Transcription
TJRFORCE-TJR2015 Annual 6723(85599FORCE)E:force- ‐tjr@umassmed.eduW:www.force- ‐tjr.org
TJRFORCE-TJR2015 Annual Report 2FORCE-TJR2015 Annual Report
TJRFORCE-TJR2015 Annual Report 3Executive SummaryThe2015FORCE- .1.CelebratinginitialFORCE- ‐TJRaccomplishmentsFORCE- ‐TJRexceededtheoriginalgoalsoftheAHRQaward(2010- ch,cliniciansandhospitalsusetheFORCE- Specifically: FORCE- isk- ReplacementprogramwasinformedbytheFORCE- s,FORCE- ‐TJRbenchmarksarecriticalforCJRhospitals. HospitalsandsurgeonsusetheFORCE- ratanyhospitalandpatient- ‐reportedpainreliefandfunctionalgain. FORCE- paymentsfromCMSqualityprograms. FORCE- icsurgeons. FORCE- orship,asFORCE- fsurgeryandrecovery.ThecoreFORCE- ‐TJRattributesofexpertdatacollection,real- ‐timereports,andrisk- willassureefficientpost- CE- ly,PatriciaD.Franklin,MDMBAMPHDavidC.Ayers,MD
TJRFORCE-TJR2015 Annual Report 4CONTENTSExecutive Summary3FORCE-TJR Accomplishments (2010-2015)6Policy informed by FORCE-TJR analyses6PRO Implementation expertise for TJR and beyond6FORCE-TJR Registry accomplishments6FORCE-TJR Comparative Effectiveness Research8The future: FORCE VALUE Management SystemHighlights from new FORCE-TJR research911PRO Implementation framework to guide successful capture12Post-TJR readmissions are associated with poorer functional gain after TJR13After successful TKR, patients achieve pain relief in their non-operative hips and knee14Post-TKR benefits demonstrated across diverse pre-operative profiles15Today’s TJR patients are younger, heavier, and just as disabled16Patients with high BMI report significant functional improvement after TJR17Appendices19Appendix 1. FORCE-TJR Bibliography19Appendix 2. How FORCE-TJR Differs from other Registries27Appendix 3. FORCE-TJR Data Elements, Cohort Summary28Appendix 4. FORCE-TJR Methods/Data Quality29Appendix 5: FORCE-TJR Publications and Ancillary Studies Committee Procedures31
TJRFORCE-TJR2015 Annual Report 5TheFORCE- mitteeNationalStakeholderCommitteeJeroanAllison,M )PatriciaFranklin,M ahFreund,M PHM APhDClaremontGraduateUniversity(PORT- ‐TKR)TerenceGoie,M r,M son,M oolCourtlandLewis,M DHartfordHospital(AAHKS)DanicaMarinac- ‐Dabic,M kinDiseases(NIAMS)MarkMelkerson,M cadiaUniversityJymeH.Schafer,M ciaSkolnik,M SWCitizensforPatientSafetyPaulVoorhorst, t,Inc.
TJRFORCE-TJR2015 Annual Report 6FORCE-TJR Accomplishments (2010-2015)The AHRQ award explicity stated that FORCE-TJR should serve both as a TJR quality and outcomes registryand as a comparative effectiveness research program. FORCE-TJR went beyond these goals to inform CMS paymentpolicy and to build generalizable PRO implementation strategies.Policy informed by FORCE-TJR analyses CMS/CMMI Value-based payment in TJR. FORCE-TJR analyses informed the risk-adjustment and outcome measuresfor the 2016 CMS/CMMI implementation of the mandatory TJR value-based payment system in 67 US metropolitanareas (Comprehensive Care for Joint Replacement program). Comprehensive risk-adjustment for readmissions,complications, and patient-reported outcomes is essential to assure equitable comparisons across hospitals and tosupport uniform patient access to TJR. In addition, the FORCE-TJR cohort was used to validate brief patient-reportedmeasures (HOOS/KOOS JR). Thus, the FORCE-TJR produces risk-adjusted, national norms for the two CJR patientreported outcome measures: HOOS/KOOS JR and the full HOOS/KOOS. US/CMS and UK comparison of patient-reported outcomes in TJR. FORCE-TJR data were highlighted in a CMSsponsored comparison of patient-reported outcomes between the US and United Kingdom for obese and non-obesepatients. The analyses were presented at the Healthcare Datapalooza in June 2015. FDA and MDEpiNet. FORCE-TJR, in collaboration with Weill Cornell and other regional US registries, will form anorthopedic network to monitor TJR implant outcomes. Uniquely, FORCE-TJR will assess the role of patient-reportedpain and function through a new phone APP to monitor early implant failure. International Consortium of Health Outcome Measures (ICHOM). The FORCE-TJR PI (Franklin) lead an internationalosteoarthritis and TJR workgroup of experts to endorse an outcome measure set and collection methods. Of note, theICHOM Osteoathritis/TJR measure set parallels the core FORCE-TJR measures.PRO Implementation expertise for TJR and beyondThe collection of complete longitudinal outcome data is critical in this era of value and quality measurement.FORCE-TJR’s unique direct-to-patient outcome methods, refined web-based infrastructure, and novel risk-adjustedoutcome reporting system achieved 85% complete data over the first year. No other US registry reports this level ofcompleteness. While the International Society of Arthroplasty Registries expects over 70% long-term data for sufficientdata quality, other US registries are reporting 20-40% response. Specific FORCE-TJR products to improve PRO collectionmethods include: PRO implementation framework for all conditions. With funding from AHRQ, and in collaboration with AcademyHealth’s Electronic Data Methods team and other US registries, FORCE-TJR investigators developed a framework toguide implementation of PROs. Based on interviews with more than 30 PRO leaders in medical, surgical, pediatric, andbehavioral health fields, this framework guides planning and implementation for clinicians and hospitals. APP for PRO collection. With AHRQ and FDA funding, the FORCE-TJR team is converting direct-to-patient PROcapture through a simple phone APP. Patient and clinician focus-groups informed the usability and design. Early APPtesting in underway with test deployment this year. PROs in pharmaceutical outcomes. FORCE-TJR will support the PRO analyses in the team implementing the newlyfunded PCORI pragmatic trial to assess comparative effectiveness of three different anti-thrombotic prophylacticmedications in TJR patients.FORCE-TJR Registry accomplishmentsSince October 2010, the Function and Outcomes Research for Comparative Effectiveness in Total JointReplacement (FORCE-TJR) registry has been a US leader in TJR outcome measurement. By fall 2015, the original AHRQ-
TJRFORCE-TJR2015 Annual Report tedtoassurethattheFORCE- dsurgeonsintheUStoday.Thus,FORCE- ‐TJRhastheonlyrisk- ‐adjusted,USnationalbenchmarksforperi- ‐operativeadverseevents,patient- age.TheFORCE- s,FORCE- tcomesforyearstocome.FORCE- tocollect,score,andtrendpatient- ‐reportedoutcomes(PROs)overtime,FORCE- ‐TJRoffersreal- ‐timescoringandpainandfunctiontrends.Real- ‐timepatient- ement)beforeandafterTJR. paredtonationalTJRnormstoguidetimingforsurgery. areddecision- essenthusiasticsupportforweb- itwas - - tforcollectingFORCEoutcomemeasures. TherevisedFORCE- eonscouldnotanswer:(1)Howdomypatients’pre- fortsoeffectively.”Surgeon,OK.3. ForInsurerValueMonitoring: CMSinitiatedpublicreportingofpost- rationwithAAHKS,FORCE- ‐TJRsignificantlyimprovedtherisk- risk- vementbeforethesedataarepubliclyreported. Privateinsurersanticipateusingpre- fTJR.FORCE- ‐TJRisdeployingnewdecision- toring: TheFORCE- ‐TJRdataprovideearlypost- sthatsolelydefine
TJRFORCE-TJR2015 Annual Report 8implantfailureasrevisionsurgery,FORCE- ‐TJRsurveillanceincludespost- ‐TJRimplantcomplicationsandpatient- ct- ‐to- ers. Implantevaluation.ThecomprehensiveFORCE- ORCE-TJR Comparative Effectiveness FORCE- ‐TJRcomparativeeffectivenessresearch. eployingbriefsurveys,FORCE- heFORCE- ersions. Definingpatientsatriskforreadmission.Thesub- erfunctionalgain.Identifyingthishigh- financialriskinaneraofbundledpayments.FORCE- todefinehigh- AOS- ‐CMSsummitonpatient- tprogram. Definingsub- lantdataandpatient- ‐reportedoutcomes,FORCE- llextendtheimplementationofnewmethods. estsalesscomplexpatientpool,butFORCE- ortthesame,orgreater,joint- ‐specificandglobalpainanddecreasedfunctionpre- E- ‐TJRhasnationalnormsforpre- ‐operativeandpost- swhoarethefastestgrowingusersofTJR. publicreportssuggestingthatone- RCE- ‐TJR’spatient- onsandappropriatenessinthissub- ‐group. Definingimpactofco- ndnon- ‐operativehipsandknees,negativelyaffectsself- urepubliccomparisonsofPROsafterTJRmustadjustforco- ‐existingmusculoskeletalconditions.
TJRFORCE-TJR2015 Annual Report 9Future FORCE-TJR researchIn the next years, using 2-5 year outcomes on 25,000 FORCE-TJR patients, we will evaluate the interactionsamong patient-comorbidity-implant factors in key patient sub-groups to define tailored best practices associated withpersistent post-operative pain relief, functional gain, and minimal post-TJR adverse events. FORCE-TJR cohort patientsagree to annual assessments for the next 20 years.FORCE-TJR BibliographyThe current FORCE-TJR Bibliography is included in Appendix 1. Since the initial overview paper published inJAMA, 30 manuscripts have been published (with additional papers under review) in diverse journals serving primarilyorthopedic surgeons and research methodologists. In addition, five ancillary research grants were awarded from AHRQ,PCORI, FDA, and NIH and six more applications are under review. Finally, more than 100 international and national peerreviewed abstracts have been presented at diverse professional meetings serving orthopedics, rheumatology, publichealth, health services research, psychometrics, and informatics.FORCE-TJR Membership Model will expand patient dataTo assure sustainability of the FORCE-TJR infrastructure, paid FORCE-TJR memberships are now open to US andinternational hospitals and surgeons committed to high-value care. In the first months after offering membership, thenumber of surgeons participating in FORCE-TJR grew by 40%, and membership continues to climb. The first internationalparticipant just joined. Member hospitals and surgeons receive the same risk-adjusted benchmarks as the initial FORCETJR sites while contributing larger numbers of TJR procedures from even more diverse settings. The FORCE-TJR cohortcontinues to grow!The future: FORCE VALUE Management SystemThe introduction of bundled payment programs brings new responsibilities and risks for hospitals and affiliatedorthopedic surgeons. Hospitals and surgeons are collaborating to manage the total care and resource use across the 90days of the surgical episode. Pre-operative risk-profiles are the first step in selecting and preparing patients for TJRsurgery, tailoring in-hospital and post-discharge care, and guiding rehabilitation. The original FORCE-TJR model has beenadapted in three important ways to meet these new demands, for hip and knee replacement, shoulder, and spine care.
TJRFORCE-TJR2015 Annual Report - ‐TIMEPRE- ndimproveoutcomes.a.Informshareddecisions:Patient- .Tailorperi- ‐operativeandpost- ilesinformsurgicalpreparationandperi- in- ‐homepost- GEMENT:Inhospitalandpost- pisodewithnewweb- ors,in- twoways:a.Risk- calteamtoassurecompletepre- ‐operativeandpost- enewreal- ‐timeepisodemonitoringtools.
TJRFORCE-TJR2015 Annual Report 11Highlights from new FORCE-TJR sofrecentlyreportedfindingsfromFORCE- ‐TJRresearch,including:§ reinorthopedicsandotherconditions§ Post- ctionafterTJR§ rnon- ‐operativehipsandknee§ Post- ‐TKRbenefitsdemonstratedacrossdiversepre- ‐operativeprofiles§ sabled§ theFORCE- ‐TJRteam.
TJRFORCE-TJR2015 Annual Report 12PRO Implementation framework to guide successful d.Todefinethisframework,registryleadersfromFORCE- thods.)
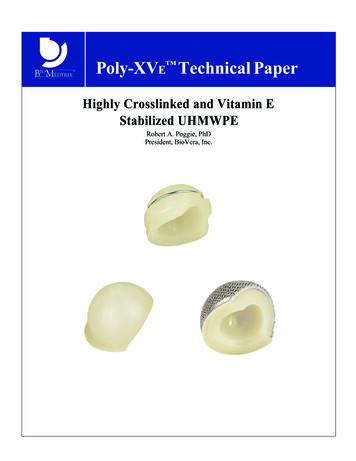
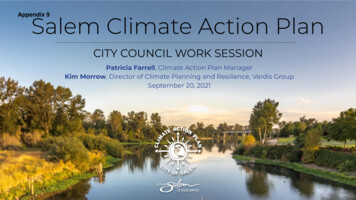
TJRFORCE-TJR2015 Annual Report 13Post-TJR readmissions are associated with poorer functional gain after acement(TJR)byhospitalandisplanningtoaddpatient- ororthopedic- ‐relatedissues.FORCE- reOAinnon- avepoorerpre- ‐TJRfunction(allp 0.05).TheFORCE- ‐TJRreadmissionmodelpredicted80- (PCS 30 14%)ascomparedtopatientswithnoreadmission(8%;p edatasupporttheimportanceofjoint- 0.000.250.500.751.001 - SpecificityArea under ROC curve RegistryDatafromFORCE- ‐TJRtoImprovetheAccuracyofRisk- ‐AdjustmentPredictionModelsforThirty- 8- ‐671.0.000.25Sensitivity0.750.000.25Area under ROC curve 0.85960.501 - Specificity0.751.00
TJRFORCE-TJR2015 Annual Report 14After successful TKR, patients achieve pain relief in their non-operative hipsand kneeToassesstheeffectofsuccessfulTKRonshort- ‐termpainreliefofthenon- uatedthechangeinpainineachjointafterTKR. efintheirnon- hesepatientsareabletounloadtheremainingnon- thepatientswhowerepainfreeintheirnon- ofPatientswithImprovementChi- ‐squarep- ‐valuePainScoreMild49%Moderate77%55.98p provementChi- ‐squarep- ‐valueScoreMild59%Moderate81%54.39p ImprovementChi- ‐squarep- ‐valuePainScoreMild35%Moderate63%239.81p 0.0001Severe79%
TJRFORCE-TJR2015 Annual Report 15Post-TKR benefits demonstrated across diverse pre-operative profilesWeexamined6- )bypre- orfunctionpre- function6- 6- ittlePain/HighFunctionn 234(5%)ClinicalCharacteristicsbyPre- ‐TKRPainandFunctionPain&FunctionStatus6- ‐mthPost- ovement toLittlePain- ‐HighFunctionWorstDecline toHighPain- REFREF6- ‐monthChangeinPainPain,KOOSMean(SD)- ‐PrePain,KOOSMean(SD)- erencesUnadjustedStandardizedDifferences,ES*6- ‐monthChangeinFunctionFunction,SF36PCS,Mean(SD)- ‐PreFunction,SF36PCS,Mean(SD)- erencesUnadjustedStandardizedDifferences,ES*6- ‐mthPost- ‐TKRSelf- ago- ry87%46%47%19%HighPain/PoorFunctionn roup3HighPain/HighFunctionn alityofLife(QOL)IssuesPre- ‐andPost- ‐TKRAwarenessKneeProblemDaily/Constantly- ‐PreAwarenessKneeProblemDaily/Constantly- ‐PostPainFrequencyDaily/Always- ‐PrePainFrequencyDaily/Always- ‐PostGroup2LittlePain/PoorFunctionn %94%28%63%82%78%65%100%65%98%35%
TJRFORCE-TJR2015 Annual Report 16Today’s TJR patients are younger, heavier, and just as disabledAtthetimeofTKRandTHR,younger( scomparedtoolder( ndolderadults.THR PATIENTSTKR PATIENTSCharacteristicsAge 65Age 65pvalueAge 65Age .151.9neverBaselinesf- - .110.0000.0007.812.011.913.52- ‐58.417.98.517.7 6Paininnon- 00(%)**BasedontheHOOS/KOOS
TJRFORCE-TJR2015 Annual Report 17Patients with high BMI report significant functional improvement after tfunctionalgainsalthoughpatientswithBMI 35hadlowermeanfunctionalgainthanthosewithBMI safterTKR,severelyobesepatients(BMI oorgreaterthanpatientswithBMI .09%29.940.411.0
TJRFORCE-TJR2015 Annual Report 18SELECTING A TOTAL JOINTREPLACEMENT REGISTRYChoosing the best TJR registry to meet your needscan be challenging. All registries are not alike; eachhas different data collection resources, reporting, andanalytic capabilities.FORCE-TJR QI brings comprehensive TJR registry outcomes (patient-reported measures,readmission and complications, and implant failures)FORCE-TJR QI is a national leader in risk-adjusted outcome analyses and benchmarks.Below is a checklist to help you (1) define your registry needs, (2) illustrate how specific functions can assist you, and (3) guide your questions whenselecting a registry to meet your needs.Hospital/Surgeon needsRequired strategies/solutionsFORCE-TJR QI1. Manage TJR utilization and outcomes tomeet CJR and bundled payment goals.Registry system follows the patient across time and locations, and is notlinked to the hospital.Example: FORCE-TJR QI system is web-based and starts in the surgeonoffice captures data in the hospital, and for 12 months after TJR. a. Capture complete risk factors BEFOREsurgery to guide patient pre-operativepreparation and minimize risks.Registry system returns data immediately in scored, trended format withnational norms to support decisions.Example: FORCE-TJR QI Patient Risk Summary is generated real-time priorto surgery. It includes medical, emotional, and musculoskeletal risk factors,trended pain and function before surgery, and social needs. b. Capture pre-operative preparation steps,in-hospital events, and post-dischargemonitoring to flag at-risk patients.Registry system supports patient and cl
FORCE-TJR 2015 Annual Report ! ! University!of!Massachusetts!Medical!School!! ion! T:!855993!6723!(855!99FORCE)!!!E .