance are shown in Table 1. Twoadditional MA's were hired during the intervention and could have played a factor in thecollection of vital signs.
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT13According to Greenhalgh . (2004), removing barriers and piloting each piece of anintervention prior to implementation will increase the success of the intervention (Greenhalgh,Robert, Macfarlane, Bate, & Kyriakidou, 2004). Therefore, prior to implementing the checklist aprocess was put in place for the ordering and processing of lab orders previously identified as abarrier.Anecdotal findings from this QI include missed opportunities for collecting the WC. WCmeasurements were only being collected on patients when labs were ordered by the MHP.Furthermore, patients who were prescribed AAA who needed WC measurements were missed.During data collection, some of the MHP did improve above baseline in the personal historycollection; however, the MHP did not meet the requirement of documenting a full history.LimitationsThe main limitations of this study are the use of a convenience sample, small sample size,lack of control group, and length of the study. This QI project was limited to one location using aconvenience sample. Since the MHP knew the project was being conducted, they may haveimproved on some points of care. The study was conducted over 12 weeks; therefore, it did notrepresent an entire year, nor did it capture the sustainability of the intervention. A randomsample including a control group, extending the length of the study to include two fullcomparative years to control for season to season variations, and including multiple locationswould greatly strengthen this QI project. Future Doctor of Nursing Practice (DNP) studentscould use these findings to expand and strengthen this QI project.ImplicationsThis QI project demonstrated checklists are useful tools in healthcare that can be utilizedto increase adherence to guidelines. Additional studies implementing the checklist at multiple
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT14locations over longer periods of time would be useful in determining its sustainability.Implementing the checklist into the EMR could improve the ease and usage. For example,validations can be implemented within the EMR to prevent the closing of a patient entry withoutthe required vital signs, missing documentation of the personal or family history, orrecommended labs being ordered. Validations could prompt the MHP regarding missinginformation or allow documentation of why the lab or vital sign was not collected. Providing achecklist format for the family and patient history, instead of a free text box, would improveuniformity to the histories collected. Although the checklist itself did improve adherence to therecommended screening guidelines, implementing these data points into the EMR would allowfor system wide implementation.ConclusionsThe cause of MHP's low adherence rates to the AACAP "Practice Parameters for the Useof Atypical Antipsychotic Medications in Children and Adolescents" practice parameter andsupported consensus statement is twofold. A portion of MHPs are unaware of the guidelinesalthough they were published in 2011, while other providers have expressed difficulty inimplementing the recommended screening guidelines into practice. This QI project demonstrateseducating the MHPs on the recommended screening guidelines and implementing a checklist hada measurable effect on increasing adherence to the recommended screening guidelines.Doctorally educated clinicians are perfectly suited to conduct interprofessional integratedprojects, function successfully within a leadership role, and improve quality of care throughimplementation of quality improvement projects to improve patient outcomes.
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT15ReferencesAlexander, G. C. , Gallagher, S. A., Mascola, A. , Moloney, R. M., & Stafford, R. S. (2011).Increasing off-label use of antipsychotic medications in the united states, 1995-2008.Pharmacoepidemiology and Drug Safety, 20(2), 177-184. doi: 10.1002/pds.2082Almandil, N. B., Liu, Y., Murray, M . L. , Besag, F. M., Aitchison, K. J., & Wong, I. C. (2013).Weight gain and other metabolic adverse effects associated with atypical antipsychotictreatment of children and adolescents: A systematic review and meta-analysis. PaediatricDrugs, 15(2), 139-150. doi:10.1007/s40272-013-0016-6American Academy of Child and Adolescent Psychiatry. (2011). Practice parameters for the useof antipsychotic medications in children and adolescents. Retrieved fromhttp://www.aacap.org/ App Themes/AACAP/docs/practice parameters/AtypicalAntipsychotic Medications Web.pdfBauer, M. S. (2002). A review of quantitative studies of adherence to mental health clinicalpractice guidelines. Harvard Review of Psychiatry, 10(3), 138-153.doi: 10.1080/10673220216217Borchard, A. , Schwappach, D.L.B., Barbir, A., & Bezzola, P. (2012). A systematic review of theeffectiveness, compliance, and critical factors for implementation of safety checklists insurgery. Annals of Surgery, 256(6), 925-933.Chaudhary, N., Varma, V., Kapoor, S., Mehta, N., Kumaran, V., & Nundy, S. (2015).Implementation of a surgical safety checklist and postoperative outcomes: A prospectiverandomized controlled study. Journal of Gastrointestinal Surgery, 19(5), 935-942.doi: 10.1007/s/11605-015-2772-9
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT16Consensus development conference on antipsychotic drugs and obesity and diabetes. (2004).Diabetes Care, 27(2), 596-601. doi:10.2337/diacare.27.2.596Cooper, W. 0., Arbogast, P. G., Ding, H., Hickson, G. B., Fuchs, D. C., & Ray, W. A. (2006).Trends in prescribing of antipsychotic medications for US children. Ambulatory Pediatrics,6(2), 79-83. bp.2005. l 1.002De Hert, M., Dobbelaere, M., Sheridan, E. M., Cohen, D., & Correll, C. U. (2011). Metabolicand endocrine adverse effects of second-generation antipsychotics in children andadolescents: A systematic review of randomized, placebo controlled trials and guidelines forclinical practice. European Psychiatry: The Journal of the Association of EuropeanPsychiatrists, 26(3), 144-158. doi: 10.1016/j.eurpsy.2010.09.011Greenhalgh, T., Robert, G., Macfarlane, F., Bate, P., & Kyriakidou, 0. (2004). Diffusion ofinnovations in service organizations: Systematic review and recommendations. The MilbankQuarterly, 82 (4), 581-629Hales, B., Terblanche, M., Fowler, R., & Sibbald, W. (2008). Development of medical checklistfor improved quality of patient care. International Journal for Quality in Health Care,20(1), 22-30. n, J. N., Cluxton-Keller, F., & Gross, D. (2012). Antipsychotic medication prescribingtrends in children and adolescents. Journal of Pediatric Health Care, 26(2), 016/j.pedhc.201 l .10.009
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT17Ko, H. C.H., Turner, T. J., & Finnigan, M . A. (2011). Systematic review of safety checklist foruse by medical care teams in acute hospital settings - limited evidence of effectiveness. BioMed Central Health Services Research, 11(211), 1-9. doi: 10.1186/1472-6963-11-211Mitchell, A. J., Delaffon, V., Vancampfort, D., Correll, C. U., & De Hert, M. (2012). Guidelineconcordant monitoring of metabolic risk in people treated with antipsychotic medication:Systematic review and meta-analysis of screening practices. Psychological Medicine, 42(1),125-147. doi: 10.1017/S003329171100105XPappadopulos, E., Jensen, P. S., Schur, S. B, MacIntyre, S. K., II, Van Orden, K., Sverd, J., . .Rube, D. (2002). "Real world" Atypical antipsychotic prescribing practices in public childand adolescent inpatient settings. Schizaphrenia Bulletin, 28 (1 ), 111-121. Retrieved g/
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT18Appendix AImproving AdherenceTheory of rovedquality of careto patientsserved.Early detectionofhyperlipidemiaassociatedwith AAA useEarly detectionofhyperglycemiaassociatedwith AAA useEarly detectionofhypertensionassociatedwith AAA useEarlydetection ofobesityassociatedwith AAA useProviders' adherence tothe checklist/Implementation ofchecklist withongoing monitoringStart by recognizing theproblem-- IMeet with key stakeholdersidentifying potentialinterventions and outcomemPrl SIJrP.c; ---- -----.Feedback from keystakeholders afterpiloting of checkl istand mod ifications ifneededPiloting of checklist Review the literature andcritically appraise theevidence-- Collection of baseline dataCollaborativelydevelop achecklist toolinvolving keystakeholdersto helpimproveadherencerates
IMPROVING ADHERENCE TO ATYPICAL ANTIPSYCHOTIC AGENT19Appendix BProvider ChecklistClozaril (Clozapine) Risperdal (Risperidone) Zyprexa (Olanzapine)Seroquel (Quetiapine) Geodon (Ziprasidone) Ability (Aripiprazole)Patient and Family History- Recorded at initiation and updated annually**Don't forget to add the date when you update the history!**Date - Patient's reports/denies a patient and family history of diabetes, highcholesterol, obesity, seizures, cardiac history, sudden unexplained deaths, syncope, or adversereactions to SGA' s.LabsFasting Glucose - Initiation, 12 weeks, and annuallyMore frequently than annually in those who have a higher baseline risk for developmentof diabetesFasting Lipids - Ini
Elishia Riffle RN, MSN, CPNP, PMHS, DNP Student The University of Texas Arlington College of Nursing In partial fulfillment of the requirements of N6621 DNP Practicum II Dr. Sharolyn Dihigo DNP, RN, CPNP-PC November 30, 2016 . IMPROVING ADHERENCE TO A TYPICAL ANTIPSYCHOTIC AGENT 2 Table of Contents