Transcription
Medical Examiners’ – Medical ManualPart 3 - Clinical Aviation Medicine3.1Cardiovascular SystemTable of ContentsPart 3 - Clinical Aviation Medicine . 13.1Cardiovascular System . 13.1.1General Considerations. 43.1.212-lead ECG interpretation . 53.1.2.13.1.2.23.1.2.33.1.3Hypertension . 73.1.3.13.1.3.23.1.3.33.1.4Considerations . 15Information to be provided . 15Disposition . 16Aortic valve disease . 173.1.7.13.1.7.23.1.7.33.1.8Considerations . 13Information to be provided . 13Disposition . 14Mitral valve disease . 153.1.6.13.1.6.23.1.6.33.1.7Considerations . 10Information to be provided. . 12Disposition . 12Coronary Heart Disease . 133.1.5.13.1.5.23.1.5.33.1.6Considerations . 7Information to be provided . 9Disposition . 9Cardiovascular Risk Assessment . 103.1.4.13.1.4.23.1.4.33.1.5Considerations . 5Information to be provided . 5Disposition . 5Considerations . 17Information to be provided . 18Disposition . 18Tricuspid and Pulmonary valve disease . 193.1.8.13.1.8.23.1.8.3Considerations . 19Information to be provided . 19Disposition . 19
3.1 Cardiovascular System I Revision I August 20183.1.9Valve replacement or repair . 203.1.9.13.1.9.23.1.9.33.1.10Atrial Fibrillation (AF) and Atrial Flutter . 213.1.10.13.1.10.23.1.10.33.1.11Consideration . 29Information to be provided . 29Disposition . 29QT Prolongation . 303.1.18.13.1.18.23.1.18.33.1.19Consideration . 28Information to be provided . 28Disposition . 28Left anterior and Left posterior Hemi-Block . 293.1.17.13.1.17.23.1.17.33.1.18Consideration . 27Information to be provided . 27Disposition . 27Right Bundle Branch Block(RBBB) . 283.1.16.13.1.16.23.1.16.33.1.17Considerations . 26Information to be provided . 26Disposition . 26Left Bundle Branch Block (LBBB) . 273.1.15.13.1.15.23.1.15.33.1.16Considerations . 25Information to be provided . 25Disposition . 25Atrio-Ventricular block (AV block) . 263.1.14.13.1.14.23.1.14.33.1.15Consideration . 24Information to be provided . 24Disposition . 24Ventricular pre-excitation . 253.1.13.13.1.13.23.1.13.33.1.14Consideration . 23Information to be provided . 23Disposition . 23Sinus node arrest and sinoatrial block. 243.1.12.13.1.12.23.1.12.33.1.13Considerations . 21Information to be provided . 21Disposition . 22Atrial and ventricular premature beats . 233.1.11.13.1.11.23.1.11.33.1.12Considerations . 20Information to be provided . 20Disposition . 20Considerations . 30Information to be provided . 30Disposition . 30Brugada syndrome . 313.1.19.1Considerations . 31Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 2
3.1 Cardiovascular System I Revision I August 20183.1.19.23.1.19.33.1.20Implantable Devices - Pacemaker . 323.1.20.13.1.20.23.1.20.33.1.21Considerations . 42Information to be provided . 42Disposition . 42Use of Warfarin . 433.1.28.13.1.28.23.1.28.33.1.29Considerations . 41Information to be provided . 41Disposition . 41Marfan’s Syndrome . 423.1.27.13.1.27.23.1.27.33.1.28Considerations . 39Information to be provided . 40Disposition . 40Congenital Heart Disease . 413.1.26.13.1.26.23.1.26.33.1.27Considerations . 38Information to be provided . 38Disposition . 38Venous Thrombo-Embolism and Anticoagulation . 393.1.25.13.1.25.23.1.25.33.1.26Consideration . 36Information to be provided . 36Disposition . 36Peripheral Vascular Disease . 383.1.24.13.1.24.23.1.24.33.1.25Considerations . 35Information to be provided . 35Disposition . 35Aortic Aneurysm . 363.1.23.13.1.23.23.1.23.33.1.24Considerations . 34Information to be provided . 34Disposition . 34Pericarditis . 353.1.22.13.1.22.23.1.22.33.1.23Considerations . 32Information to be provided . 32Disposition . 32Cardiomyopathy. 343.1.21.13.1.21.23.1.21.33.1.22Information to be provided . 31Disposition . 31Considerations . 43Information to be provided . 43Disposition . 43Use of novel anticoagulants (NOACs) . 443.1.29.13.1.29.23.1.29.3Considerations . 44Information to be provided . 44Disposition . 44Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 3
3.1 Cardiovascular System I Revision I August 20183.1.1General Considerations ICAO Annex 1:6.3.4, 6.4.4, 6.5.4 Civil Aviation Act:s27B CAR Part 67:67.103 k & l, 67.105 k & l, 67.107 k & l GD:Timing of Routine Examinations & ExaminationProcedures ICAO medical Manual:Chapter 1This chapter gives guidance for the assessment of applicants’ cardiovascular system.The aim of the examination is to ensure that the applicant does not suffer from anycardiovascular condition likely to cause aeromedically significant impairment of thecardiovascular function or an unacceptable risk of incapacitation.The cardiovascular examination may also identify applicants who are more likely to developcardiovascular disease in the future, and allows giving preventative advice. This may reducefuture aeromedical risk and assist those applicants in retaining their medical certificate forlonger, thus keeping experienced pilots and controllers in the work force.These applicants should be given advice or preferably be referred to their GP to seek suchadvice. While not part of the Director’s regulatory function, this approach is consistent withsound risk management, medical ethics and most recent ICAO recommendations.The assessment should consider that an unrestricted medical certificate permits theexercise of all the privileges that are granted under the licence held. These may includeaerobatics, high altitude operations with reduced O2 partial pressure, long period ofimmobility etc. When appropriate, relevant operational restrictions may be imposed.This chapter of the manual lists a number of frequently encountered cardiovascularconditions relevant to flight safety. The list is not exhaustive. The CAA Aviation MedicalTeam should be consulted as necessary.Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 4
3.1 Cardiovascular System I Revision I August 20183.1.23.1.2.112-lead ECG interpretationConsiderationsThe 12-lead electrocardiogram (12-lead ECG) is an integral element of CAA applicantmedical assessment. A 12-lead ECG is required at the time of the initial application for aclass 1, 2, or 3 CAA medical certificate, and periodically thereafter. The periodicityrequirements for routine 12-lead ECGs, and details about their conduct and resultsinterpretation, are described in the relevant General Directions.This medical manual section describes a number of 12-lead ECG variants that may beconsidered as being normal for the purpose of interpreting a machine-generated 12-leadECG report (See Examination Procedures GD 3.3.2).3.1.2.2Information to be providedFor the purpose of CAA medical assessment, the consideration of a 12-lead ECG requiresThe full ECG tracing, which: Is signed and dated by the medical examiner; and If a single-channel recorder is used, is cut, mounted, and labelled; or If a multi-channel recorder is used, is presented in an A4 format.A report: If applicable, the machine-generated report; or If applicable, the report of the Medical Examiner confirming that the tracing is a‘normal variant’, as described below, and therefore normal for the purpose of CAAmedical assessment; or If applicable, the report of the cardiologist or specialist medical physician whointerpreted the results of the 12-lead ECG.3.1.2.3DispositionA machine-generated 12-lead ECG report may be interpreted as being normal, for thepurposes of paragraph 3.3.2 of the Examination Procedures GD, if: The ECG machine reports the tracing as being normal or a normal variant, withoutqualification[i]; or A cardiologist or specialist medical physician has reported the ECG as being normal ora normal variant; orMedical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 5
3.1 Cardiovascular System I Revision I August 2018The ECG machine reports only one of the following: Sinus arrhythmia; Early repolarization; Short QT; First degree AV (atrio-ventricular) block with P-R interval of no more than 0.21seconds (210 ms) that shortens to 0.20 seconds or less with simple exercise in theMedical Examiner’s office; the Medical Examiner should submit both pre exercise andpost exercise ECGs that document the shortening of the P-R interval; Sinus bradycardia below 45 bpm under the age of 50, and below 50 bpm at age 50 ormore; provided the heart rate increases with simple exercise in the MedicalExaminer’s office; the Medical Examiner should submit both pre exercise and postexercise heart rate, preferably by way of an ECG; Sinus tachycardia of less than 110 bpm; RSR pattern in leads V1 and / or V2 with QRS interval less than 0.12 sec; Isolated conduction delays (such as Intra-atrial Conduction Delay, Intra-ventricularconduction delay, Incomplete / partial right bundle branch block) provided this is not anew appearance; Left ventricular hypertrophy by voltage criteria only in a slim applicant, in the absenceof hypertension; Low voltage in limb leads (but consider obesity and hypothyroidism); Left axis deviation, less than or equal of -30 degrees; No more than one premature ventricular beat on a 12-lead ECG; No more than one premature atrial beats on a 12-lead ECG in an asymptomaticapplicant.The ECG should be interpreted as representing a medical condition of aeromedicalsignificance, unless: The machine reports the ECG as normal; or A cardiologist or specialist medical physician reports the ECG as normal or a normalvariant.[i]“Qualification” refers to wording that serves to suggest other than an absolutely normal ECG. Words suchas ‘possibly’ (e.g “possibly normal”), ‘essentially’ (e.g. “Essentially normal”), are examples of such wordsthat are sometimes used in this context.Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 6
3.1 Cardiovascular System I Revision I August sion represents a long term risk factor for cardiovascular, cerebrovascular andperipheral vascular disease. Isolated mild to moderate hypertension seldom represents animmediate risk of incapacitation but has to be considered when conducting thecardiovascular risk assessment in accordance with the General Direction “ExaminationProcedures”.Blood pressure that is difficult to control or requiring multiple antihypertensive agents shouldalert the ME of the possibility of medical causes that require excluding.Treatment of hypertension should be compatible with flying activities. ACE inhibitors, Betablockers, Calcium antagonist and mild Diuretics are generally compatible. A period ofgrounding should be observed when initiating treatment, lasting from a few days to onemonth depending on the agent. Dose increments should be more cautious than for thegeneral population to ensure absence of side effects, including electrolytes imbalance,hypotension and decreased G tolerance.Clonidine and Methyldopa and other centrally acting agents are not acceptable. Loopdiuretics are generally not acceptable. Sympatholytics such as Guanethidine are notacceptable except that low dose Alpha-blockers may be used with caution. Selective Alphablockers such as Tamsulozin are preferred when used for benign prostate hyperplasia.Alpha-blockers should be avoided by pilots doing aerobatics. They generally require alonger, up to one month, ground trial. BP determination lying and standing to observe forpostural drop should be recorded on several occasions prior to authorising a return to flying.Particular care must be taken in assessing applicants working in a hot environment, withpossible resulting dehydration, or exposure to high G loads (i.e. agricultural pilots, aerobaticpilots).Measurement of Blood Pressure:The blood pressure is measured in the sitting position. The arm must be supported andheld at the level of the Atria. If the BP is outside the range 90-140 systolic, lying andstanding BP readings should also be taken.If initial two readings are below 140 systolic and 90 diastolic no further action is required.If levels are 140/90 or higher two further readings at several minutes’ intervals should betaken together with pulse rate.The same applies to people on antihypertensive medication. Standing and lying readingsshould also be taken for those on medication to assess for postural drop (see BloodPressure Examination Report form 24267-114).If three blood pressure readings exceed 140/90, hypertension is likely and further readingsover several days should be taken. This can be done by the applicant’s own GP or theirnursing staff. Persistently elevated blood pressure should not be dismissed as due to “whitecoat”. If hypertension is suspected a fundus examination should be done.Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 7
3.1 Cardiovascular System I Revision I August 2018Pre-existing records from the GP, community readings or ambulatory monitoring can assistin confirming if an individual suffers from unacceptable hypertension. They should beobtained whenever in doubt.If still in doubt a 24 h blood pressure recording should be considered and the applicant bereferred to their treating physician if hypertension is confirmed.The mean Blood Pressure can be estimated with the following formula: [Diast (SystDiast)/3]. The normal mean blood pressure range is 70 – 110 mmHg;A fast pulse rate may mean that the applicant is particularly anxious; a slow pulse mayreveal good cardiovascular conditioning or undeclared use of beta blockers.Medication and Hypertension:Beta-blockers:Hydrophilic drugs are preferred (i.e. Atenolol,Metoprolol). Only a few days’ grounding isnecessary. Observe for any bronchospasm andfatigue.ACE inhibitors:Long acting ACE inhibitors are preferred;1 to 3 weeks period off flying duty are recommended;Observe for postural hypotension and electrolytesimbalance. Do several lying and standing BPmeasurements.Angiotensin Receptor Blocker (ARB):Permitted, see ACE inhibitors, excellent first line.Calcium channel antagonists:Long acting permitted, i.e. Amlodipine.Nifedipine not permitted, unless it is a controlledrelease preparation, taken once daily.A one week period off flying duty is recommended.Thiazide diuretics &Spironolactone:α-BlockersLow dose diuretics only. Avoid in people with ahistory of gout. Watch for hyponatremia,hypokalaemia / hyperkalaemia. Only a few days offflying duty are necessary unless introduced assecond line.Observe for postural hypotension. Do several lyingand standing BP measurements. Avoid in aerobaticpilots.3 to 4 weeks period off duty are recommended.Slow increase in dosage (For prostatism, selectivealpha blockers should be used i.e. Tamsulozin ratherthan Prazocin).Loop diuretics:Generally not permitted – of aeromedicalsignificance.Centrally acting medication:Not permitted.Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 8
3.1 Cardiovascular System I Revision I August 20183.1.3.2Information to be provided A Blood Pressure Examination Report (form 24067-214) ECG in accordance with the General Directions, or as clinically indicated; Fasting glucose or HbA1c and blood lipids in accordance with the GD “Timing ofexamination” and at other times as indicated; Creatinine, e-GFR and electrolytes on the first occasion that hypertension isdiagnosed, then as indicated; Echocardiogram, if clinically indicated, i.e. suspected ventricular hypertrophy; Investigations to exclude secondary hypertension as clinically indicated, or Investigations as clinically indicated in the presence of co-existing cardiac, vascularrenal disease or other significant pathology.3.1.3.3DispositionApplicants with untreated hypertension should be referred back to their GP for review andtreatment as appropriate.Controlled or mild hypertension is generally allowable at all levels of medical certification.An applicant with hypertension may be considered as having a condition that is not ofaeromedical significance if: The systolic blood pressure is 160 mmHg; The diastolic blood pressure is 90 mmHg; The 5-years cardiovascular risk assessment is below 10%; or It the 5-years cardiovascular risk is 10% or above, ischaemia has been excluded inaccordance with any relevant General Direction; The ECG is normal; There is no evidence of ventricular hypertrophy; There is no evidence of end-organ damage or peripheral vascular disease; The medication is acceptable and there are no adverse drug side effects that are ofaeromedical significance; There is no known or suspected unresolved cause of hypertension such as:alcoholism, reno-vascular disease, endocrine disorder, obstructive sleep apnoea, etc.The certificate duration may be reduced and / or surveillance imposed if the ME considersit appropriate.Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 9
3.1 Cardiovascular System I Revision I August 20183.1.43.1.4.1Cardiovascular Risk AssessmentConsiderationsCardiovascular events may lead to medical incapacitation. Thus an estimation of theprobability of an applicant suffering a cardiovascular (CV) event is an essential part of theassessment. Such estimation is based on community prevalence of ischaemia.The General Direction “Timetable for Routine Examinations” prescribes when a formalcardiovascular risk assessment is required to be performed.The General Direction “Examinations Procedures” prescribes how a formal cardiovascularrisk assessment should be performed.The General Direction “Examination Procedures” requires that a 5-year CV risk estimate of10% or above requires exclusion of cardiac ischaemia.The information sheet “Cardiovascular risk” provides explanations for applicants. MEsmay find the information useful.Note: An applicant with a history of peripheral vascular disease, cerebrovascular accidentor cardiovascular disease automatically falls in a high 5-year cardiovascular risk category,i.e. well above 10%.Stress ECG (or ETT):In general a symptom limited, unequivocally negative, stress ECG reaching a good level ofexercise (end of stage 3, i.e. 9 minutes or above of the Bruce protocol, 85% of maximumpredicted, 10 METS) is acceptable evidence of absence of ischaemia.When a stress ECG cannot be accomplished by exercise, a pharmacological stress testmay be acceptable. The reason for undertaking such test must be explained andconsidered.When required, the CAA acknowledged validity of such test is: One year in the case of Class 1 and 3 applicants; Two years in the case of Class 2 applicants.The Part 5 of this manual provides CAA protocols for the various tests and their reporting.The relevant protocol should be printed and given to the applicant to pass on to thepractitioner conducting the test. This is to ensure a high quality stress is performed, that isuseful for aviation public safety purposes.Calcium Scoring:CT Coronary Artery Calcium Scoring (CT Calcium Scoring) is a relatively inexpensive test.Published research confirms the powerful prognostic value of a zero Agatston score.For the purpose of the cardiovascular risk assessment, a Calcium Score of zero will allowto reassess the cardiovascular risk as being lower than suggested by the method prescribedin the GD “Examination procedures”. A Calcium score of zero can be relied upon for severalyears.Medical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 10
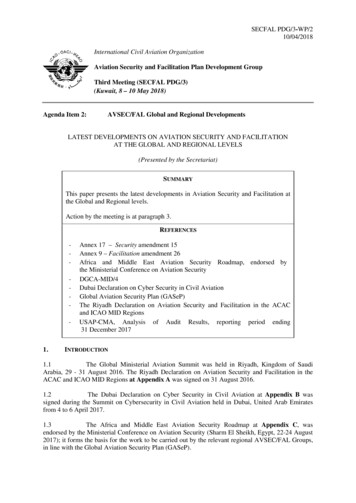
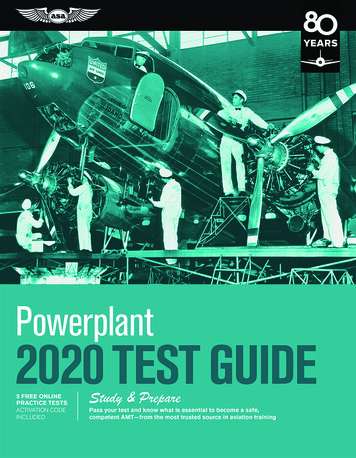
3.1 Cardiovascular System I Revision I August 2018Currently, until changes are made to several documents, this policy can only beimplemented via the statutory process provided by sections 27B(2) and (3) of the CivilAviation Act flexibility (Accredited Medical Conclusion).At this point of time CAA will accept an Agatston score of zero as remaining valid for aperiod of five years.So, currently:1.If an applicant returns an elevated 5-year Cardiovascular Risk Estimation (10% orgreater) then a CT Calcium Score may be undertaken instead of an Exercise Stress ECG;2.If the CT Calcium Score is zero the application may be progressed via thestatutory flexibility process, by applying for the identification of AMC experts;3.If the CT Calcium Score is non-zero then the usual workup, to exclude reversiblemyocardial ischaemia, is required.This process is also shown here in diagram form.Other cardiac tests:In some cases a stress ECG is not sufficient to exclude ischaemia because of an insufficientlevel of exercise, a non-unequivocally negative or a positive tracing.A stress echocardiogram or myocardial perfusion scan can be undertaken to more reliablyexclude ischaemia. Other reasons to undertake such investigations may be the applicant’scardiovascular history or a previous equivocal stress ECG. In doubt MEs should contact theCAA.The role of other investigative modalities has not been clearly established in the context ofaeromedical certification. MEs should consult with CAA whenever an applicant presents toMedical Examiners’ – Medical Manual Part 3 - Clinical Aviation Medicine 11
3.1 Cardiovascular System I Revision I August 2018them having undergone any other such investigations, including coronary angiography orCT coronary angiography.3.1.4.2Information to be provided.See comments about CT Calcium Scoring that may affect the following list. ECG, blood lipids and blood glucose or HbA1c, in accordance with the GD “Timing forRoutine Examinations”; Cardiovascular risk assessment in accordance with the GDs “Timing of RoutineAssessments” and “Examination Procedures”; In the case of a Class 1or 3 applicant: Annual stress ECG (or test of higher sensitivity/ specificity as appropriate) when ischaemia needs excluding under the GD“Examination Procedure” - Full ECG tracings and report to be provided to CAA; In the case of a Class 2 applicant: Two yearly stress ECG (or test of higher sensitivity /specificity as appropriate) when ischaemia needs excluding under the GD“Examination Procedure” - Full tracing and report to be provided to CAA; Tests and reports as may have been advised by CAA in the case of an applicant witha history of cardiovascular disease. Such applicants often require annual specialistreview and exercise testing of some kind.3.1.4.3Disposition An appl
Medical Examiners' - Medical Manual Part 3 - Clinical Aviation Medicine 5 3.1.2 12-lead ECG interpretation 3.1.2.1 Considerations The 12-lead electrocardiogram (12-lead ECG) is an integral element of CAA applicant medical assessment. A 12-lead ECG is required at the time of the initial application for a