Transcription
TO:DePauw Student-Athletes and Their FamiliesFROM:Rex Call, LAT, ATC, Director of Sports MedicineDATE:June 1, 2013RE:Sports Medicine and Insurance Information for DePauw Intercollegiate AthletesIn preparation for the upcoming 2013-2014 sport seasons, I would like to provide you with importantinformation regarding your pre-participation medical forms and some additional information on our sportsmedicine services at DePauw University.1. Please carefully review the information and forms in the pre-participation medical packet that youhave received. All forms should be thoroughly and accurately completed and returned no laterthan July 25th. Informational pages in the packet can be retained for reference. No studentathlete will be allowed to participate in practice until all required forms have been submitted andreviewed and medical clearance has been given by DePauw University Sports Medicine.Be aware that the pre-participation medical packet for first year students, transfer students, andDePauw students who are new to DePauw’s intercollegiate program includes The DePauwUniversity Sports Medicine Physical Exam Form. It should be completed by your physicianduring the Summer and prior to your return to campus. Once completed, it should be returnedwith your other pre-participation forms. New student-athletes who do not complete a physical athome during the Summer (or fail to return their completed physical exam form) and have tocomplete the physical exam on campus at the student health service will be charged a healthservice fee. The scheduling of a physical exam at the student health service on check-in day couldresult in a delay in being medically cleared in time for the first practice. For returning DePauwstudent-athletes, you are not required to complete another physical exam. Because aphysical exam is not required after the first year of participation, the DePauw UniversitySports Medicine Physical Exam Form is not part of the returning student-athlete’s preparticipation medical packet.2. Mail all of your completed pre-participation medical forms to: DePauw Sports Medicine,Attention- Medical Records, Lilly Center, 702 S. College Avenue, Greencastle, Indiana 46135.(We ask that you do not return the forms by fax or e-mail.)3. Student-athletes must be covered by a primary medical insurance plan to participate inintercollegiate athletics at DePauw. Your primary medical insurance coverage must be payableup to a benefit of not less than 10,000 for injuries arising out of practice for or participation inintercollegiate sports. If you do not have primary medical insurance coverage, or your currentmedical coverage does not cover intercollegiate athletics, or does not meet the minimal coveragerequirement above, you will need to purchase coverage prior to starting your intercollegiate sportparticipation at DePauw (Please note that out of state Medicaid insurance programs typically donot meet the requirement above). A student-athlete will not be allowed to participate in anyorganized team activity until documentation of primary medical insurance coverage and a frontand back copy of your medical insurance card are provided in the medical insurance section ofyour Part1 Form.
Page 24. The Athletic Department does carry a secondary insurance policy on student-athletes. Coverageis subject to specific policy terms and conditions and includes certain restrictions and exclusionsof which you should be aware. DePauw secondary insurance policy information is available /sports-medicine/insurance/. Please also notethat the NCAA’s Catastrophic Injury Insurance Program covers student-athletes who arecatastrophically injured while participating in a covered intercollegiate athletic activity (subject toall policy terms and conditions). The policy has a 90,000.00 deductible and is supplementalcoverage in the event of a catastrophic injury. More information on this program can be found onthe NCAA’s web-site at: www.ncaa.org5. Almost all sports medicine services provided in the DePauw athletic training rooms by theDePauw Sports Medicine staff are at no cost to the student-athlete. Please note that individualinjury support devices (whether preventative or post-injury) such as customized braces,preventative knee braces, and orthotics are examples of expenses that are a student-athlete’sresponsibility. Office visits to the DePauw Student Health Service are covered under the studenthealth fee assessed to each student for the school year. There are some procedures/services at thehealth services, such as x-rays, lab work, and post-concussion computer (impact) testing that arenot covered by the student health fee (see student health services web page). Off campus care bythe team orthopedic doctor or care by any off campus medical provider or facility includingdiagnostic tests are the financial responsibility of the student-athlete.6. For your information, the DePauw Athletic Department office phone number is 765-658-4012and the Sports Medicine staff contact information is listed below. Have an enjoyable summerand we will look forward to seeing you in the fall !Campus Sports Medicine Staff:Scott Ripple, M.D.Team PhysicianDePauw University Wellness CenterGreencastle, IN 46135Office: 765-658-4555Roger Doan, LAT, ATC, CSCSAthletic Trainer-Soccer, Track, SwimmingLilly Center-DePauw Universityrdortch@depauw.eduOffice: 765-658-4939Rex Call, LAT, ATCDirector Sports MedicineAthletic Trainer: FB, SoftballLilly Center-DePauw Universityrcall@depauw.eduOffice: 765-658-4937Kara Campbell, LAT, ATCAthletic Trainer-CC, F.Hockey, W. Basketball, W. LacrosseLilly Center-DePauw Universitykaracampbell@depauw.eduOffice: 765-658-4968TBAGraduate Assistant Athletic TrainerVB, Tennis, Golf, BaseballOffice: 765-658-4983Sunku Kwon, LAT, ATCAthletic Trainer-Ass’t FB, M. Basketball, M. LacrosseLilly Center-DePauw Universitysunkukwon@depauw.eduOffice:765-658-4953
DePauw University Sports Medicine2013‐2014Pre‐Participation Medical Information and FormsforFirst Year Student‐Athletes, Transfer Student‐Athletes,or DePauw Students New to DePauw’s Intercollegiate ProgramStudent‐Athlete Information and Forms (Completed by Student‐Athlete)Part 1‐Part 2‐Part 3‐Part 4‐Part 5‐Student‐Athlete Information FormMedical History FormSignature Page FormDocumentation of Sickle Cell Trait Status Information and FormNCAA Banned Drugs and Medical Exceptions InformationIf you are taking a prescription medication with a banned substance in it (e.g. ADHD medicationcontaining a stimulant) , please carefully review Part 5 for information on the additionaldocumentation that you will need to submit for your DePauw sports medicine file.Part 6‐ Travel Form‐Emergency InformationTo be Completed by a PhysicianPart 7‐ Physical Exam FormComplete and Mail Forms by July 25th to:DePauw Sports MedicineAttention‐ Medical RecordsLilly Center‐ 702 S. College AvenueGreencastle, IN 46135(Please do not return completed forms by e‐mail or Fax)
Part 1Student-Athlete InformationALL INFORMATION YOU PROVIDE ON THESE FORMS IS CONFIDENTIAL AND WILL BE AVAILABLE ONLY AS AUTHORIZEDLast Name First Name M.I. Sport(s)DePauw E‐Mail Cell Phone UB Mailbox #Class of DOB: Age: Country of Birth Sex: M FDPU Address: Permanent Address:Family Doctor/PCP Phone: E‐Mail:Who should we contact in the event of an emergency ?Parent/Guardian Phone: Cell Phone E‐MailParent/Guardian Phone: Cell Phone E‐MailMedical Insurance Information(Insurance Required for Participation in Intercollegiate Athletics)I attest that I have primary medical insurance coverage under a current in-force insurance policy for injuries thatoccur during my participation in intercollegiate athletics that is payable up to a benefit of not less than 10,000 forinjuries arising out of practice or or participation in intercollegiate sports. If there is a material change in coverageor expiration of coverage, I agree to notify DePauw University of this development and update the insuranceinformation I have on file with DePauw University. I understand that DePauw obtains secondary insurancecoverage through Student Athletic Protection, Inc. for medical expenses for injuries resulting from participation inintercollegiate athletics, and agree that DePauw has no responsibility whatsoever for the payment of any suchexpenses on my behalf other than those expenses that might be covered through this secondary insurance coverage.(If you do not have primary medical insurance that meets the minimal requirement above or are uninsured, you will need topurchase medical insurance that covers intercollegiate athletics. Please note that out of state Medicaid insurance programstypically do not meet the requirement above.)Student Signature:Date:Parent/Guardian Signature:Date:(Parent or guardian signature required for athletes that enter DePauw before their 18th birthday)Insurance Company Policy Holder:Insurance Company Address: Phone:Policy/ID/group Numbers (specify)Is prior authorization required for medical care ? YesAttach copy of front of insurance card here.NoAttach copy of back of insurance card here.
Part 2Medical HistoryNameSport (s)Do you currently have or have you ever had or experienced any of the following (check all that apply andexplain below):ADHD/ADD (refer to Part 5)AllergiesAnemia/bleeding tisDiabetesEating disorderEpilepsy/seizure disorderFaintingHeadaches/MigrainesHistory in family of unexplainedsudden death before age 50History in family of heart diseaseMenstrual problemsHeart disease/problemsMissing vital/paired organHeart murmurMononucleosisHearing impairmentSickle cell anemia/sickle cell traitHeat-related illnessSkin conditionHepatitis/liver diseaseStinger/burnerHigh blood pressureSudden shortness of breathHIV/Aidsduring exerciseIndigestion/ulcers/digestive problemsSudden unexplained fatigueJaundiceduring exerciseJoint/back/bone/muscle injuryTuberculosisKidney disease/problemsVision differenceMarfan’s syndrome or otherOther (please explain)genetic disordersIf you are taking medication(s) for a medical condition checked above, please list under #7 of Part 21.Please explain any conditions you checked above.2.Please give additional information on major injuries, surgeries, or major illnesses that you have had and thedates which they occurred.3.Concussion History (if applicable):Date SymptomsDays/Weeks to be Cleared for ParticipationImpact / Computer Tested (yes/no)4.Are you currently under the care of a physician ? yes no (if yes, please explain)5.Do you currently have an injury that is unhealed ? yes no (if yes, please explain)6.Has a doctor ever denied or restricted your participation in athletics for any reason ? yes no(if yes, please explain)
Part 2Medical History (Continued)NameSport(s)7. List all prescription and over the counter medications taken on a regular basis and the medical reason.Prescription MedicationsOver The Counter Medications8. List all vitamins and supplements that you take.9. Do you wear (check all that apply) :glassescontactsDate of last vision examdental bracesother dental appliancehearing aidorthoticsbraces or sleeves on any of your joints (explain)DEPAUW SPORTS MEDICINE USE ONLY (New Student-Athlete):Sports Medicine Staff Review: LAT/ATC Signature Date:Notes:Height: Weight:Pulse: BP: Date checked:BP re-check neededFollow-up: BP: Date checked: By:Follow- up needed: Yes NoIf yes: Dr. Thieken OtherReason for follow-up:Follow-up completion notes/signature/date:Cleared for Participation : Yes NoNote:Scott Ripple, M.D. Date:
Part 3NameSport(s)Authorization for Release of Medical Information:I give my permission to the DePauw University Sports Medicine physicians and the athletic training staff and other health careproviders employed/affiliated with DePauw University to release my medical information to (1) other health care professionals orproviders to which I may be referred for evaluation and treatment, (2) DePauw Health Services, (3) DePauw Disability Services(3) DePauw Athletic Department personnel, and (4) DePauw’s secondary insurance carrier- Student Athletic Protection, Inc.I also give permission for DePauw Sports Medicine personnel to disclose medical information to the following individual(s):check next to where permission is given Mother Father Other (specify)This authorization for release of medical information is valid for one year from the date signed. If I decide to revoke thisauthorization, I must do so in writing and will contact the Director of Sports Medicine to do so.Student Signature DateParent or Guardian Signature Date(Parent or guardian signature required for athletes that enter DePauw before their 18th birthday.)Acceptance of Risk and Release:I realize that participation in intercollegiate athletics involves the potential for injury, including death, and that even with goodcoaching, training and equipment, injuries can and will occur. In consideration of DePauw allowing me to participate inintercollegiate athletics, I hereby accept the risk of any injury, including death, that might arise from such participation, andhereby release and discharge DePauw and its officers, employees, trustees and their successors and assigns, of and from anyliability, cost, expense or damage, including attorneys’ fees, arising out of my participation and any injuries sustained by me,including death.Student SignatureDateParent or Guardian SignatureDate(Parent or guardian signature required for athletes that enter DePauw before their 18th birthday.)Authorization for Medical Treatment:I hereby authorize the DePauw University Sports Medicine Staff and team physicians, as well as those healthcare personneldesignated by them, to evaluate and treat any injuries/illnesses as they deem necessary to my health and well being as a result ofany injuries/illnesses that occur during athletic participation at DePauw. If the Sports Medicine staff or those designated areunable to communicate with me, the treatment deemed necessary for my health may be given.Student Signature DateParent or Guardian SignatureDate(Parent or guardian signature required for athletes that enter DePauw before their 18th birthday.)Agreement to Report Injuries:I accept the responsibility for reporting my injuries and illnesses to the DePauw Sports Medicine Staff, including signs andsymptoms of concussion.Student Signature Date
Part 4-InformationPOLICY ON SCREENING FOR SICKLE CELL TRAITSickle cell trait is an inherited disorder of hemoglobin in the blood that can cause serious medicalproblems during intense exercise if precautions are not taken. In recent months, the membership ofNCAA Division III passed new documentation requirements pertaining to confirmation of sickle cell traitstatus. The New NCAA requirements go into effect for the 2013-2014 school year. In implementing thispolicy at DePauw University, on a one time basis all student-athletes (both new and returning) will need tosubmit appropriate documentation showing compliance with the new requirement. Because therequirements are similar to providing proof of a medical exam by a licensed physician or providing proofof insurance coverage prior to participation, sickle cell trait documentation is a component of the preparticipation medical screening information. Information on sickle cell trait is available on our SportsMedicine Website at: edicine/safeguards/sickle-cell/and includes a website (National Newborn Screening and Global Resource Center) that could be apotential source for obtaining your newborn test results. Please note that a student-athlete will not beallowed to participate in any physical activity associated with an intercollegiate team until sicklecell trait status or the waiver is on file with our sports medicine staff.Student-athletes at DePauw University can choose to meet the new requirement in one of three ways:1. Elect not to confirm sickle cell trait status. In which case the student-athlete will be required tosign a waiver releasing DePauw University, its officers, employees, and agents from any and allcosts, liability, expense claims, demands or causes of action on account of any loss or personalinjury that might result from the individual’s decision not to confirm or determine their sickle celltrait status. Note: Student-athlete’s whose test results are pending or have not been submittedprior to the first official team practice will also be required to sign the waiver in order to be clearedfor participation.2. Submit a copy of a prior sickle cell trait test with results. You can contact the primary carephysician or the pediatrician who saw you as a newborn or see your personal physician forguidance. Our research indicates that sickle cell trait screening is a routine part of newbornscreening for babies born in U.S. hospitals and in U.S. military hospitals. However, there can bedifficulties in obtaining those test results.3. If no sickle cell trait test report is available, you have difficulty getting your documentation, or youdo not think you were tested, you can request to have a blood test done for sickle cell trait. If youchoose to have a blood test, we highly recommend that you complete this with your primary carephysician at home. You can then submit a copy of your test results at the same time you submityour other pre-participation medical forms which are due by July 25th. Please note that theDePauw University Health Service charges a fee for the blood test and results take approximately3-5 days.The NCAA and DePauw University highly recommend that all student-athletes know their “status” withrespect to sickle cell trait. All student-athletes at DePauw regardless of whether “status” is known or thestudent-athlete has chosen to sign the waiver will receive pre-season education on sickle cell trait.Individuals who have tested positive for sickle cell trait can participate in athletics but must meetwith the team physician to discuss sickle cell trait and to review safety precautions that should be takenduring athletic participation. If you have questions about this new requirement, please contact ourDirector of Sports Medicine, Rex Call, at 765-658-4937 (rcall@depauw.edu) or Dr. Scott Ripple, TeamPhysician, at 765-658-4555 (sripple@depauw.edu).
Part 4Sickle Cell Trait Information and Documentation of Sickle Cell Trait StatusAn NCAA fact sheet for student-athletes has been provided with this form and additional informationon sickle cell trait is available on the DePauw Sports Medicine Web Page s/sports-medicine/safeguards/sickle-cell/Please review the information and check one of the boxes below indicating how you will meet theNCAA sickle cell trait documentation requirement and then sign and date. This form should bereturned with your other pre-participation forms. I do not wish to confirm my sickle cell trait status and have completed the waiver below.I, , understand and acknowledge that DePauw University and theNCAA recommends that all athletes have knowledge of their sickle cell status. Additionally, I have readand fully understand the aforementioned facts and the University policy about sickle cell trait and sicklecell trait testing. I hereby affirm that I have fully disclosed in writing any prior medical history and/orknowledge of sickle cell trait status to DePauw University Sports Medicine and Health Service personnel.I do not wish to confirm my sickle cell trait status and I voluntarily agree to release, discharge, indemnify,and hold harmless DePauw University, its officers, employees, agents, and their successors and assignsfrom any and all costs, claims, damages or expenses, including attorneys fees, arising from any loss orpersonal injury that might result from my refusal to confirm my status. If after signing this waiver, at alater date I confirm my sickle cell trait status, I agree to submit documentation of my test results toDePauw University. I have read and signed this document with full knowledge of its significance. Ifurther state that I am at least 18 years of age and competent to sign this waiver.Student-Athlete’s SignaturePrint NameSportParent/Guardian’s Signature(if under 18 years of age)Print Name DateDateI have attached a copy of my newborn test results or other previous test results for sicklecell trait to this form.Student- Athlete’s SignaturePrint NameSportParent/Guardian’s Signature(if under 18 years of age)Print Name DateDateI am going to confirm my sickle cell trait status by having a blood test done and/or willsubmit a copy of my test results to DePauw Sports Medicine when the results are available.I understand that if my test results are pending or have not been submitted prior to the firstofficial practice, I must sign the waiver to be cleared for participation.Student-Athlete’s SignaturePrint NameParent/Guardian’s Signature(if under 18 years of age)Print NameSportDateDate
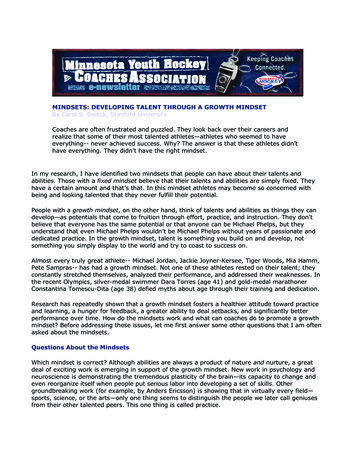
A Fact Sheet for Student-athletesSICKLE CELL TRAITWhat issicklecell trait?Sickle cell trait is not adisease. Sickle cell trait is theinheritance of one gene forsickle hemoglobin and onefor normal hemoglobin. Sicklecell trait will not turn into thedisease. Sickle cell trait is alife-long condition that will notchange over time.u During intense exercise, red blood cells containing thesickle hemoglobin can change shape from round toquarter-moon, or “sickle.”u Sickled red cells may accumulate in the bloodstreamduring intense exercise, blocking normal blood flow tothe tissues and muscles.u During intense exercise, athletes with sickle cell traithave experienced significant physical distress, collapsedand even died.u Heat, dehydration, altitude and asthma can increase therisk for and worsen complications associated with sicklecell trait, even when exercise is not intense.u Athletes with sickle cell trait should not be excluded fromparticipation as precautions can be put into place.Do youknow if youhave sicklecell trait?People at high riskfor having sickle cell traitare those whose ancestorscome from Africa, South orCentral America, India, SaudiArabia and Caribbean andMediterranean countries.u Sickle cell trait occurs in about 8 percent of the U.S.African-American population, and between one in 2,000 toone in 10,000 in the Caucasian population.u Most U.S. states test at birth, but most athletes with sicklecell trait don’t know they have it.u The NCAA recommends that athletics departments confirmthe sickle cell trait status in all student-athletes.u Knowledge of sickle cell trait status can be a gatewayto education and simple precautions that may preventcollapse among athletes with sickle cell trait, allowingyou to thrive in your sport.how can i preventa collapse?u Know your sickle cell trait status.u Engage in a slow and gradual preseasonconditioning regimen.u Build up your intensity slowly while training.u Set your own pace. Use adequate rest and recoverybetween repetitions, especially during “gassers” andintense station or “mat” drills.u Avoid pushing with all-out exertion longer than two tothree minutes without a rest interval or a breather.u If you experience symptoms such as muscle pain,abnormal weakness, undue fatigue or breathlessness,stop the activity immediately and notify your athletictrainer and/or coach.u Stay well hydrated at all times, especially in hot andu Maintain proper asthma management.u Refrain from extreme exercise during acute illness,if feeling ill, or while experiencing a fever.u Beware when adjusting to a change in altitude, e.g., a risein altitude of as little as 2,000 feet. Modify your training andrequest that supplemental oxygen be available to you.u Seek prompt medical care when experiencingunusual physical distress.humid conditions.u Avoid using high-caffeine energy drinks or supplements,or other stimulants, as they may contribute to dehydration.For more information and resources,visit www.NCAA.org/health-safety
Part 5NCAA Documentation Requirements for Student-Athletes Taking a Prescribed MedicationContaining a Banned Substance.Any student-athlete, who for legitimate medical reasons, might be taking a prescribed medication containing a banned substance(see the categories below) should review medical exception procedures to see what supporting medical documentation should bemaintained in their DePauw Sports Medicine file. Refer to Information and Forms for DePauw Student-AthletesTaking aPrescribed Medication Containing a Substance Banned by the NCAA on the DePauw Sports Medicine website which can beaccessed at ports-medicine/forms/. We realize that the majority of studentathletes are not affected by the medical exception policy but awareness is important and you should report any prescriptionmedications that you are taking in Part 2.Applicable Drug Classes Where a Prescribed Medication Could Contain a Banned Substance-diuretics and other masking agents-peptide hormones and analogues-beta 2 Agonists (permitted by prescription and inhalation)-anabolic agents-stimulants (most ADD/ADHD medications contain a banned stimulant)-anti-estrogensADHD MEDICATIONS From the drug classes above, ADHD Medications that contain a banned stimulant are one of the morecommon examples of prescription medications that require supporting medical documentation for the student-athlete’s sportsmedicine file at DePauw. In addition, the NCAA has implemented stricter documentation guidelines (Medical ExceptionProcedures) affecting student-athletes who take an ADHD/ADD medication that contains a stimulant on the NCAA’s banneddrug list. These stricter guidelines involve the procedures to review and approve legitimate use of ADHD medications thatcontain NCAA banned substances. If you are taking an ADHD medication you can access and print off the appropriate ADHDform for your treating physician from our sports medicine web site at: portsmedicine/forms/ If this is the first time that you have submitted your documentation, please use the NCAA Medical ExceptionDocumentation Reporting Form to Support the Diagnosis of Attention Deficit Hyperactivity Disorder (ADHD) andTreatment with Banned Stimulant Medication which can be used by the physician who manages your ADHD care as aguideline for the supporting medical documentation that should be submitted to DePauw Sports Medicine. It may also be helpfulto you and your physician to print off and review the NCAA Medical Exception Policy and Reporting Guidelines. We want toparticularly emphasize to student-athletes taking a medication for ADHD that a key part of your documentation will be inclusionof documentation of a comprehensive clinical assessment (past or present) establishing the diagnosis.Once the initial documentation of a comprehensive clinical evaluation is on file with DePauw Sports Medicine, then each yearthereafter only documentation of an annual follow-up with the treating physician will need to be submitted for your DePauw file.The Annual Medical Follow-up Documentation Form for Student-Athletes Taking ADHD Medication with NCAABanned Stimulant Medication can be used by your treating physician as a guideline for completing and documenting an annualfollow-up.ASTHMA INHALERS If you use an inhaled asthma medication, please submit documentation from your treating physicianthat includes diagnosis, course of treatment, and current prescription.DRUG TESTING AT NCAA POST-SEASON CHAMPIONSHIP EVENTS If a student-athlete tests positive at an NCAApost-season championship event for a banned substance in a prescribed medication and the athlete does not have the NCAArequired medical documentation for DePauw to submit, their eligibility would be suspended by the NCAA (there is an appealsprocess). Please consult with the DePauw athletic trainer assigned to your team for any questions pertaining to NCAA MedicalException Policies and Procedures. It is the responsibility of the student-athlete to work with their treating physician incompleting the medical requirements and submitting the appropriate documentation (in advance for their DePauw SportsMedicine file) that would be needed to gain a medical exception if the student-athlete were to test positive at an NCAAPost-Season Championship Event.RESOURCE EXCHANGE CENTER The National Center for Drug Free Sport, provides a Resource Exchange Center (REC)as a helpful source for colleges and student-athletes. The REC is a confidential resource for student-athletes. You may inquireon-line to see if a prescription medication or supplement contains a substance banned by the NCAA. The REC can be accessedat: www.drugfreesport.com/rec. The password needed for Division III student-athletes to use the web site is ncaa3.
Part 6Student-Athlete Travel FormInformation on this form will be used by the sports Medicine Staff and/or your Coaching staff in theevent of an emergency while traveling to, or participating in, an away athletic event.Student-Athlete Information:Date Completed:Name: Sport(s): Birthdate:Campus Address: Cell Phone:
that the NCAA's Catastrophic Injury Insurance Program covers student-athletes who are catastrophically injured while participating in a covered intercollegiate athletic activity (subject to coverage in the event of a catastrophic injury. More information on this program can be found on the NCAA's web-site at: www.ncaa.org 5.