Transcription
Addressing Sickle Cell CareEdward Donnell Ivy, MD, MPHMedical Officer, Genetic Services BranchMaternal and Child Health BureauHealth Resources and Services Administration
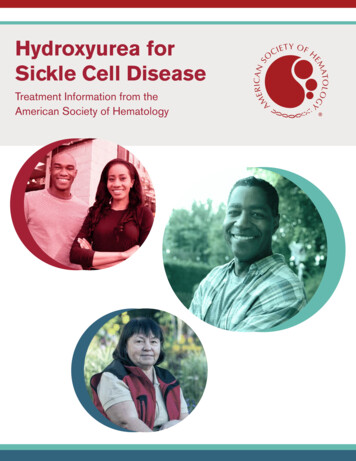
Increases in Life Expectancy of Patients withSickle Cell AnemiaMSH50PROPS I40National Sickle Cell 198019902000Life Expectancy(Years)
Advancements in Sickle Cell That HaveImproved Life Expectance Sickle cell screening Penicillin Prophylaxis Stoke Screening(Transcranial DopplerUltrasound) Blood Transfusion Bone MarrowTransplantation Hydroxyurea
Agencies of Health and Human Services, HHS Administration for Children & Families (ACF)Administration on Aging (AoA)Agency for Healthcare Research & Quality (AHRQ)Agency for Toxic Substances & Disease Registry (ATSDR)Centers for Disease Control & Prevention (CDC)Centers for Medicare & Medicaid Services (CMS)Food & Drug Administration (FDA)Health Resources & Services Administration (HRSA)Indian Health Service (HIS)National Institutes of Health (NIH)Substance Abuse & Mental Health Services Administration (SAMHSA)*Members of HHS Hemoglobinopathies Federal Partners Initiative
Agency for Healthcare Research and Quality Charged with improving quality, safety, efficiency andeffectiveness of healthcare US Preventative Task Force releases recommendations Evidence Based Practice Centers support development ofevidence reports and technology assessments to assistpublic- and private-sector organizations to improve qualityof health care in the United States. In 2008, released report supporting use of Hydroxyurea asan effective therapy in sickle cell disease AHRQ provides grants to study the improvement of sicklecell care, including a grant given to Dr. Paula Tanabe in2011 to study improving emergency care for sickle cellpatients.
Center for Disease Control andPrevention The federal agency responsiblefor protecting the nations healththrough health promotion,prevention of disease, injury anddisability, and preparedness fornew health threatsThe National Center on BirthDefects and DevelopmentalDisabilities has a Blood Disordersdivision which produces sickle cellmaterials and works to improvesickle cell careThe Blood Disorders division isleading the RuSH project,(Registry and Surveillance forHemoglobinopathies)
More on RuSHProject Goals Determine How Many People HaveSCD and Thalassemia Increase Knowledge and Awareness Demonstrate the Value ofSurveillance DataState-based information often includes: Vital records—births, deaths,pregnancies, and pregnancyoutcomes Immunization records—vaccinationsor shots given to prevent diseases Newborn screening results Health care statistics—hospitalizations, emergency roomvisits, and other sources of medicalcare
Health Resources and Services Administration The federal agency responsible for improving access tohealth care services for people who are uninsured,isolated, or medically vulnerable HRSA works with Federally Qualified Health Centers,visiting nurses programs, nursing home programs, andother community based programs designed to reachvulnerable populations The Maternal and Child Health Bureau within HRSA isresponsible for the National Sickle Cell Disease NewbornScreening Program and the National Sickle Cell DiseaseTreatment Demonstration Program
National Sickle Cell Disease NewbornScreening ProgramGoals and Activities Improve follow-up of individualsdetected through newborn screeningand other screening approaches withsickle cell disease, sickle cell trait, andother hemoglobinopathiesAssure that individuals identified withsickle cell disease and otherhemoglobinopathies receive the highestquality of health care and supportiveservices throughout their lifespanAssure that individuals with sickle celldisease, trait and otherhemoglobinopathies—including those in“emerging populations”—receiveappropriate education and counseling toenable them to make informed healthrelated decisions, including, but notlimited to, those related to reproductivechoices
National Sickle Cell Disease TreatmentDemonstration Program Program is designed to establishpractice models for the preventionand treatment of sickle cell diseasethrough the coordinated efforts ofproviders, key stake holders,affected individuals and theirfamilies.Networks have two main goals: support the provision of coordinated,comprehensive, culturally competent andfamily-centered care for individuals withsickle cell disease.work collaboratively with partners such asFederally Qualified Health Centers(FQHC); nonprofit hospitals or clinics;university health centers offering primarycare; subspecialty comprehensive sicklecell centers; and community-basedorganizations that provide resources topeople with sickle cell disease.
National Heart, Lung and Blood Institute Has been involved in sickle cellresearch since 1950’sNHLBI mandated to research sicklecell with passage of Sickle CellDisease Treatment Act of 1972The Division for Blood Disorders andResources sponsors bench andclinical research to improve sickle cellcareThe Division for the Application ofResearch Discoveries is sponsoringthe development of practiceguidelinesThis year, DARD supported theestablishment of the National BloodDisorders Program
National Blood Disorders Program*Coordinating CommitteeProfessional and Non-Profit Organizations:Federal Agencies:1.American Academy of Emergency Medicine2.American Academy of Family Physicians19. Agency for Healthcare Research and Quality(AHRQ)3.American Academy of Pediatrics20. Centers for Disease Control and Prevention (CDC)4.American Academy of Physician Assistants21. Centers for Medicaid and Medicare Services (CMS)5.American Association of Blood Banks22. Food and Drug Administration (FDA)6.American College of Medical Genetics7.American College of Physicians23. Health Resources and Services Administration(HRSA)8.American Osteopathic Association9.American Society of Hematology10. American Society of PediatricHematologist/Oncologist11. International Association of Sickle CellNurses and Physician Assistants12. National Initiative for Children’s HealthcareQuality13. National Medical Association14. Sickle Cell Disease Association of America15. Society for Academic Emergency Medicine24. National Institute of Minority Health and HealthDisparities (NCMHD)25. National Heart, Lung and Blood Institute (NHLBI)26. Office of the Assistant Secretary for Planning andEvaluation27. Office of Minority Health, HHS (OMH)* Convened by the NHLBI
Infrastructure ofNHLBI-Sponsored National Programs Wider circles indicatemore partners A CoordinatingCommittee is theleadership body ofthe Program Work groups addresstargeted topics andprojects Wider involvement isthrough the internetvia a “KnowledgeNetwork” and othermeansCoordinatingCommittee
Functioning of National Partnership ProgramsIndividual/STRATEGIESClinicalby riousSourcesCommon MessagesClinic-CommunityConnectionsKnowledge andBehavior ProgramsNational ProgramsDisease PatternsPolicy &MissionsEpidemiology,Efficacy & CERTheory & ementation &Community Research
Social-Ecological ModelBroader EnvironmentCommunitiesOrganizations(Schools, Worksites,Healthcare)FamilyIndividual
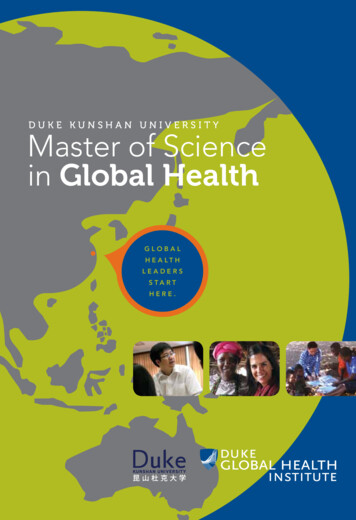
Contribution of Determinants of HealthProportional Contribution ofDeterminants of Health to PrematureDeathSource: Steven A. Schroeder, “We Can Do Better-Improving the Health of the American People,” New EnglandJournal of Medicine, 327, no 12 (September 20, 2007), p. 1222
Barriers Identified fromHydroxyurea Conference (2008)Lack of knowledge about hydroxyurea as a therapeutic optionDifficulty in communication between patients and their caregivers regarding the use ofhydroxyureaNeed for frequent monitoring of response to hydroxuyreaLack of adherence to treatment regimenProvider bias and negative attitudes toward patients with sickle cell disease and theirtreatmentLack of clarity of hydroxyurea treatment regimens and under treatment in adultsLimited number of physicians who have expertise in the use of hydroxyurea for sicklecell diseaseFailure to engage patients /caregivers in treatment decision-making in adevelopmentally appropriate manner
Expert Panel Recommendation on theManagement of Sickle Cell Disease 12-Member Multi-disciplinary Panel Family PhysicianNurse PractitionerTransfusion SpecialistObstetrics/gynecologyHematologists: Internal Medicine, PediatricPsychiatrist Five Chapters Health MaintenanceManagement of Acute ComplicationsManagement of Chronic ComplicationsHydroxyurea TherapyTransfusion
Expert Panel Recommendations Focus Target audiences: Prime: Primary care clinicians Secondary: Specialtyphysicians, healthcaresystems, policymakers, others Goals: Implementable evidencebased recommendations onmanaging sickle cell diseasein clinical practice Identification of gaps inknowledge for additionalresearch
Implementation of Guidelines:A Tree that Bears FruitTransfusionsImplementation ntHydoxyureaGuidelines
Health Maintenance Includes recommendations forprimary care providers andspecialists Examples of recommendation Vaccinate persons with sickle cell toprevent pneumococcal infections Provide penicillin prophylaxis tochildren younger than age 5 toprevent sepsis Screen for stroke risk in childrenwith sickle cell disease usingTranscranial Doppler Ultrasound(TCD) Provide genetic counseling topotential parents
Acute Complications Recommendations primarily targetcare in the emergency room settingIn some cases, the recommendationprovide guidance but does notprovide detailFor example, the guidelines maystate treat pain but does not providedetail about which pain med to use,how often or at which dosesWhen available and appropriate, theguidelines uses guidance from othersources, such as the American PainSociety GuidelinesExamples Acute PainAcute Chest SyndromeWorsening Anemia
Chronic Complications Guidelines attempt to providerecommendations for illnessesthroughout the lifespanDue to limited resources and time,the guidelines are not meant toprovide recommendations on everyaspect of sickle cell diseaseChronic chapter providesrecommendations that can be usedby the primary care provider theemergency provider and thespecialistsExamples Chronic PainRenal ComplicationsPulmonary complications
Hydroxyurea Strong evidence that sickle cellpatients meeting certain criteriashould be started onHydroxyurea Includes recommendations forboth primary care providers andspecialists Includes a protocol for initiatingand maintaining hydroxyureatherapy Effective use of hydroxyurea willrequire an approach that gets allstakeholders involved, includingthe patient, family, primary careproviders, emergency roomstaff, specialists and others
The Chronic Care Model25
Five Key Elements of RevitalizationResident engagementand communityleadershipDevelop strategicand accountablepartnershipsMaintaining aresults focussupported by dataAdapted from White HouseNeighborhood RevitalizationReport, July 2011Investing in andbuildingorganizationalcapacityAlignment ofresources to aunified and targetedimpact strategy
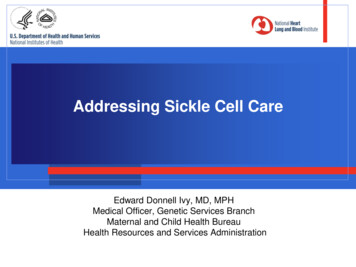
Improving Population HealthBiologicalRiskCreate health promoting ALFAMILYNEIGHBORHOOD, COMMUNITYCultural andSocial NormsModified from Institute ofMedicine. 2010. PromotingCardiovascular Health in theDeveloping World.27SOCIETYImprove Knowledge, Motivation,Skills, BehaviorsCOMMUNITY EDUCATIONAL &BEHAVIORAL PROGRAMSHEALTH CAREDELIVERY& ACCESSHEALTH DETERMINANTSENVIRONMENT & POLICYAPPROACHES
Multi-level Model for ClinicalImplementationSocial, Cultural,Physical EnvironmentsImplementationApproaches &Intervention targetsHealthcare Environment Performance measures (e.g.,HEDIS) Accreditation (JCAHO) Insurance reimbursement (p4p) National clinical guidelinesClinical Institutions CMEs, educational materials, academic detailing Referral & appointment policies Clinical decision support tools eHR reminders, mobile health technology Patient monitoring & feedback to clinicians Local guidelines; national guideline endorsement Local provider incentivesClinicians Tests: screening & diagnosis Treatments & procedures Advice & counseling ReferralsPatient HealthPatients Knowledge Attitudes Behaviors Tx Adherence Risk factors
Principles of Patient-Centered MedicalHome Personal physician - each patienthas an ongoing relationship with apersonal physician provide, continuousand comprehensive care.Physician directed medical practice–leads a team at the practice levelwho take responsibility for the ongoingcare of patients.Whole person orientation –personalphysician responsible for providing allthe patient’s health care needs orarranging appropriate care with otherqualified professionals. This includescare for all stages of life; acute care;chronic care; preventive services; andend of life care. Care is coordinated and/orintegrated across all elements of thecomplex health care systemQuality and safety are hallmarks ofthe medical home:Enhanced access to care is availablethrough open scheduling, expandedhours and new options forcommunicationPayment appropriately recognizes theadded value provided to patients whohave a patient-centered medicalhome.Adapted from HRSA presentation: HRSA Sickle Cell Disease Program, September 2009
30
Increases in Life Expectancy of Patients with Sickle Cell Anemia Life Expectancy (Years) Year 0 10 20 30 40 50 1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000