Transcription
Adult Oral Health AssessmentExecutive SummaryNovember 2009Missouri Department of Health and Senior ServicesOffice of Primary Care and Rural HealthOral Health Programwww.dhss.mo.gov/oral health
TABLE OF Appendix15
Adult Oral Health Assessment Executive SummaryINTRODUCTIONIn 2008, the Office of Primary Care and Rural Health (OPCRH), Missouri Department ofHealth and Senior Services (DHSS), was awarded “Grants to Support Oral Health WorkforceActivities” from the Health Resources and Service Administration (HRSA). One component ofthis grant allowed for a statewide assessment to examine the oral health of specific adult populations throughout Missouri. The data collected through this grant opportunity is crucial, as adultand senior populations have largely been excluded from previous oral health surveillance activities due to current operational funding streams solely directed to populations birth to age eighteen. The following specific aims were established for the assessment: To provide a benchmark of the oral health of adult Missourians living independently andseeking services at a meal site/community center. To provide a benchmark of the oral health of adult Missourians requiring living assistanceand thus residing in skilled nursing facilities. To provide a benchmark of the oral health of adult Missourians who are considered uninsuredor under-insured. To identify access to dental care issues related to adult Missourians.The data presented in this report provides a summary of the survey findings. The first sectionwill describe the methods used in completing the assessment. The second section will discuss thefindings of the assessment by population groups and the third section will provide summarization.
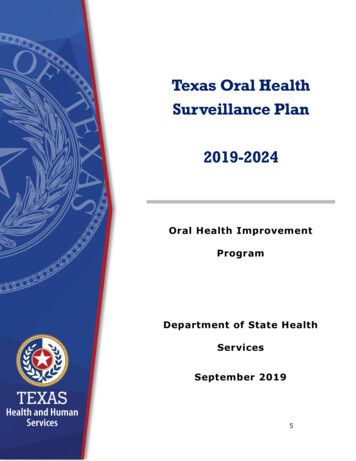
SECTION ONE: METHODOLOGYIn January of 2009 OPCRH contractedwith the University of Missouri Kansas City(UMKC), School of Dentistry to conduct astatewide assessment of adults by specific populations in Missouri. An assessment of this kindhad not been done in any form previously. Thepopulations to be examined included 1) adultsliving independently and seeking services ata meal site/community center sometimes referred to as “well elderly”; 2) adults requiringliving assistance residing in skilled nursing facilities sometimes referred to as “ill elderly” and3) adults who were considered underinsuredand uninsured by virtue of the fact that theysought health and care services through homeless shelters or federally qualified health centers(FHQC).The “Urban-Rural Portion” for each countyin Missouri was obtained using the “MABLE/Geocorr2K: Geographic Correspondence En-gine with Census 2000 Geography” utilityavailable from the Missouri Census Data html). Using the Urban-Rural Portion,the state was stratified into 3 categories: metro( 50% of county population is rural), micro(50-99% of county population is rural), and rural (100% of county population is rural). The494 skilled nursing facilities in Missouri werecategorized as being metro, micro or rural, thentwenty-six facilities were randomly selectedproportional to the number of rural, micro andmetro nursing facilities in the state. To reducetravel costs, a senior meal site in the same community as the randomly selected nursing facilitywas selected.If a nursing facility refused, a replacement facility from the same sampling strata was selected. In addition to the twenty-six skilled nursingfacilities, twenty-five community senior centers,2009 Oral Health Assessment SitesData Source: Missouri Department of Health and Senior Services
eight homeless shelters, and nine federally qualified health centers were selected for the assessments. Assessments at the sites did not includeall clients. Some clients at skilled nursing facilities were not evaluated due to the inabilityto gain access to the mouth or restricted permission from care-givers. At the meal sites theattendance was often impacted by the weather,other competing programs, and type of mealbeing served. The map on the previous page displays the various sites where assessments wereconducted.UMKC recruited and trained a team of thirteen dental hygienists to conduct oral healthscreenings throughout the state of Missouri. Alldental hygienists were licensed in the state ofMissouri and the training session was designedby a dental educator from the UMKC School ofDentistry, Division of Dental Hygiene.Two interview instruments for demographicinformation were developed for this activity.The first instrument was designed for use withthe elderly adults. This included the “well elderly” living independently and seeking servicesat a meal site/community center and the “ill elderly” requiring assistance and living in a skillednursing facility. The second instrument was designed to be used with the underinsured/uninsured adults and was used at the FQHCs andhomeless shelters. These two instruments weredeveloped by a dental educator in collaborationwith the Association of State and TerritorialDental Directors consultant and reviewed forface validity by a team of dental hygiene facultyfrom UMKC.The instruments were identical except for thedepth of interview questions. Typically, the clients at the meal sites and shelters were able to bemore conversant. Thus, the interview questionsassessed for more detail than those questionsasked of the skilled nursing facility clients.Both instruments collected interview information from the subjects as well as intra-oralscreening data. Interview information includeddemographics such as age, ethnicity, type of dental insurance (if applicable) and reason for thelast dental visit. The assessment for the FQHCsand the homeless shelters gathered informationregarding current and past dental pain, types ofservices sought and barriers to dental care. Theassessment for the skilled nursing facilities andthe meal sites/community centers collected dataregarding reasons for past dental visits and alsocategorized the alertness of the individual todiscern for completeness of answers. Copies ofthe interview information can be found in Appendices A and B.All intra-oral screenings were completed usinga pen light and a mouth mirror. Clients wereable to be assessed while in chairs, wheelchairsor while lying in bed. No dental radiographs (xrays) were used. Gauze was used to clear themouth of debris/saliva if oral debris made it difficult to view intra-oral conditions.The screening looked at: the condition of the lips and tonguethe presence of teeth in both archesthe presence and condition of a dentureuntreated decaysevere periodontitis as evidenced by mobilityand visible furcation involvementcandidiasis and other oral lesionssaliva statusoral cleanlinesstreatment urgencyA copy of the intra-oral screening form can befound in Appendix C.The assessments were completed by the trainedhygienist over a period of eight weeks, and thenanalyzed by the ASTDD consultant. DescripOral Health Assessment Summary 3
SECTION TWO: FINDINGSvices at Meal Sites/Community Centers.A total of 1,904 adults were assessed; 1,186individuals in skilled nursing facilities (SNF),464 from meal sites (senior centers), 124 fromhomeless shelters, and 130 at federally qualifiedhealth centers. The results will be reported intwo parts:DEMOGRAPHICS Part One: Key Findings from assessments ofolder adults living in skilled nursing facilitiesand seeking services at meal sites/communitycenters. Part Two: Key Findings from assessments ofadults considered uninsured and underinsured.PART ONE: Key Findings of Oral HealthAssessments of Older Adults Living inSkilled Nursing Facilities or Seeking Ser-The table below describes the demographicsof adults representing the “ill elderly” and the“well elderly” of Missouri. It should be notedthat seventy-three percent of the adults at theskilled nursing facilities and sixty-four percentat meal sites/community centers were female.Of all of the individuals assessed, ninety-fourpercent of the individuals were Caucasian andapproximately ninety percent were over theage of sixty, which is close to the statewidepopulation rate of Caucasians 55 years old andover at ninety-one percent based on the DHSSMissouri Information for Community Assessment (MICA). This assessment did not include any individuals considered home bound.These demographics are illustrated in Table 1.TABLE 1: DEMOGRAPHICS OF SENIORS ASSESSEDIN SKILLED NURSING FACILITIES AND MEAL SITESSkilled Nursing FacilitiesNumber of ParticipantsFemale865 (73%)Male316 (27%)Missing/Unknown5 ( sing/UnknownMeal SitesNumber of Participants298 (64%)164 (35%)2 ( 1%)1108 (93%)59 (5%)7 ( 1%)12 (1%)436 (94%)20 (4%)5 ( 1%)3 (1%)Age Group 5031 (3%)51to6076 (6%)61to70 119 (10%)71to80253 (21%)81to90506 (43%)91 163 (14%)Missing/Unknown38 (3%)9 (2%)15 (3%)109 (24%)178 (38%)137 (30%)15 (3%)1 ( 1%)4 Office of Primary Care and Rural Health
KEY FINDING 1: Many older adults inMissouri are in need of dental care.fourteen percent had severe periodontal disease.This information is illustrated in Table 2.Twenty-four percent of older adults living inskilled nursing facilities reported having seen adentist in the past year. This can be compared tothe more than fifty percent of those assessed atmeal sites/community centers. Twenty-six percent of adults in skilled nursing facilities werein need of either early or urgent dental care. Ofthose, fifteen adults in the skilled nursing facilities (2%) had pain or abscesses requiring urgentcare. This can be compared to almost eighteenpercent of adults assessed at meal sites/community centers required dental care with threeadults (1%) noted with pain and/or abscessesrequiring urgent care. Individuals who werenoted to need early dental care were those withuntreated decay or a need for denture fabrication or repair.Forty-four percent of skilled nursing facilityresidents were assessed as having untreated decay and twenty-two percent having severe periodontal disease (mobile teeth and visible roots).Of the adults assessed at meal sites/communitycenters, twenty percent had untreated decay andKEY FINDING 2: Missouri’s adults havelimited oral function necessary to maintainhealth through proper diet and nutrition.A complete and functioning dentition, whether of one’s own natural teeth or in the formof dentures, is important to maintaining goodhealth through proper nutrition. Table 3 illustrates the percentage of individuals missingteeth (edentulous) in either upper or lower arch,the percentage of those who have dentures, andthe percentage of those dentures that need tobe repaired.It should be noted that not all individualsmissing teeth have those teeth replaced with adenture. Furthermore, of those dentures thatdo exist, twenty-one to thirty-eight percentrequire repair. Having no dentures to replacemissing teeth or having dentures that needrepair leads to loss of function and ultimatelypoor health because of improper diet and nutrition for these individuals.TABLE 2: STATUS OF SENIOR/ADULTS NEED OF DENTAL CAREUntreated Dental DecaySkilled NursingFacilitiesMeal Sites44%20%14%37%17%2% 1%Severe Periodontal Disease22%Required Early Dental CareRequired Urgent Dental CareOral Health Assessment Summary 5
KEY FINDING 3: The oral health of Missouri adults attending senior centers isbetter than that of adults residing in skillednursing facilities.In comparison, findings at senior meal sitesincluded: When screened for oral cleanliness, lesions, orinfection: residents had significant oral debris in theirmouths 77 percent of skilled nursing facility 32 percent of skilled nursing facility residents had dry lips7 percent of skilled nursing facilityresidents had oral lesions4 percent of skilled nursing facility residentshad a yeast infection or candidiasis 43 percent of adults at senior meal sites hadsignificant oral debris in their mouths12 percent of adults at senior meal sites haddry lips5 percent of adults at senior meal sitesexhibited lesions3 percent of the adults at senior mealsites had a yeast infection or candidiasisThis data is displayed in Table 4.TABLE 3: STATUS OF EDENTULOUS IN SKILLED NURSINGFACILITIES AND SENIOR MEAL SITESSkilled NursingMeal Sites/FacilitiesMissing All Upper TeethDenture Replacing the Upper TeethUpper Dentures That Need RepairMissing All Lower TeethDenture Replacing the Lower TeethLower Dentures That Need Repair56%81%21%44%74%34%TABLE 4: ORAL, CLEANLINESS, LESIONS ANDINFECTION STATUSSkilled NursingDry LipsSome Areas With Oral DebrisMost Areas With Oral DebrisDry, Sticky TissuesOral LesionsCandidiasis6 Office of Primary Care and Rural HealthFacilities32%62%15%35%7%4%Community Centers42%95%23%29%90%38%Meal Sites/Community Centers12%42%1%12%5%3%
PART TWO: Key Findings of Oral HealthAssessments of Missouri’s Uninsured andUnderinsuredDEMOGRAPHICSAdults were assessed at homeless shelters andFQHC’s medical clinics to obtain oral healthdata of Missouri’s uninsured and underinsured.Table 5 describes the demographics of thoseadults screened. It should be noted that thirtytwo percent of the adults assessed were femaleand seventy-two percent of the individuals wereCaucasian. The age range of these adults (defined as age 21) was from 21 to 81 .KEY FINDING 1: A large segment ofuninsured and underinsured adults in Missouri are in need of dental care. About one-third (32%) of adults assessed inFQHC’s medical clinics reported having seen adentist in the past year; and of those, only onethird (32%) went in for regular check-ups. Overforty percent of those having seen a dentist inthe past year were seen because there was a specific dental treatment to be remedied such astooth ache relief, broken tooth, or decay. Of the adults assessed in shelters approximately one-quarter (27%) reported a dentalvisit within the past year. Of those, thirty-sixpercent went for a routine check-up and atleast one-third (31%) sought treatment whenprompted by discomfort.TABLE 5: DEMOGRAPHICS OF FQHC’S AND SHELTER PARTICIPANTSGenderFemaleMaleFQHCNumber of ParticipantsSheltersNumber of Participants42 (32%)88 (68%)39 (32%)85 (68%)85 (69%)35 (28%)4 (04%)47 (38%)22 (18%)23 (18%)22 (18%)10 (08%)Race/ethnicityCaucasian97 (75%)African-American23 (18%)Other10 (08%)Age Group 217 (05%)21to3021 (16%)31to4021 (16%)41to5027 (21%)51to6020 (15%)61to7020 (15%)71to8011 (09%)81 2 (02%)Missing/Unknown1 (01%)Note: Percentages may equal more than 100% because of rounding.Oral Health Assessment Summary 7
Both in the FQHC’s and in the sheltersapproximately eleven to fourteen percent ofadults needed urgent treatment This classification of urgent care was assigned when the clientwas experiencing pain or had visible abscesses.These findings are illustrated in Table 6.most one-third of individuals reported nothaving dental insurance and being unable toget dental care in the last twelve months. Thevast majority of these respondents reported alack of affordability as the reason.This finding is illustrated in Table 7.KEY FINDING 2: Uninsured and underinsured adults in Missouri are impacted byaccess issues. KEY FINDING 3: Many of Missouri’s uninsured and underinsured experience limitedoral function necessary to maintain healththrough proper diet and nutrition.Of the adults assessed at the homeless shelters, sixty-nine percent reported having no dental insurance and almost fifty-two percent indicated that dental care had not been possible inthe past twelve months.A complete and functioning dentition, whether of one’s own natural teeth or in the form ofdentures, is important to maintaining goodhealth through proper nutrition. Almost eighteen percent of individuals atAt the federally qualified health centers al-TABLE 6: STATUS OF UNINSURED AND UNDERINSURED NEEDING DENTAL CAREDental Visit Within the Past YearMain Reason for VisitCheck up, exam or cleaningDiscomfortNeeds Early Dental CareNeeds Urgent Dental CareHomeless Shelters27%36%31%29%14%TABLE 7: FINDINGS AND ACCESS TO DENTAL CAREHomeless SheltersNo Dental Insurance69%Could not get dental care whenneeded during the past 12 months52%Reason that dental care could not be securedCould not afford itn 45No Insurancen 34Other Family Needsn 2Note: Participants could select more than one option so percentages are not presented.8 Office of Primary Care and Rural HealthFQHC32%32%40 %37%11%FQHC32%34%n 29n 7
federally qualified health centers are edentulous,i.e. missing all teeth in both arches.However, the encouraging news is that ninetyone percent of those individuals have denturesto replace the dentition.Table 8 illustrates the percentage of individuals missing teeth in either the upper or lowerarch, percent of those that have replacementsin the form of dentures and the percentage ofthose dentures that need to be repaired.Needing a repair or relining is indicative of adenture that is not functional. Therefore, onemust not only consider the number of clientswith dentures, but also the condition of thedentures as well.SUMMARYIn conclusion, the Centers for Disease Controland Prevention (CDC) report that nationallytwenty-five percent of American adults over age60 have lost all their teeth, primarily because oftooth decay, which affects more than ninetypercent of adults over age 40, and advancedgum disease, which affects five-fifteen percentof adults.In addition, oral cancers pose a threat to thehealth of U.S. adults. Healthy People 2010 and2020 documents both address the need for earlydetection of oral cancer. While the picture foradults in general is serious, it is even more critical for seniors and for those adults who are underinsured/uninsured and lack the resources toget dental care.According to the CDC, gum disease is associated with diabetes, and there is emerging evidence of the relationship between periodontaldisease and cardiovascular disease and stroke.TABLE 8: EDENTULOUS IN SHELTERS AND FQHC’S ASSESSMENT SITESCompletely EdentulousMissing All Upper TeethDenture Replacing the Upper TeethUpper Dentures That Need RepairMissing All Lower TeethDenture Replacing the Lower TeethLower Dentures That Need RepairHomeless 8%Note: Percentage of IndividualsOral Health Assessment Summary 9
All of this leads to higher healthcare costs.Oral health problems also result in quality oflife issues for seniors. Poor oral health causesneedless pain and suffering; loss of self-esteem;and difficulty in speaking, chewing and swallowing. Furthermore, loss of function of teethcauses problems associated with poor nutrition.SENIOR MISSOURIANSThe importance of this assessment for the future of senior oral health is underscored by thefact that there is a scarcity of Missouri-specificoral health data for older adults. Without suchdata, effective planning and resource development cannot occur.In Missouri, the percentage of adults in general visiting the dentist in a year is below the national average, while the number of adults 65 having all teeth extracted is above the nationalaverage (Data from Kaiser Family Foundation,2008). The assessment of seniors in skilled nursing facilities and senior centers indicates thatthe number of seniors who have seen a dentistor have had all teeth extracted compares even10 Office of Primary Care and Rural Healthless favorably.In Missouri thirteen percent of the state’s population is age 65 , and of the 771,300 seniors inMissouri, 36,696 or five percent are in skillednursing facilities. According to the CDC, beingdisabled, homebound or institutionalized arerisk factors for poor oral health.It should be noted that in the case of the assessment of seniors at skilled nursing facilitiesthat because of cognitive function, not all ofthose assessed could self-report; seventy-fourpercent of the seniors assessed in skilled nursing facilities were described by the screeners as“alert”, with twenty percent unable to give answers and four percent described as “unaware”.In addition, as was discussed earlier, the screening consisted of a visual examination only, withno dental radiographs or use of instruments.Moreover, the assessment did not includehomebound seniors. This leads to limitations inthe data by virtue of the abilities of the population. Therefore, the actual need for care forseniors in Missouri is underestimated.Given these qualifications, the following com-
parisons to the general adult population and tonational data on seniors can be drawn: Missouri’s seniors are not receiving as muchdental care as the adult population in general.Both groups of seniors assessed in Missouri fallbelow the national average and the state averageof adults overall who have seen a dentist in thepast year. The Kaiser Family Foundation reportsfor 2008, the number of adults nationwide whohave seen a dentist in the past year is seventyone percent. In Missouri, among the generaladult population, the Kaiser Family Foundationreports for 2008 that sixty-three percent visiteda dentist in the past year. Moreover, the results for Missouri seniorsin nursing homes do not compare favorablywith national data on seniors. According to theMedical Expenditure Panel Survey (MEPS)2006, forty-nine percent of those age 60-69 hadat least one dental visit in the past year; fortyfive percent of those age 70-79 had at least onedental visit in the past year; and among those80 and older, thirty-seven percent had a dentalvisit in the past year.Of those seniors assessed in skilled nursing facilities, forty-four percent had untreated decay;and of those assessed in senior centers, twentypercent had untreated decay. Nationally, according to the NHANES 1999-2002 Survey,nineteen percent of those ages 60 and over haddental caries. The CDC suggests that olderadults may have new tooth decay at higher ratesthan children.Of those seniors assessed in skilled nursingfacilities, twenty-two percent had severe periodontitis. This number mirrors the findings ofthe CDC which estimates that twenty-threepercent of adults 65-74 have severe periodontaldisease. Seniors assessed at the meal sites, exhibited less severe periodontitis with fourteenpercent.Compared to seniors who attend meal sites,residents of skilled nursing facilities are statistically older, are medically compromised andOral Health Assessment Summary 11
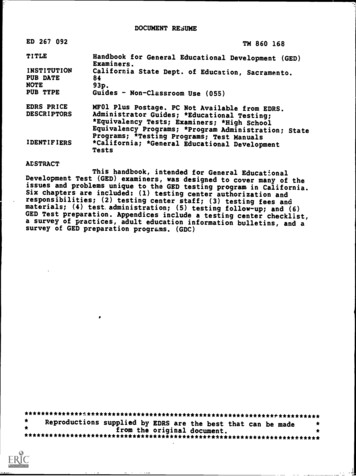
more frail. Therefore, findings illustrate that theoral health of residents of skilled nursing facilities tends to be worse.According to the CDC, many of the medications taken by seniors can cause dry mouth andreduction of the flow of saliva increased the riskof oral disease. On average, the CDC estimatesindividuals in skilled nursing facilities take anaverage of eight drugs per day.More Missouri seniors are missing all teeththan are seniors nationally. More than fortypercent of seniors in the skilled nursing facilities were edentulous in both arches; and closeto thirty percent of the seniors at the meal siteswere missing all teeth.MEPS 2006 reports that nationally, of those60-69, sixteen percent are edentulous in botharches; among those 70-79, twenty-five percentare; and among those 80 and over, thirty percent are missing all teeth.Approximately forty percent of the seniors12 Office of Primary Care and Rural Healthassessed in skilled nursing facilities need treatment – either early care or urgent care, as determined by the screeners.UNISURED MISSOURIANSThe following facts underscore the access problem for many adults: Two-thirds of adults in the shelters reportedhaving no dental insurance. Approximately half of adults in the sheltersreported that dental care had not been possiblein the past twelve months. Almost one-third of individuals at theFQHC’s reported not having dental insurance. Almost one-third of individuals at the
FQHC’s reported not being able to get dental care in the last twelve months; and the vastmajority of these respondents reported a lack ofaffordability.The impact of the access problem is demonstrated in their oral health. Of the individualsassessed at FQHC’s forty-one percent had untreated decay; this percentage was higher stillamong residents of shelters, with forty-ninepercent having untreated decay. These averagesare twice the numbers reported nationally. According to the NHANES 1999-2002 Survey,twenty-three percent of those age 20 and uphad decay.Approximately one-quarter (26%) of FQHCclients had severe periodontitis, while sevenpercent of residents in shelters exhibited severeperiodontal disease. These results were probablyimpacted by the fact that the population in theshelters was much younger on the whole thanthose assessed in the FQHCs.Of the FQHC clients assessed, eighteen percent were edentulous in both arches. NHANESdata (1988-1994) reported ten percent of adultsage 18 and above nationally reported completetooth loss.NEXT STEPSThe objectives of the oral health assessmentwere: To provide a benchmark of the oral healthof adult Missourians living independently andseeking services at a meal site/community center. To provide a benchmark of the oral healthof adult Missourians requiring living assistanceand thus residing in skilled nursing facilities. ADULTS MISSING ALL TEETHUntreated DecayOral Health Assessment Summary 13
To provide a benchmark of the oral healthof adult Missourians who are considered uninsured or underinsured. To identify access to dental care issues related to adult Missourians.Establishing this baseline data was the first step.The next step is for appropriate groups, such aspublic health specialists, oral health professionals, legislators and policy-makers to review thedata and design the strategies to address the oralhealth of Missouri adults, especially the vulnerable populations.Through the collaboration of the Oral HealthTask Force in 2009, a Statewide Oral HealthPlan was developed. The implementation ofthe Plan will be further discussed by a steeringcommittee which grew out of the Task Force.This assessment data should serve as a valuableresource for the Steering Committee as theydesign oral health programs and services.14 Office of Primary Care and Rural HealthACKNOWLEDGEMENTSThis assessment was developed and implemented by a group of dedicated health professionals.The Department of Health and Senior Services (DHSS) would like to thank the Oral HealthAssessment Team, the University of Missouri Kansas City School of Dentistry, and the ASTDD consultant.Also, DHSS would like to acknowledge withgratitude the participation of twenty-six skillednursing facilities, twenty-five senior sites, nineFederally Qualified Health Centers, and eighthomeless shelters that helped to make this assessment possible.
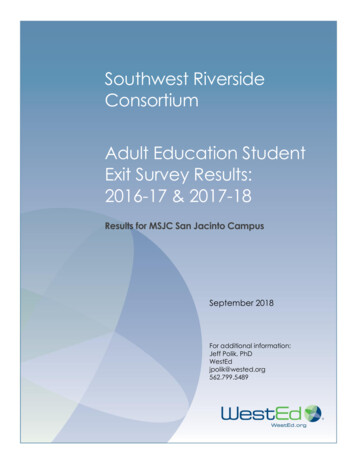
Oral Health Assessment Summary 1581-90NoneArmed Forces34Private insurance2DENTAL INSURANCE/COVERAGE:1 MedicaidnoSEEN A DENTIST IN PAST YEAR:1 yesUnaware of the screeningUnable to give reliable answersOther (please explain)Tooth extraction34Toothache/pain2IF YES, WHY:1 Routine cleaning/exam35 91-100 2Other5RESPONSE STATUS:1 male22ETHNICITY:1 African-American61-702AGE:1 51-60/ /SURVEY DATE:GENDER:1 MaleZip codeCLIENT #:NAME OF FACILITY/AGENCY:APPENDIX A: SKILLED NURSING FACILITY AND MEAL SITE ORAL HEALTH ASSESSMENT
16 Office of Primary Care and Rural HealthMedicaid/MedicareNoYesDo you have dental insurance?Medicaid/MedicareNoYesDo you have medicalinsurance?Zip CodeNAME OFFACILITY/AGENCY:/ /Was called in by the dentist forcheck-up, examination or cleaning.OtherDon’t know/don’t remembere.f.d. Went for treatment of a conditionthat dentist discovered at earliercheck-upc. Something was wrong, bothering orhurting.b.a. Went in on own for check-up,examination or cleaning.What was the main reason that you lastvisited a dentist? (Please check one)a. Nob. Yesc. Don’t know/don’t rememberDuring the past 6 months, did you have atoothache more than once, when biting orchewing?SURVEY DATE:CLIENT #:c. Don’t know/don’trememberb. Yesa. Noa. Could not afford itb. No insurancec. Did not accept Medicaidd. Not serious enoughe. Wait too long in clinic/officef. Difficulty getting appointmentg. Don’t like/trust dentistsh. No dentist availablei. Didn’t know where to goj. No way to get therek. Hours not convenientl. Speak a different languagem. Other family needsn. Other reasono Don’t know/don’t remembera. 6 months or lessb. More than 6 months, but not more than 1 year agoc. More than 1 year ago, but not more than 3 years agod. More than 3 years agoe. Never have beenf. Don’t know/don’t rememberDuring the past 12 months, The last time you could not get thewas there a time when youdental care you needed, what was theneeded dental care butmain reason you couldn’t get care?could not get it at that time? (Please circle one)GENDER:ETHNICITY:1 African-American1 Male2 Caucasian3 Hispanic2 Female4 Asian5 OtherAbout how long has it been since you last visited a dentist? Includeall types of dentists, such as, orthodontists, oral surgeons, and allother dental specialists, as well as dental hygienists.AGE:APPENDIX B: FQHC AND SHELTER ORAL HEALTH ASSESSMENT
Oral Health Assessment Summary 17MANDIBULAR DENTURE STATUS:1 OK - can use as is2 Needs repair/reline to be functional3 NA – has natural teethORAL CLEANLINESS:1 Clean mouth/dentures2 Food, calculus, materia alba in some areas of mouth/dentures3 Food, calculus, materia alba in most areas of the mouth or ondentures; bridges of calculus severe bad breath.SALIVA:1 Moist tissues, watery & free-flowing saliva2 Dry, sticky tissues, little saliva or saliva very thick-ropey3 Tissues parched and red, very little/no saliva presentTREATMENT URGENCY:1 No obvious problems – should receive regular dental care2 Early dental care needed – before next
skilled nursing facilities reported having seen a dentist in the past year. This can be compared to the more than fifty percent of those assessed at meal sites/community centers. Twenty-six per-cent of adults in skilled nursing facilities were in need of either early or urgent dental care. Of those, fifteen adults in the skilled nursing facili-