Transcription
Government of the District of ColumbiaAnthony A. Williams, MayorFirst Citywide ComprehensiveSubstance Abuse Strategyfor the District of ColumbiaSeptember 2003PRESENTED BY THEMAYOR'S INTERAGENCY TASK FORCEON SUBSTANCE ABUSE PREVENTION, TREATMENT & CONTROLJames A. BufordTask Force ChairChief Charles H. RamseyTask Force Co-Chair
The Mayor’s Interagency Task Force on Substance AbusePrevention, Treatment and ControlTA S K F O RC E M E M B E R SJames A. BufordChief Charles H. RamseyNeil AlbertPeggy Cooper CafritzFernando Daniels III, M.D.Yvonne GilchristOlivia GoldenCarolyn GrahamHon. Anita Josey-HerringMargaret KellemsMartha KnisleyJohn KoskinenJasper OrmondEric PricePatricia RileyAdrian ThompsonCaptain James ThompsonDr. Paul VanceOdie WashingtonNancy WareTask Force Chair, Director, Department of HealthTask Force Co-Chair, Chief of Police Metropolitan Police DepartmentDirector, Department of Parks and RecreationPresident, DC School BoardMedical Director, DC Fire and Emergency Medical ServicesDirector, Department of Human ServicesDirector, Child and Family ServicesDeputy Mayor for Children, Youth, Families, and EldersJudge, DC Superior Court/Office of Corporation Counsel/Criminal/JuvenileDeputy Mayor for Public Safety and JusticeDirector, Department of Mental HealthCity Administrator and Deputy MayorCourt Services and Offender Supervision AgencyDeputy Mayor for Economic DevelopmentSpecial Counsel to the U.S. AttorneyChief, DC Fire and Emergency Medical ServicesDirector, Mayor’s Office of Health PolicySuperintendent, DC Public SchoolsDirector, DC Department of CorrectionsDirector, Criminal Justice Coordinating CouncilA S S O C I A T E TA S K F O RC E M E M B E R SNiquelle AllenSampson AnnanPatrick CanavanLeslie CombsPhyllis Kaiser-DarkBrenda DonaldMichael J. DuBoseRogue GeraldLinda HolifieldWanda JohnsonMark JordanNola JoyceMoses McAllisterJames MillerLaTonya MoorePeter ParhamDave RosenthalAttorney, Alcohol Beverage Regulatory AuthorityDirector of Research and Resource Development, Metropolitan Police DepartmentDirector, Neighborhood Service Coordinators, Office of the City AdministratorProgram Analyst, Court Services and Offender SupervisionExecutive Assistant to the City AdministratorChief of Staff, Child and Family Services AgencyPublic Health Educator, DC Department of CorrectionsDirector, Clinical Services, Child and Family ServicesSpecial Assistant to the Director, Department of HealthDeputy Director, Mayor’s Health Policy CouncilChief of Staff, Office of the Deputy Mayor for Public SafetySenior Executive Director, Office of Organizational Development, Metropolitan PoliceDepartmentDirector, Social Services Division, DC Superior CourtDeputy Fire Chief Executive Officer, Fire and Emergency Medical ServicesSubstance Abuse Specialist, Child and Family Services AdministrationDirector, Interagency Partnerships, District of Columbia Public SchoolsActing Deputy of Corporation Counsel, Criminal Divisioni
A D D I C T I O N P R E V E N T I O N A N D R E C OV E RY A D M I N I S T R A T I O N S TA F FWilliam StewardConstance BushNatleen ChanceLinda Y. FisherJanet PerkinsWendy Thamani SalaamCarol WareInterim Deputy Director of Substance Abuse ServiceDirector, State Incentive GrantsExecutive Assistant to the Senior Deputy Director for Substance AbuseChief, Office of Prevention and Youth ServicesDeputy Director for Policy and ResearchChief, Office of Public PolicyChief Administrative OfficerC A R N E VA L E A S S O C I A T E S , L L CJohn CarnevaleJen BaffiScott ChronisterNancy DudleyBrad HartPat MurphyRobert WarshawPrimary ConsultantConsulting TeamConsulting TeamConsulting TeamConsulting TeamConsulting TeamConsulting Teamii
The First Citywide ComprehensiveSubstance Abuse Strategy for theDistrict of ColumbiaTA B L E O F C O N T E N T SChapter 1:INTRODUCTION . 1-1Chapter 2:THE DIMENSION OF THE DISTRICT’S SUBSTANCE ABUSE PROBLEM . 2-1Chapter 3:THE DISTRICT’S SUBSTANCE ABUSE PROGRAMS AND BUDGETS. 3-1Chapter 4:STRATEGIC GOALS AND OBJECTIVES . 4-1Chapter 5:POLICY AND PROGRAM PRIORITIES . 5-1Chapter 6:CONCLUSION . 6-1References . R-1Appendix A:SUBSTANCE ABUSE-RELATED DATA FOR THE DISTRICT OF COLUMBIA . A-1Appendix B:CONSULTATION LIST. B-1Appendix CINVENTORY OF SUBSTANCE ABUSE-RELATED PROGRAMS AND RESOURCES . C-1iii
L I S T O F TA B L E SChapter 2Figure 1 1.2 Billion in Social Costs of Alcohol and Drug Abuse in the District of ColumbiaTable 1Percentage Reporting Substance Abuse on a Past-Month BasisTable 2Percentage Reporting Past Year Dependence in the District Compared with the U.S.Table 3Treatment Admissions in the DistrictTable 4Reported Crimes in the District, 1993-2002Table 5Arrests for Index Crimes in the District, 1996-2000Table 6Substance Abuse Arrests, 1996-2000Table 7Hospital Emergency Room Episodes and Drug Mentions for Illicit Drug UseTable 8Past-Month Use of Alcohol, Tobacco, and Illicit Drugs, by WardChapter 3Table 1Substance Abuse Program ExpendituresFigure 1Substance Abuse Expenditures by Focus of ProgramTable 2District of Columbia Substance Abuse Program Funding, FY 2003–FY 2004Table 3Federal Substance Abuse Program Expenditures, FY 2003–FY 2004Table 4Funding by Functional Area, FY 2003Table 5Substance Abuse Arrests, 1998–2002Table 6DC Substance Abuse Expenditures–Summary TablesChapter 4Figure 1Ten-Year Target for AddictionFigure 2Ten-Year Target for Social CostsFigure 3Ten-Year Targets for Youth Substance UseFigure 4Ten-Year Targets for Youth Substance Use InitiationChapter 6Figure 1Timeline for Strategy Development and ImplementationAppendix BTable 1DC Substance Abuse Expenditures–Agency Tablesiv
Chapter 1INTRODUCTIONA S U B S TA N C E A BU S E S T R A T E G Y F O R T H E D I S T R I C T O F C O L U M B I AThe statistics on substance abuse amongthe residents of the District of Columbia (theDistrict) are disturbing. Approximately 60,000residents--nearly one in 10--are addicted toillegal drugs or alcohol. Of the 1.3 millionemergency room visits in the District, about40 percent are related to drug and alcoholabuse. Fifty percent of the reported motorvehicle crashes in the District are associatedwith substance abuse. Nearly 15 percent ofnew mothers report having used illicit drugsduring pregnancy. Eighty-five percent offoster care placements are connected withsubstance abuse. Twenty-seven percent of thecumulative reported AIDS cases in theDistrict are related to intravenous drug use.And one source estimates that the social costsof drug and alcohol abuse to the District aremore than 1.2 billion. Adding tobaccorelated social costs raises this figure to morethan 1.7 billion.These troubling statistics, however, mustbe viewed against a larger background, onethat includes the overall positive strides thathave been made in recent years by the city.The District of Columbia has achieved realprogress in reducing drug-related crime andviolence in the past decade and in makingneighborhoods safer and more secure.Efforts to restore its fiscal health andeconomic vitality are attracting new residentsand businesses. Not all of the news is good,however, in particular the recent resurgenceof homicides in the District.Much of the District’s progress so far isdue, in part, to ongoing efforts to prevent,treat, and control substance abuse. Thecocaine epidemic that ravaged the city forover two decades and nearly destroyed ageneration of the District’s youth hassubsided. Today, rates of cocaine use by youthare low. Although no one can deny progress,serious hurdles remain, chief among them theneed to close the “treatment gap” between thecity’s drug treatment capacity and the numberof individuals requiring help. Equallyimportant is the need to continue a strongsubstance abuse prevention effort that willenable District youth to make healthy lifestylechoices. If the District is to become thecapital city that every American can feel proudof, then recent positive strides againstsubstance abuse must continue.THE MAYOR’S TASK FORCEIn response to the impact of substanceabuse on the District’s health, safety, andfinancial stability, Mayor Anthony A. Williamsappointed an executive-level task force toprepare and recommend the citywide“A Substance Abuse Strategy for the District mustrepresent a firm commitment to address both the publicsafety and public health aspects of the problem.”– DC Mayor Anthony A. WilliamsSubstance Abuse Strategy (Strategy) andbudget. In May of 2001, the mayor establishedthe Interagency Task Force on SubstanceAbuse Prevention, Treatment, and Control(the Task Force) and formally commissionedthe group to oversee the District’s substanceabuse policies and interagency andintergovernmental substance abuse activities.According to the mayor’s order, the TaskForce is charged with “enhancing theeffectiveness of the city’s health, socialservice, and criminal justice system bymonitoring use of federal grant fundingtogether with local funding to implementinnovative substance abuse programs.”Furthermore, the mayor’s order requires the
Task Force to “establish well-definedperformance outcome measures that willfacilitate an assessment of costs and benefitsin investments in substance abuse prevention,treatment and control.”Police Department Chief Charles H. Ramseyare working in close collaboration with themayor’s staff to ensure a comprehensive lineof attack.THE SCOPE OF THE PROBLEMA COMPREHENSIVE STRATEGYFor the past year the Task Force hasworked closely with the mayor’s staff as wellas with a wide variety of experts andstakeholders to develop a Substance AbuseStrategy that is both accountable to taxpayersand well coordinated with existing Districtagency plans and budgets. At a minimum, theStrategy is designed to address two enormousand perhaps ambitious challenges: reducingthe city’s addicted population by 25,000 andreducing the social costs of substance abuseby 300 million by the year 2010. In addition,the Task Force has also identified policies toaddress substance abuse among Districtyouth, to close the gap between the numbersof individuals requiring treatment and theservicesavailable,andtoenhancecoordination between city and federalagencies.“The mayor and the Task Force are committed to astrategic plan with the built-in support of a widecommunity of stakeholders.”-- Metropolitan PoliceDepartment Chief Charles H. RamseyFrom the outset, the mayor’s approach todeveloping the Substance Abuse Strategy forthe District has represented a firmcommitment to address both public safetyand public health aspects of substance abuse.Clearly, District residents are entitled toprotection from any unlawful behaviors,including those of drug offenders. And drugaddicts--as individuals suffering from achronic, relapsing brain disease--requirecomprehensive, effective treatment.The mayor’s selection of Task Forceleadership reflects his balanced approach tothe issue.D.C. Department of HealthDirector James A. Buford and Metropolitan1-2Recent data make it clear that the city’ssubstance abuse problem as a whole is farmore extensive than previously recognized. InDecember of 2000, the DC Department ofHealth engaged Westcom International, Ltd.,toconductthenation’sfirst-ever,“The Strategy presented here represents our collective willto aggressively target addiction, so our citizens can enjoyhealthy and productive lives.” – D.C. Department ofHealth Director James A. Bufordcomprehensive citywide household survey onsubstance abuse. The results of the survey of1,535 District households reveal startlinginformation. For illegal drugs alone, the rateof addiction in DC is nearly 40 percent higherthan the rate of addiction for the nation thatsame year. Nine percent of District residentsreport a dependence on drugs and alcohol,compared with a national estimate of 4.8percent identified by the federal government’s2000 National Household Survey on DrugAbuse. Furthermore, the survey’s addictionrates are considered to be conservativebecause, like all household surveys, the DCHousehold Survey excludes institutionalizedand homeless populations. Moreover, one outof six adolescents–children between 12 and 17years old–reported having consumed alcoholin the month leading up to the survey.Twenty-onepercentofadolescentrespondents had used an illicit drug in the pastyear, and 7 percent reported using an illicitdrug within the past month.At the mayor’s request, the Task Forceconducted an analysis of the District’s drugprograms and governmental expenditures.Each District agency provided the Task Forcewith an inventory of substance abuse-relatedprogramming and financial figures. Theanalysis revealed that District agencies spent
more than 289 million of local funds ontreatment, prevention, and law enforcementefforts in Fiscal Year 2003.Federalexpenditures add another 61 million tooverall governmental expenditures in theDistrict. Another 7 million are funds from“other” sources, which include monies theDistrict receives from non-tax revenue. Itmust be clearly understood, however, thatthese funds, approximately 356 million,include an extensive array of programmingthat targets substance abuse secondarily toother issues. In other words, only 53million, or 15 percent, of the total 356million expenditure can be tied to programswhose primary focus is substance abuserelated. Furthermore, only 35 million of the 53 million is dedicated solely to the directprovision of substance abuse treatmentprograms.The analysis of the District’s drugprograms and budgets underscores two mainpoints. First, a significant percentage of thebudget is already directed to solving theproblem of substance abuse and itsconsequences. Second, this substantialamount may still be inadequate, especiallywith regard to two critical missions: 1) closingthe gap between the number of addictsrequiring treatment and the services that areavailable and 2) strengthening the District’ssubstance abuse prevention programs.The wisdom of investing in treatment, inparticular, becomes especially clear when onetakes a longer-term perspective. Effectivetreatment, meaning treatment that iscomprehensive and includes aftercare, returnsmore in the long run to its community than itinitially costs. Recent research has found thatevery dollar spent on effective treatment leadsto a 7.46 reduction in crime-related spendingand lost productivity. When savings related tohealth are included, every 1 invested inaddiction treatment programs yields 12 insavings.More and more politicians, policymakers,and members of the public are supportingincreased treatment funding as reasonable“venture capital” whose upfront investmentyields downstream benefits. For example, inApril 2000, the District of Columbia Councilenacted the Choice in Drug Treatment Act of2000 (the Act) which established a vouchersystem allowing patients to choose servicesfrom an approved list of providers. The Actalso contained separate provider certificationrequirements. Ultimately the Act will enhanceaccess to treatment services by expanding thepool of providers that meet certificationrequirements. In addition, the Act establishedthe Addiction Recovery Fund as the solesource of payments to participating certifiedtreatment providers. Finally, a portion of themonies allocated to the fund was earmarkedto implement a pilot substance abusetreatment program for youth. However,because these funds were previously targetingadults, fewer adults will be served through thisfunding source.“Upfront investment in effective prevention and treatmentwill save taxpayer money and the lives of Districtresidents.”-- Addiction, Prevention, and RecoveryAdministration Interim Deputy Director WilliamH. StewardThe certification of treatment providersresults in tangible financial benefit to theDistrict of Columbia. Certification is aprerequisite to gain Medicaid reimbursementfor treatment services provided to Medicaideligible clients. With the approval of theMedicaid Rehabilitation Option for SubstanceAbuse services in 2003, the District will gainaccess to additional substance abuse treatmentdollars.A COMMUNITY APPROACHThe mayor and the Task Force arecommitted to the development andimplementation of a strategic plan that has thebuilt-in support of a wide community ofstakeholders. To foster community buy-in, theTask Force sponsored focus groups thatevolved into Strategy Working Groups in theareas of prevention, treatment, and lawenforcement. In many instances, individuals1-3
within the same field met for the first time. Inaddition, the Task Force sponsored a series ofNeighborhood Forums to gather thecommunity’s perspectives and to incorporatethem into the Strategy. The Strategy WorkingGroups and Neighborhood Forums identifiedthe most pressing issues and provided theTask Force with valuable input on strategicgoals, objectives, and activities. In the comingyear as the Strategy is implemented, theWorking Groups will serve as a major form oflinkage to the entire community of Districtstakeholders.RESULTS-DRIVEN STRATEGYThe mayor’s concept of the SubstanceAbuse Strategy for the District has alwaysbeen one that is fully accountable to the city’staxpayers. In an effort to ensure effectivemonitoring and measurement of Strategyoutcomes and results, the Task Forceconsulted the nation’s leading experts on drugpolicy and budget. The District’s approachincorporates the latest and most sophisticatedmethodology in the field of drug policy,including the “logic model” technique, whichutilizes a systems approach and establishesaccountability by linking programming,budget, and measurable goals and objectives.Unlike the traditional “supply versus demandreduction” approach, the logic modelacknowledges the inter-relatedness of drugprogramming efforts, particularly therelationship between criminal justice andtreatment efforts that function to reduce boththe supply of and demand for drugs. Second,the logic model emphasizes the critical needfor cooperation and coordination amongdifferent levels of government. This isespecially important in the case of the Districtin which the drug-related activities of thefederal and other adjacent governments areinextricably linked.The following Strategy represents acomprehensive, coordinated response to theserious threat posed by substance abuse andits consequences in the District. It provides anoverview of current programming to address1-4the problem and outlines steps to better focusits efforts. It establishes goals and priorities inthe areas of programs and budget and setsforthaframeworkforenforcingaccountability. This strategic approach isespecially critical in the face of challengesposed by scarce resources. Spending prioritiesand targeted points of attack are realisticallydescribed in the context of existing Districtagency policies, plans, and budgets.Strategic planning is an “organic” process,in which a formal feedback mechanism--orperformance measurement system–is used torefine and enhance a strategic approach.(Strategic planning will be addressed in detailin Chapter 4). Nevertheless, the coreunderlying principles of the District’sSubstance Abuse Strategy will remainconstant. We must attempt to prevent drugproblems before they start. We must foster acompassionate response to the suffering ofaddicts and their families. We must ground asubstance abuse strategy in a foundation ofpolitical will, beginning with the city’s mayorand spreading out to the individuals at theneighborhood level. Finally, we must involvea network of stakeholders who are committedto the development, implementation, andmonitoring of the Strategy.It is the vision of both the mayor and theTask Force that this strategic plan becomes amodel effort to inspire other cities with itsmethodology, planning, implementation, andsuccess.
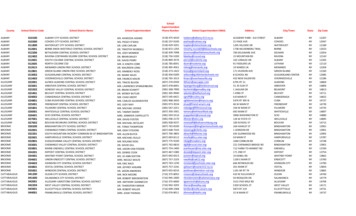
Chapter 2THE DIMENSION OF THE DISTRICT’S SUBSTANCE ABUSE PROBLEMFA C I N G T H E C H A L L E N G ENo single statistic captures the entire scaleand scope of substance abuse in the Districtof Columbia. However, by piecing together avariety of substance abuse data “indicators,” itis possible to gain a sense of the magnitude ofthe problem. In short, these figures portray acity in which the rates of alcohol and drugabuse are high, and in some cases, exceed thenational average. Perhaps most troubling,these elevated rates of addiction arecompounded by a serious shortage oftreatment capacity.The District’s levels of substance abuseresult in significant negative consequences,particularly with regard to the health andsafety of the city’s citizens. Substance abuseimposes considerable economic and socialcosts, including increased burdens on hospital,school, and child welfare systems. Thecumulative effect of these consequencesexacts a toll on all District residents anddevastates certain segments of the populationwhere rates of addiction and drug-relatedviolence are highest.HIV/AIDS, hepatitis B and C, as well as thehealth costs of victims of drug-related crime.Figure 1 illustrates that approximately 700million of the total 1.2 billion in social costsis attributable to alcohol use andapproximately 500 million to other drugs.Reducing the social costs of substanceabuse requires a specific strategic plan,including targeted efforts to lower bothFigure 1 1.2 Billion in Social Costsof Alcohol and Drug Abusein the District of ColumbiaOther Drugs42%Alcohol58% 1.2 BILLION IN SOCIAL COSTSThe social and economic costs of alcoholand drug abuse in the District of Columbiaare staggering—possibly exceeding more than 1.2 billion per year or 2,100 per resident.These costs consist primarily of the value oflost productivity from substance abuse fromsuch causes as premature deaths, criminalcareers, substance abuse-related illnesses, andincarceration. They also reflect the health andcrime consequences from substance abuse,both in the direct effects on the drug user andthe community at large. Such costs includemedical consequences of substance abusefrom diseases such as tuberculosis,current rates of addiction and what may becharacterized as “initiation” or “recruitment”into addiction. This latter category of useinvolves the prevention of first-time use aswell as reductions in so-called “casual druguse” before it progresses into more seriousproblems.Drug addiction and alcoholism contributedisproportionately to social costs. Researchindicates that although the addict populationrepresents only about 20 percent of theoverall user population nationwide, addictsaccount for more than two-thirds of theconsumption of illicit drugs. Similarly, thoseaddicted to alcohol account for the bulk of
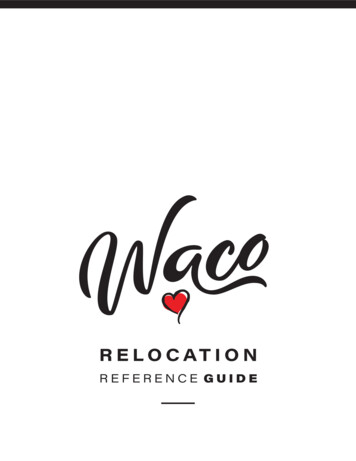
alcohol consumption. As top consumers ofalcohol and other drugs, addicts andalcoholics commit the majority of crime,suffer the majority of health-related problems,and have the lowest productivity.Addiction, however, does not fuel theentire substance abuse problem or itsassociated costs. Recreational drug andalcohol use, sometimes referred to as “casual”or “current drug use,” entices new users tostart using drugs and alcohol. This “casualuser” is usually connected to a family, attendsschool or is employed, and projects a positivelifestyle. In epidemiological terms the “casualdrug user” is a “carrier” of the disease ofaddiction who influences his or her peers tomake unhealthy lifestyle choices. Casual druguse and its role in spreading addiction must bethoroughly examined and understood as amajor contributing force to any givencommunity’s substance abuse problem.their use, which means that it tends toundercount rates of addiction because drugaddicts and alcoholics often lead transitorylifestyles outside of stable household units.(As discussed later in this document, theMayor’s Interagency Task Force on SubstanceAbuse Prevention, Treatment and Control(Task Force) plans to obtain population-basedestimates of the addict population in DC).The Household Survey found that 41,000or nearly 10 percent of District residentsreported using an illicit drug in the 30 daysbefore being interviewed (past-month basis).Table 1Percentage Reporting Substance Useon a Past-Month BasisAgeGroupSCALE OF OVERALL DRUG USEA useful starting point in assessing theextent of the substance abuse problem in theDistrict is to determine the magnitude of thesubstance-abusing population.For thepurposes of making policy, it is helpful toconsider the scale of the substance abuseproblem in the context of general overall userates (prevalence) and the number of“initiates” (individuals who are beginning toexperiment with alcohol, cigarettes, and/orillicit drugs).The 2000 District of ColumbiaHousehold Survey (Household Survey)developed estimates of overall prevalence byasking respondents about their drug-usingactivity in the 30 days before the survey,during the past year, and during theirlifetimes. Such an approach captures allforms of drug-using behavior, from one-timeuse(sometimesreferredtoasexperimentation), recreational use (nondependence), to dependence. The surveyquestions only members of households %12.1%18-2420.5%64.8%31.8%25-3414.0%59.5%25.6%35 6.4%47.5%25.9%Total, AllAge Groups9.6%50.1%25.7%Source: 2000 District of Columbia HouseholdSurvey on Substance Abuse.It also revealed that an estimated 109,000residents had used cigarettes and 73,000individuals had engaged in binge drinking inthe previous month. Table 1 presents data onthe percentage of the population reportingillicit drug, alcohol, and tobacco use on a pastmonth basis (current or regular users). Itshows that the highest rate of illicit drug usein the District occurs between the ages of 18and 34. Among those between the ages of 18and 24, specifically, the overall rate of drug
use is nearly 21 percent—meaning that one infive used illicit drugs on a past-month basis.The number-one illicit “drug of choice”in the District is clearly marijuana.Asignificant number of residents, however, usecocaine. Other drugs, though less prevalentacross all user groups, appear to be popularamong certain segments of the population.For example, although many younger drugusers did not report using either heroin orinhalants, both of these substances were beingused by about 10 percent of drug users overthe age of 35.A resurgence of PCP (phencyclidinehydrochloride) use began in 2001 andcontinues today in the Northeast andSoutheast sectors of the District as well as innearby Prince George’s County. AlthoughPCP still lags behind marijuana and cocaine, arange of statistics marks its troubling increase.Detoxification patients in the District nowtest positive for PCP six times more oftenthan in 1999. The Prince George’s Countypolice laboratory, which tests all drugs seizedin the county, received more than 115 PCPsamples in 2002–up from eight in 2000.The Household Survey reveals dramaticdifferences in illicit drug use on the basis ofgender, employment, and education. Districtmales use illicit drugs at almost two and a halftimes the rate of females (14.0 percent formales compared with 5.8 percent for females).Rates of drug use were highest among thosewith a high school education or less (11.4percent) compared with those with moreeducation (8.6 percent for those with one tofour years of college and 6.4 percent for thosewith graduate degrees). Rates of drug use alsovary according to employment status. Nearlyone of every four (24 percent) unemployedresidents used an illicit substance on a pastmonth basis compared to 8.1 percent forthose employed full time.DISTRICT RATES OF ILLICITDRUG USE 52 PERCENT HIGHERTHAN THOSE OF THE NATIONThe District’s overall rates of substanceabuse are higher than those of the nation as awhole. The overall illicit drug use rate of 9.6percent in the District is a striking 52 percenthigher than the nationwide rate of 6.3 percentfor the same year. District youth, however,ages 12 to 17, report a lower rate of illicit druguse relative to young people throughout theUnited States.DRAMATIC RATES OF ALCOHOLAND TOBACCO USE AMONGDISTRICT YOUTHUnlike the comparatively low rates ofillicit drug use for District youth, theHousehold Survey reveals dramatic rates ofalcohol and tobacco use among this group.Although access to tobacco and alcohol isprohibited for individuals under the ages of 18and 21, respectively, one in every threeDistrict adolescents between 12 and 17 yearsof age (34 percent) reported that they hadused alcohol during their lifetime. Seventeenpercent reported that they used alcohol on apast-month basis.Rates of past-monthalcohol use were highest for young adultsbetween 18 and 24 years old, with 77 percentreporting past-month use. With regard totobacco, about one in 10 adolescents betweenthe ages of 12 and 17 (12.1 percent) reportedsmoking cigarettes on a past-month basis; therate jumps to almost 32 percent for thosebetween the ages of 18 and 24.For first-time drug use—“substanceabuse initiation”—the Household Surveyreveals that the onset of substance abuse is amore serious problem for the District than forthe nation. Simply put: District residentsreport drug use initiation at an earlier agecompared to those in the nation. This onsettends to occur early in the teen years. What is2-3
most interesting, however, is that despite thisearlier initiation, prevalence rates for the Districtamong those
The Mayor's Interagency Task Force on Substance Abuse Prevention, Treatment and Control TASK FORCE MEMBERS James A. Buford Task Force Chair, Director, Department of Health Chief Charles H. Ramsey Task Force Co-Chair, Chief of Police Metropolitan Police Department Neil Albert Director, Department of Parks and Recreation Peggy Cooper Cafritz President, DC School Board