Transcription
The Scope and Likely Clinical Impactof Race-correction in AlgorithmsWho Gets Health Care and Why:AI, Race and Health EquityNIHCM Foundation28 September 2021David S. Jones, M.D., Ph.D.Ackerman Professor of the Culture of MedicineHarvard College ProfessorProfessor of EpidemiologyHarvard University
Should we provide differentmedical care to people ofdifferent races and ethnicities because of their races andethnicities?
Race (and racism) is pervasive in medical practice:Race adjustmentRace correctionRace normingRisk calculatorsTreatment guidelines though much of this is unique to medicine in the United States
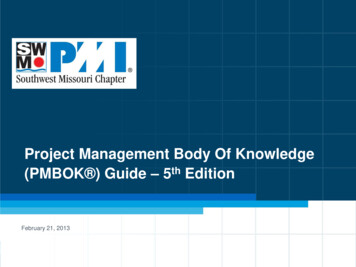
A 13 point scaleHigh score High risk
0 points. Once the number of pointsDevelopment of a Nomogram for Predictionallof ofa patient’sVaginalBirth AftercharacteristicsCesarean Deliveryarethat sum is found on the “total points”redicted probability of VBAC is thehe lowermost scale that is obtained byal line from the “total points” to theale. Thus, a patient whose character0 total points has an approximatelyhaving a VBAC.alidation procedure showed that thethe nomogram on the test set wasiginally determined from the trainingunder the curve that remained 0.75.es the predicted rates of VBAC withWilliam A. Grobman, MD, MBA, Yinglei Lai, PhD, Mark B. Landon, MD, Catherine Y. Spong, MD,Kenneth J. Leveno, MD, Dwight J. Rouse, MD, MSPH, Michael W. Varner, MD, Atef H. Moawad, MD,Steve N. Caritis, MD, Margaret Harper, MD, Ronald J. Wapner, MD, Yoram Sorokin, MD,Menachem Miodovnik, MD, Marshall Carpenter, MD, Mary J. O’Sullivan, MD, Baha M. Sibai, MD,Oded Langer, MD, John M. Thorp, MD, Susan M. Ramin, MD, and Brian M. Mercer, MD,for the National Institute of Child Health and Human Development (NICHD) Maternal–FetalMedicine Units Network (MFMU)*OBJECTIVE: To develop a model based on factors available at the first prenatal visit that predicts chance ofsuccessful vaginal birth after cesarean delivery (VBAC) forindividual patients who undergo a trial of labor.See related editorial on page 796.* For members of the NICHD MFMU, see the Appendix.METHODS: All women with one prior low transversecesarean who underwent a trial of labor at term with avertex singleton gestation were identified from a concurrently collected database of deliveries at 19 academiccenters during a 4-year period. Using factors identifiableat the first prenatal visit, we analyzed different classification techniques in an effort to develop a meaningfulprediction model for VBAC success. After developmentand cross-validation, this model was represented by agraphic nomogram.From the Departments of Obstetrics and Gynecology at Northwestern University,Chicago, Illinois; the George Washington University Biostatistics Center,Washington, DC; the Ohio State University, Columbus, Ohio; NationalInstitute of Child Health and Human Development, Bethesda, Maryland;University of Texas Southwestern Medical Center, Dallas, Texas; University ofAlabama at Birmingham, Birmingham, Alabama; University of Chicago,Chicago, Illinois; University of Utah, Salt Lake City, Utah; University ofPittsburgh, Pittsburgh, Pennsylvania; Wake Forest University, Winston-Salem,North Carolina; Thomas Jefferson University, Philadelphia, Pennsylvania;Wayne State University, Detroit, Michigan; University of Cincinnati, Cincinnati, Ohio; Columbia University, New York, New York; Brown University,Providence, Rhode Island; University of Miami, Miami, Florida; University ofTennessee, Memphis, Tennessee; University of Texas at San Antonio, SanAntonio, Texas; University of North Carolina, Chapel Hill, North Carolina;University of Texas at Houston, Houston, Texas; and Case Western ReserveUniversity, Cleveland, Ohio.RESULTS: Seven-thousand six hundred sixty womenwere available for analysis. The prediction model is basedon a multivariable logistic regression, including the variables of maternal age, body mass index, ethnicity, priorvaginal delivery, the occurrence of a VBAC, and a potentially recurrent indication for the cesarean delivery. Afteranalyzing the model with cross-validation techniques, itwas found to be both accurate and discriminating.Supported by grants from the National Institute of Child Health and HumanDevelopment (HD21410, HD21414, HD27860, HD27861, HD27869,HD27905, HD27915, HD27917, HD34116, HD34122, HD34136,HD34208, HD34210, HD40500, HD40485, HD40544, HD40545,HD40560, HD40512, and HD36801).(Obstet Gynecol 2007;109:806–12)The authors thank the following core committee members: Francee Johnson, BSN,and Julia McCampbell, RN (protocol development and coordination betweenclinical research centers); Elizabeth Thom, PhD (protocol/data management andstatistical analysis); and Alan M. Peaceman, MD (protocol development andoversight).Corresponding author: William A. Grobman, MD, MBA, 333 East SuperiorStreet, Suite 410, Chicago, IL 60611: e-mail: w-grobman@northwestern.edu., APRIL 2007 2007 by The American College of Obstetricians and Gynecologists. Publishedby Lippincott Williams & Wilkins.ISSN: 0029-7844/07806VOL. 109, NO. 4, APRIL 2007CONCLUSION: A predictive nomogram, which incorporates six variables easily ascertainable at the first prenatalvisit, has been developed that allows the determinationof a patient-specific chance for successful VBAC for thosewomen who undertake trial of labor.LEVEL OF EVIDENCE: IIare placed into one group of similar risk.A more individualized approach makes use ofthe many factors that have been associated withVBAC. Some examples of these factors includeLogistic Regression Equation for Predictionof Achieving VBAC After a Trial of LaborPredicted probability of successful VBAC!exp(w)/[1"exp(w)], where w!3.766 – 0.039(age)– 0.060 (prepregnancy body mass index)– 0.671 (African-American race)–0.680 (Hispanic race)"0.888 (any prior vaginaldelivery)"1.003 (vaginal delivery after prior cesarean)–0.632 (recurring indication for cesarean)Pregnant women who have had a prior cesareandelivery often are confronted with the decision ofwhether to attempt a trial of labor. One importantcomponent in this decision-making process is thelikelihood that a trial of labor will result in a vaginaldelivery. Correspondingly, investigators have attempted to elucidate the factors that are associatedwith successful vaginal birth after cesarean delivery(VBAC). Some of the factors that have been repeat-OBSTETRICS & GYNECOLOGYGrobman et alVBAC Prediction809
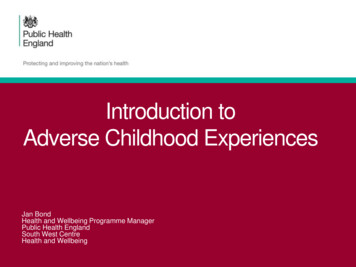
Medicine a nd So cie t y2Table 1. Examples of Race Correction in Clinical Medicine.*Debra Malina, Ph.D., EditorThe New England Journal of MedicineDownloaded from nejm.org by DAVID JONES on June 25, 2020. For personal use only. No other uses without permission.Copyright 2020 Massachusetts Medical Society. All rights reserved.Hidden in Plain Sight — Reconsidering the Useof Race Correction in Clinical AlgorithmsTool and Clinical UtilityThe American Heart Association’s Get with theGuidelines–Heart Failure9 ore)n engl j meddiagnostic algorithms and practice guidelinesthat adjust or “correct” their outputs on the basisof a patient’s race or ethnicity. Physicians use thesealgorithms to individualize risk assessment andguide clinical decisions. By embedding race intothe basic data and decisions of health care, thesealgorithms propagate race-based medicine. Manyof these race-adjusted algorithms guide decisionsin ways that may direct more attention or resources to white patients than to members of racial and ethnic minorities.To illustrate the potential dangers of suchpractices, we have compiled a partial list of raceadjusted algorithms (Table 1). We explore severalof them in detail here. Given their potential toperpetuate or even amplify race-based healthinequities, they merit thorough scrutiny.nejm.orgC ardiolo gyUse of RaceEquity ConcernCardiologyDarshali A. Vyas, M.D., Leo G. Eisenstein, M.D., and David S. Jones, M.D., Ph.D.Physicians still lack consensus on the meaningof race. When the Journal took up the topic in2003 with a debate about the role of race inmedicine, one side argued that racial and ethniccategories reflected underlying population genetics and could be clinically useful.1 Othersheld that any small benefit was outweighed bypotential harms that arose from the long, rottenhistory of racism in medicine.2 Weighing thetwo sides, the accompanying Perspective articleconcluded that though the concept of race was“fraught with sensitivities and fueled by pastabuses and the potential for future abuses,”race-based medicine still had potential: “it seemsunwise to abandon the practice of recording racewhen we have barely begun to understand thearchitecture of the human genome.”3The next year, a randomized trial showed thata combination of hydralazine and isosorbidedinitrate reduced mortality due to heart failureamong patients who identified themselves asblack. The Food and Drug Administration granted a race-specific indication for that product,BiDil, in 2005.4 Even though BiDil’s ultimate commercial failure cast doubt on race-based medicine, it did not lay the approach to rest. Prominentgeneticists have repeatedly called on physicians totake race seriously,5,6 while distinguished socialscientists vehemently contest these calls.7,8Our understanding of race and human genetics has advanced considerably since 2003, yetthese insights have not led to clear guidelines onthe use of race in medicine. The result is ongoingconflict between the latest insights from population genetics and the clinical implementation ofrace. For example, despite mounting evidence thatrace is not a reliable proxy for genetic difference,the belief that it is has become embedded, sometimes insidiously, within medical practice. Onesubtle insertion of race into medicine involvesInput VariablesThe American Heart Association (AHA) Get withthe Guidelines–Heart Failure Risk Score predictsthe risk of death in patients admitted to the hospital.9 It assigns three additional points to any patient identified as “nonblack,” thereby categorizing all black patients as being at lower risk. TheAHA does not provide a rationale for this adjustment. Clinicians are advised to use this risk scoreto guide decisions about referral to cardiologyand allocation of health care resources. Since“black” is equated with lower risk, following theguidelines could direct care away from black patients. A 2019 study found that race may influence decisions in heart-failure management, withmeasurable consequences: black and Latinx patients who presented to a Boston emergency department with heart failure were less likely thanwhite patients to be admitted to the cardiologyservice.24Cardiac surgeons also consider race. The So-Predicts in-hospital mortality in patients withacute heart failure. Clinicians are advised to usethis risk stratification to guide decisions regarding initiating medical therapy.Systolic blood pressureBlood urea nitrogenSodiumAgeHeart rateHistory of COPDRace: black or nonblackAdds 3 points to the risk score if the patient is identified as nonblack. Thisaddition increases the estimated probability of death (higher scores predicthigher mortality).The original study envisioned using this scoreto “increase the use of recommendedmedical therapy in high-risk patients andreduce resource utilization in those at lowrisk.”9 The race correction regards blackpatients as lower risk and may raise thethreshold for using clinical resources forblack patients.Operation typeAge and sexRace: black/African American, Asian,American Indian/Alaskan Native,Native Hawaiian/Pacific Islander,or “Hispanic, Latino or Spanishethnicity”; white race is the defaultsetting.BMIThe risk score for operative mortality andmajor complications increases (insome cases, by 20%) if a patient isidentified as black. Identification asanother nonwhite race or ethnicity doesnot increase the risk score for death,but it does change the risk score formajor complications such as renal failure, stroke, and prolonged ventilation.When used preoperatively to assess a patient’s risk, these calculations could steerminority patients, deemed higher risk,away from these procedures.Serum creatinineAge and sexRace: black vs. white or otherThe MDRD equation reports a higher eGFR Both equations report higher eGFR values(by a factor of 1.210) if the patient is(given the same creatinine measurement)identified as black. This adjustment isfor patients identified as black, suggestingsimilar in magnitude to the correctionbetter kidney function. These higher eGFRfor sex (0.742 if female).values may delay referral to specialist careThe CKD-EPI equation (which included aor listing for kidney transplantation.larger number of black patients in thestudy population), proposes a moremodest race correction (by a factorof 1.159) if the patient is identified asblack. This correction is larger than thecorrection for sex (1.018 if female).AgeHypertension, diabetesSerum creatinine levelCause of death (e.g., cerebrovascularaccident)Donation after cardiac deathHepatitis CHeight and weightHLA matchingCold ischemiaEn bloc transplantationDouble kidney transplantationRace: African AmericanIncreases the predicted risk of kidney graftfailure if the potential donor is identified as African American (coefficient,0.179), a risk adjustment intermediatebetween those for hypertension (0.126)and diabetes (0.130) and that for elevated creatinine (0.209–0.220).Cardiac surgeryThe Society of Thoracic Surgeons Short TermRisk Calculator10 Calculates a patient’s risks of complications anddeath with the most common cardiac surgeries. Considers 60 variables, some of which arelisted here.NephrologyEstimated glomerular filtration rate (eGFR)MDRD and CKD-EPI equations11 culator)Estimates glomerular filtration rate on the basisof a measurement of serum creatinine.Organ Procurement and TransplantationNetwork: Kidney Donor Risk Index s predicted risk of donor kidney graftfailure, which is used to predict viability of potential kidney donor.† Use of this tool may reduce the pool ofAfrican-American kidney donors in theUnited States. Since African-Americanpatients are more likely to receive kidneysfrom African-American donors, by reducing the pool of available kidneys, the KDRIcould exacerbate this racial inequity in access to kidneys for transplantation.
Michelle MorseRWJF Health Policy FellowHouse Ways and Means
This is not a call for race-blind medicine.We need to be race-conscious withoutmaking things worse.
Vol 456 6 November 2008 doi:10.1038/nature07331LETTERSXYGenes mirror geography within EuropeJohn Novembre1,2, Toby Johnson4,5,6, Katarzyna Bryc7, Zoltán Kutalik4,6, Adam R. Boyko7, Adam Auton7,Amit Indap7, Karen S. King8, Sven Bergmann4,6, Matthew R. Nelson8, Matthew Stephens2,3 & Carlos D. Bustamante7
For the common causes of death, illness, ED visits, etc.,how much do genetic variants matter,especially those with a known “racial” distribution?fiThe risks: miscategorization, rei cation, and distraction.
Harm #1: MiscategorizationWhat do the US race/ethnicitycategories really mean?
Sincerely,Debra Malina, Ph.D.Perspective EditorProposal:New England Journal of Medicine10 Shattuck StreetBoston, MA 02115(617) 734-9800Fax: (617) 739-9864http://www.nejm.orgRace is a useful proxy for racism in medical data09-Jul-2020Is it?To the Editor:While many agree that there is very little evidence to support a biologic explanation for race based differences in health outcomes,racism has proven indisputable negative impacts on health. Currently, race is the only available placeholder for racism, which needsto be accounted for. The absence of ‘proof’ for some of the observed differences in outcomes by race is tied to the absence ofscience which has not yet developed any consistent measurement for racism – an important mechanism via which race generatespoor outcomes. When race is included in models that predict higher risk, and that higher risk is then used to design and deliverinterventions, including race ensures that treatment is appropriately matched to outcomes. Underprediction of risk in these instanceshas been associated with harm and has disproportionately impacted socially vulnerable populations, who due to structural racism aredisproportionately black.1-3 Hopefully one day the beta for race will be zero. Until then, there are instances in which including race iscrucial to ensure equitable care delivery.Hammond, Gmerice; Joynt Maddox, Karen E.Washington University in Saint Louis, Washington University in Saint Louis School of Medicine,
Harm #2: Rei cationfiWhat is race?Is race a natural kind?What are the risks of saying that it is?
Harm #3: DistractionDoes our preoccupation with racedistract us from other, moreimportant, factors?
We need to consider race (and racism) — but how?Continue to map the genetic structure of human variations.Develop better categories of human difference (or adequate ancestryinformative markers), though this might be an intractable problem.Be wary of the use of race in predictive tools.We need to do a much better job with SES — but how?Markers that describe multiple aspects of lived experience.Longitudinal datasets that allow the integration of exposures over a lifetime.Sophisticated analyses that can discern cause and effect in complex, multidimensional datasets.
AI algorithms must be designed deliberately to avoidrecapitulating the problems of race and racism
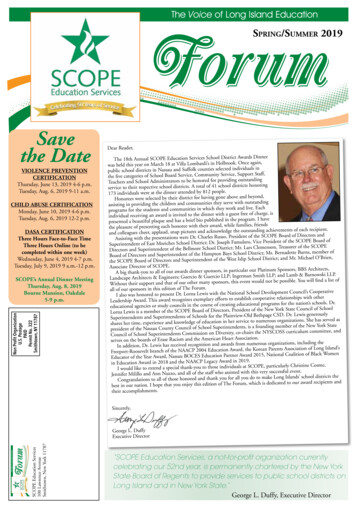
Racial bias in costdata leads an algorithmto underestimatehealth care needs ofBlack patients.RES EARCHDissecting racial bias in an algorithm used to managethe health of populationsZiad Obermeyer1,2*, Brian Powers3, Christine Vogeli4, Sendhil Mullainathan5*†There is growing concern that algorithmsmay reproduce racial and gender disparities via the people building them orthrough the data used to train them (1–3).Empirical work is increasingly lendingresearcher-created algorithms (10–13). Without an algorithm’s training data, objective function, and prediction methodology, we can onlyguess as to the actual mechanisms for theimportant algorithmic disparities that arise.ASCIENCEDownloaded from http://scieHealth systems rely on commercial prediction algorithms to identify and help patients with complexhealth needs. We show that a widely used algorithm, typical of this industry-wide approach andaffecting millions of patients, exhibits significant racial bias: At a given risk score, Black patientsare considerably sicker than White patients, as evidenced by signs of uncontrolled illnesses.Remedying this disparity would increase the percentage of Black patients receiving additionalhelp from 17.7 to 46.5%. The bias arises because the algorithm predicts health care costs rather thanillness, but unequal access to care means that we spend less money caring for Black patients thanfor White patients. Thus, despite health care cost appearing to be an effective proxy for healthby some measures of predictive accuracy, large racial biases arise. We suggest that the choice ofconvenient, seemingly effective proxies for ground truth can be an important source of algorithmicbias in many contexts.Assessing risk, automating racism25 OCTOBER 2019 VOL 366 ISSUE 6464Downloaded from http://science.sciencemag.org/ on October 28, 2019ECONOMICSthat rely on past data to build a predictor offuture health care needs.Our dataset describes one such typical algorithm. It contains both the algorithm’s predictions as well as the data needed to understandSOCIAL SCIENCEits inner workings:that is, the underlying ingredients used to form the algorithm (data,objective function,etc.)and linksa rich racial bias in societyA health carealgorithmreflectstounderlyingset of outcome data. Because we have theBy Ruha Benjaminera, the intentionto deepen racial inequibeyond the algorithm developers by coninputs, outputs,and eventual outcomes,ourties was more explicit, today coded ineqstructing a more fine-grained measure selybecausethosehealth outcomes, by extracting and cleandata allow us a rare opportunity to quantifytries adopt digital tools to identifywho design and adopt such tools are noting data from electronic health records torisk andresources, theau- isolatethinking carefullyracial disparitiesin allocatealgorithmsandthe about systemic racism. determine the severity, not just the number,tomation of racial discrimination isObermeyer et al. gained access to the trainof conditions. Crucially, they found that somechanisms bya growingwhichtheyarise.It shouldbe and contextual data for long as the tool remains effective at preconcern.Socialscientistsing data, algorithm,have been at the forefront of studyone of the largest commercial tools used bydicting costs, the outputs will continue toemphasizedingthatthisalgorithmisnotunique.the historical, political, economic, andhealth insurers to assess the health profilesbe racially biased by design, even as theyethical dimensions of such tools (1–3). Butfor millions of patients. The purpose of themay not explicitly attempt to take race intoRather, it ismostemblematicofageneralizedapanalysts do not have access to widelytool is to identify a subset of patients who reaccount. For this reason, Obermeyer et al.proprietary algorithms and so canquire additional attention for complex healthengage the literature on “problem formulaproach to usedriskpredictionin thesecnottypicallyidentify the precisemecha-healthneeds beforethe situation becomes too diretion,” which illustrates that depending onthat produce disparate outcomes.and costly. Given increased pressure by thehow one defines the problem to be solved—tor, widelynismsadoptedbyarangeofforandOn page 447 of this issue, Obermeyer etAffordable Care Act to minimize spending,whether to lower health care costs or toal. (4) report one of the first studies tomost hospital systems now utilize predictiveincrease access to care—the outcomes the outputs and inputs of an altools to decide how to invest resources. Invary considerably.gorithm that predicts health risk, and inaddition to identifying the precise mechaTo grasp the broader implications of theagencies (21).fluences treatment, of millions of people.nism that produces biased predictions, Oberstudy, consider this hypothetical: The abletoquantifytheracialis 1951 and an African American mother ofOur analysishasimplicationsbeyondwhatsigned to predict the cost of care as a proxydisparity and create alternative algorithmicfive, Henrietta Lacks, goes to Johns Hopkinsfor healthneeds,Black patients algorithm.with thepredictors.Hospital with pain, bleeding, and a knotwe learn aboutthisparticularFirst,same risk score as White patients tend toPractically speaking, their finding meansin her stomach. After Lacks is tested andmuch sicker, becauseprovidersspend algorithmthat if two people have the same risk scoretreated with radium tubes, she is “digitallythe specificbeproblemsolvedby thismuch less on their care overall. This studythat indicates they do not need to be enrolledtriaged” (2) using a new state-of-the-art riskhas analogiesinmanyothersectors:Theprecontributes greatly to a more socially conin a “high-risk management program,” theassessment tool that suggests to hospitalscious approach to technology develophealth of the Black patient is likely muchstaff the next course of action. Because thedicted riskment,of somefutureoutcome(inourdemonstrating how a seeminglyworse than that of their White counterpart.tool assesses risk using the predicted costchoice of label (that is, health cost)According to Obermeyer et al., if the predicand because far less has commonlycase, healthbenigncarewidelylife-usedto weretar-recalibrated to actual needs ofbeencare,spentinitiatesa needs)process withispotentiallytive toolon Black patients despite theirthreatening results. Whereas in a previouson the basis of the number and severity ofactual needs, the automated system unget policy interventionsunder the assumptionactive chronic illnesses, then twice as manyderestimates the level of attention LacksBlackpatientswouldbeidentifiedforinterneeds. On the basis of the results, she isDepartment of AfricaneffectAmerican Studies,Princetonthat the treatmentismonotonicinthatUniversity, Princeton, NJ, USA. Email: ruha@princeton.eduvention. Notably, the researchers went welldischarged, her health rapidly deteriorates,risk, and the methodsused to build the algosciencemag.org421rithm are standard. Mechanisms of bias un-Published by AAASPHOTO: FATCAMERA/GETTY IMAGESRESEARCH ARTICLE
Yes, this will be dif cult, but:Science and technology haveaccomplished an enormous amountWe have a resourceful and wellresourced scienti c establishmentIf we want to do this, we canfifiOur patients deserve better
Race (and racism) is pervasive in medical practice: Race adjustment Race correction Race norming Risk calculators Treatment guidelines though much of this is unique to medicine in the United States