Transcription
An Overdose DeathIs Not Murder:Why Drug-InducedHomicide Laws AreCounterproductiveand Inhumane
We are the Drug Policy Allianceand we envision new drug policiesgrounded in science, compassion,health and human rights.Please join us.Copyright November 2017Drug Policy AllianceAll rights reservedPrinted in theUnited States of AmericaThis report is alsoavailable in PDF formaton the Drug PolicyAlliance website:drugpolicy.org/DIH
Table of Contents2Executive Summary556Background: Overdose Crisis and ResponseIncreasing Rates of Opioid OverdoseResponse to Opioid Overdose Crisis8899Drug-Induced Homicide: A Legal OverviewFederal and State LawsLegislative HistoryLegal Challenges1111151618Drug-Induced Homicide: A Current SnapshotIncreasing ProsecutionsNew LegislationFentanylProfile: Michael Millette2021232628Regional Trends: nal Trends: The NortheastPennsylvaniaNew YorkNew Jersey33343536Regional Trends: The SouthTennesseeLouisianaNorth Carolina37A Parent’s Perspective: Peter Brunn in His Own Words3939Prosecutions of Drug-Induced Homicide Will Not Curb Overdose DeathsDrug-Induced Homicide Prosecutions Will Neither Deter Drug Selling nor ReduceOverdose Death RatesDrug-Induced Homicide Laws Undermine 911 Good Samaritan Laws4041414347485152Drug-Induced Homicide Laws Perpetuate the Harms of CriminalizationDrug-Induced Homicide Laws Foster Poor Prosecutorial DiscretionProfile: Amy ShembergerEnforcement of Drug-Induced Homicide Laws Has the Potential toExacerbate Racial Disparities in the Criminal Justice SystemProfile: James LinderDrug-Induced Homicide Laws Reduce Access to Needed Services525253545454Drug-Induced Homicide Prosecutions Waste Resources that Could be Spenton Effective Interventions Proven to Reduce Overdose DeathsOverdose Prevention Education, Good Samaritan, and Naloxone AccessSafe Consumption SitesDrug CheckingOpioid Agonist TherapyHeroin-Assisted TreatmentPromising Research55Conclusion56Appendix66Endnotes
Executive SummaryThe country is in the middle of a tragic increasein drug overdose deaths. Countless lives havebeen lost – each one leaving an irreparable rift inthe hearts and lives of their families and friends.These tragedies are best honored by implementingevidence-based solutions that help individuals,families, and communities heal and that preventadditional avoidable deaths. This report examinesone strategy that the evidence suggests isintensifying, rather than helping, the problem andcalls for leaders to turn towards proven measures toaddress the increasing rates of overdose deaths.In the 1980s, at the height of the draconian war on drugs,the federal government and a host of states passed “druginduced homicide” laws intended to punish people who solddrugs that led to accidental overdose deaths with sentencesequivalent to those for manslaughter and murder. For thefirst 15-20 years, these laws were rarely used by police orprosecutors, but steadily increasing rates of drug overdosedeaths across the country have led the law enforcementcommunity to revive them. Currently, 20 states – Delaware,Colorado, Florida, Illinois, Kansas, Louisiana, Michigan,Minnesota, New Hampshire, New Jersey, North Carolina,Oklahoma, Pennsylvania, Rhode Island, Tennessee,Vermont, Washington, West Virginia, Wisconsin, andWyoming – have drug-induced homicide laws on the books.A number of other states, while without specific druginduced homicide statutes, still charge the offense of drugdelivery resulting in death under various felony-murder,depraved heart, or involuntary or voluntary manslaughterlaws. These laws and prosecutions have proliferated despitethe absence of any evidence of their effectiveness in reducingdrug use or sales or preventing overdose deaths. In fact,as this report illustrates, these efforts exacerbate the veryproblem they seek to remediate by discouraging people whouse drugs from seeking help and assistance.Although data are unavailable on the number of peoplebeing prosecuted under these laws, media mentions of druginduced homicide prosecutions have increased substantiallyover the last six years. In 2011, there were 363 news articlesabout individuals being charged with or prosecuted for druginduced homicide, increasing over 300% to 1,178 in 2016.2Based on press mentions, use of drug-induced homicide lawsvaries widely from state to state. Since 2011, midwesternstates Wisconsin, Ohio, Illinois, and Minnesota have beenthe most aggressive in prosecuting drug-induced homicides,with northeastern states Pennsylvania, New Jersey, and NewYork and southern states Louisiana, North Carolina, andTennessee rapidly expanding their use of these laws. Furthersignaling a return to failed drug war tactics, in 2017 alone,elected officials in at least 13 states – Connecticut, Idaho,Illinois, Maine, Maryland, Massachusetts, New Hampshire,New York, Ohio, South Carolina, Tennessee, Virginia, andWest Virginia – introduced bills to create new drug-inducedhomicide offenses or strengthen existing drug-inducedhomicide laws.Prosecutors and legislators who champion renewed druginduced homicide enforcement couch the use of this punitivemeasure, either naively or disingenuously, as necessary tocurb increasing rates of drug overdose deaths. But thereis not a shred of evidence that these laws are effective atreducing overdose fatalities. In fact, death tolls continue toclimb across the country, even in the states and countiesmost aggressively prosecuting drug-induced homicide cases.As just one example, despite ten full-time police officersinvestigating 53 potential drug-induced homicide casesin Hamilton County, Ohio in 2015, the county stillrecorded 100 more opioid-related overdose deaths in2016 than in 2015.This should be unsurprising. Though the stated rationaleof prosecutors and legislators throughout the country isthat harsh penalties like those associated with drug-inducedhomicide laws will deter drug selling, and, as a result, willreduce drug use and related harms like overdose, we haveheard this story before. Drug war proponents have beenrepeating the deterrence mantra for over 40 years, and yetdrugs are cheaper, stronger, and more widely available than atany other time in US history. Supply follows demand, so thesupply chain for illegal substances is not eliminated becausea single seller is incarcerated, whether for drug-inducedhomicide or otherwise. Rather, the only effect of imprisoninga drug seller is to open the market for another one. Researchconsistently shows that neither increased arrests nor increasedseverity of criminal punishment for drug law violationsresults in less use (demand) or sales (supply). In other words,punitive sentences for drug offenses have no deterrent effect.An Overdose Death Is Not Murder: Why Drug-InducedHomicide Laws Are Counterproductive and Inhumane
Unfortunately, the only behavior that is deterred by druginduced homicide prosecutions is the seeking of life-savingmedical assistance. Increasing, and wholly preventable,overdose fatalities are an expected by-product of druginduced homicide law enforcement. The most commonreason people cite for not calling 911 in the event of anoverdose is fear of police involvement. Recognizing thisbarrier, 40 states and the District of Columbia have passed“911 Good Samaritan” laws, which provide, in varyingdegrees, limited criminal immunity for drug-related offensesfor those who seek medical assistance for an overdose victim.This public health approach to problematic drug use,however, is rendered useless by enforcement of drug-inducedhomicide laws.People positioned to save lives are unlikely to call 911 if theyfear being charged with murder or manslaughter. JenniferMarie Johnson called 911 when her husband overdosed aftershe gave him methadone; she is currently serving six yearsin Minnesota prison for drug-induced homicide. Erik ScottBrown received an enhanced sentence of 23 years in federalprison partly because he failed to call 911 after a friend,whom he had supplied with one tenth of a gram of heroin,fatally overdosed. According to his testimony, the reasonhe did not call 911 was because drugs were present at thescene. Prosecutors – by their own admissions – want to make“examples” of these types of cases. But elevating punishmentsfor drug-induced homicide charges has a chilling effect onseeking medical assistance and, as a result, leads to more, notfewer, avoidable overdose fatalities.This is especially true when police and prosecutors widelyabuse their discretion in investigating and prosecutingdrug-induced homicide cases. The vast majority of chargesare sought against those in the best positions to seekmedical assistance for overdose victims – family, friends,acquaintances, and people who sell small amounts of drugs,often to support their own drug addiction. Despite policeand prosecutor promises to go after upper echelon drugmanufacturers and distributors, that rarely happens. Outof the 32 drug-induced homicide prosecutions identified bythe New Jersey Law Journal in the early 2000s, 25 involvedprosecution of friends of the decedent who did not selldrugs in any significant manner. After analyzing the 100most recent cases of drug-induced homicide in southeasternWisconsin (as of February 2017), Wisconsin’s Fox6 reportedthat nearly 90% of those charged were friends or relativesof the person who died, or the lowest people in the drugwww.drugpolicy.orgsupply chain, who were often selling to support their ownsubstance use disorder. A Chicago Tribune review of druginduced homicide cases between 2011 and 2014 in variousIllinois counties showed that the defendant was typically thelast person who was with the person who overdosed. Lawenforcement must be held accountable for this appallingmisuse of discretion; particularly when it discourages theseeking of medical care and wastes resources that couldotherwise be spent on interventions that have actuallybeen proven successful at reducing overdose deaths.Unchecked police and prosecutorial discretion in druginduced homicide cases is particularly ominous given theseverity of sentences and the racist history of drug warenforcement. Although rates of drug use and selling arecomparable across racial lines, black and Latino people arefar more likely to be stopped, searched, arrested, prosecuted,convicted and incarcerated for drug law violations thanare white people. When, in response to the overdose crisis,Maine Governor Paul Le Page states that “black dealers”and “guys with the name D-Money, Smoothie, Shifty” arethe root of the problem by bringing drugs from places likeBrooklyn into his rural state, he lays it bare. Most electedofficials and prosecutors advocating a punishment-orientedapproach to a public health crisis are more careful with theirlanguage than Le Page – targeting “pushers” and “thosepeople” – but the implication is the same.Enforcement of drug war policies has historically targetedblack and Latino communities, and drug-inducedhomicide prosecutions appear to follow this pattern. Whilecomprehensive data are not available, the district attorneyof one predominantly white suburban county in Illinois witha black population of only 1.6% has charged four black menfrom Chicago with drug-induced homicide (making up35% of the total prosecutions), and one prosecutor inMinnesota appears to have charged predominutely blackpeople with drug-induced homicide. Though we cannotdraw any conclusions from these sparse facts, if lawenforcement utilizes drug-induced homicide like it has othertools of the drug war, we can reasonably expect that theresult will be future cases like James Linder’s, a black manfrom Chicago who is serving 28 years in federal prison afterbeing sentenced by an all-white jury in rural Illinois.3
Executive Summary, cont.Unfortunately, the harms of a highly punitive response todrug use and sales expand far beyond the effects of the actualpunishment. Indeed, criminalizing people who sell and usedrugs, through means like drug-induced homicide charges,amplifies the risk of fatal overdoses and diseases by increasingstigma and marginalization and driving people away fromneeded medical care, treatment, and harm reduction services.On the other hand, proven strategies are available to reducethe harms associated with drug misuse, treat dependenceand addiction, improve immediate overdose responses,enhance public safety, and prevent fatalities. These strategiesinclude expanding access to the life-saving medicinenaloxone and training in how to administer it; enacting andimplementing legal protections that encourage people to callfor medical help for overdose victims; training people howto prevent, recognize, and respond to an overdose; increasingaccess to opioid agonist treatment such as methadone andbuprenorphine, and to other effective, non-coercive drugtreatments; authorizing drug checking and safe consumptionsites; and improving research on promising drug treatments.Each of these strategies has evidence to support itseffectiveness. Drug-induced homicide laws have none.They have not proven successful at either reducing overdosedeaths or curtailing the use or sale of illegal drugs. And yet,ironically, prosecutors and legislators wield this punitivesword with impunity. They are not required to show resultsin support of their faulty rationale, and they are not heldaccountable for utterly wasted resources. We simply cannotlet our elected officials off the hook that easily anymore.Not when it could be your child, friend or, simply, fellowhuman being, who dies from a drug overdose or is lockedup for murder due to our elected officials’ failures to embraceproven, life-saving public health interventions in favor ofwasteful, destructive punishments.4An Overdose Death Is Not Murder: Why Drug-InducedHomicide Laws Are Counterproductive and Inhumane
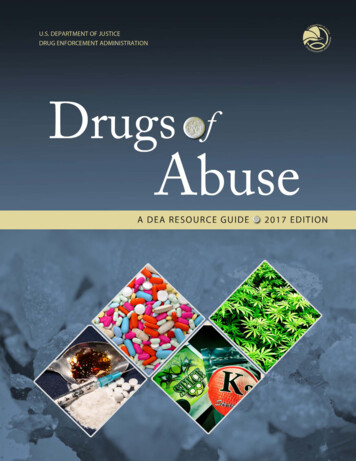
Background: Overdose Crisisand ResponseIncreasing Rates of Opioid OverdoseIn 2015 (the most recent year for which complete data areavailable), drug overdoses accounted for over 52,000 U.S.deaths.1 Provisional data for 2016 put the number of overdosedeaths at over 64,000 – a staggering 22% increase from theyear before.2 From 2000 to 2015 more than half a millionpeople died from drug overdoses.3 The drug overdose deathrate increased significantly from 12.3 per 100,000 peoplein 2010 to 16.3 in 2015.4 Opioids – prescription and illicit– are the main drivers of increases in drug overdose deathsover the past 15 years. Opioids are a class of drugs thatinclude the illicit drug heroin as well as the legal prescriptionpain medications oxycodone (OxyContin ), hydrocodone(Vicodin ), codeine, morphine and others.5 Opioids wereinvolved in more than 33,000 deaths in 2015, accounting forsix out of every ten fatal overdoses, and representing over a200% increase since 2000.6 7Sales, substance treatment admissions, and overdosedeath rates related to prescription opioids have increasedsimultaneously since 1999.8 Moreover, from 1999 to 2011,consumption of hydrocodone more than doubled andconsumption of oxycodone increased by nearly 500%.9In 2014, almost two million Americans were addictedto prescription opioids.10 In 2015, more than 15,000people died from overdoses involving prescription opioids,quadrupling the 1999 rate.11www.drugpolicy.orgBeginning in 2010, heroin overdose fatalities began increasingrapidly across the country while fatal overdoses involvingprescription opioids began to level off and even declinedslightly between 2011 and 2012.12 Between just 2010 and2015, the rate of heroin-related overdose deaths more thanquadrupled.13 From 2014 to 2015 alone, heroin overdosedeath rates increased by 20.6%, with nearly 13,000 peopledying in 2015.14 It is important to note, though, that 77%of prescription opioid overdose deaths and 67% of heroinoverdose deaths are the result of mixing opioids with otherdrugs or alcohol.15The most recent increases in opioid overdose deathsare attributed to illicitly manufactured fentanyl. Whilepharmaceutical fentanyl is a synthetic opioid approved fortreating severe pain,16 illicitly manufactured fentanyl is oftenadded to heroin to cut costs while increasing potency.17The number of overdose deaths involving synthetic opioids,excluding methadone but including fentanyl, increased by72% from 2014 to 2015.18 Roughly 9,500 people died fromoverdoses involving synthetic opioids other than methadonein 2015.19 Provisional data from 2016 indicates that drugdeaths involving fentanyl more than doubled from 2015to 2016.20 Along with other synthetic opioids (other thanmethadone), fentanyl overdoses resulted in 20,145 deaths lastyear, significantly above the 15,446 attributed to heroin or the14,427 attributed to opioid pills alone.215
Background: Overdose Crisis andResponse, cont.Figure 1. CDC Data—Overdose Deaths Involving Opioids, United States, 2000-2015.1110Deaths per 100,000 population987Any Opioid654Commonly Prescribed Opioids(Natural & Semi-SyntheticOpioids and her Synthetic Opioids(e.g. fentanyl, tramadol)2007 2008 2009 20102011Response to Opioid Overdose CrisisWhereas past opioid epidemics were seen primarily interms of low-income African Americans developing anaddiction to heroin, the current epidemic is perceived asdisproportionately affecting white, middle class people whomisuse pharmaceutical opioids.22 Moreover, some of thegreatest increases in heroin use have occurred in demographicgroups with historically low rates: women, the privatelyinsured, and people with higher incomes.2362012201320142015The result, the New York Times has noted, is a “gentler drugwar.”24 Some Republican legislators who long championedpunitive drug war policies, for example, now propose morehumane responses. There has been a renewed emphasison treatment, expanded access to the overdose antidotenaloxone, the passage of Good Samaritan laws that offerprotection to those calling for help during an overdose,and, recently, serious discussions of previously-taboo harmreduction interventions, such as supervised consumptionservices. Nonetheless, drug war strategies persist. Despitemedia attention elsewhere, use of the criminal justice systemcontinues to dominate local, state, and federal responses toincreasing rates of opioid use and overdose.An Overdose Death Is Not Murder: Why Drug-InducedHomicide Laws Are Counterproductive and Inhumane
The Office of National Drug Control Policy has promotedprescription drug monitoring programs and coordinatedfederal-state crackdowns on pain physicians, patients, andillicit sellers.25 The Drug Enforcement Administration (DEA)has aggressively investigated and prosecuted pain physiciansfor prescribing practices viewed as outside the scope oflegitimate medical practice.26 The Obama administrationprioritized “law enforcement efforts to decrease pill mills,drug trafficking and doctor shopping” beginning in 2011.27States have mirrored the federal response to combattingprescription opioid misuse. Unsurprisingly, these responseshave been wholly ineffective at reducing rates of prescriptionopioid use or overdose.Moreover, as people addicted to opioids transition to or enterthe illicit heroin market, they are met with the same “arrestand incarcerate” policies that have been widely recognized asineffective at reducing drug use, causing high rates of relapse,recidivism and re-incarceration.28 Indeed, the criminalizationof drug use is a major driver of incarceration in the UnitedStates. Each year, U.S. law enforcement makes nearly 1.5million drug arrests – more arrests than for all violent crimescombined. The overwhelming majority – more than 80% –are for possession only and involve no violent offense.29 In2015, nearly 40% of drug arrests (more than 570,000 people)were for marijuana possession, and 45% (more than 674,000people) were for possession of drugs other than marijuana.30Just 16% of all drug arrests were for sale or manufacture ofany drug.31 Clearly, the drug war lumbers on notwithstandingwidespread disillusionment with its persistent failures atreducing problematic drug use and protecting public healthand safety. President Trump and Attorney General JeffSessions can be expected to ratchet itup even further.32www.drugpolicy.orgAs overdose rates continue to rise, so do the proportion ofpolicy proposals focused on punishment and retributioninstead of public health and safety. Elected officials unfamiliarwith, or resistant to, harm reduction, prevention, andtreatment interventions are introducing punitive, counterproductive legislative measures in a misguided effort toreduce overdose fatalities. Though their rhetoric may becompassionate, their policies are anything but. They areadopting a law and order approach to solve a public healthcrisis, with devastating consequences.For instance, before 2004, 29 states had permitted peoplewith substance use disorder to be involuntarily committedto treatment, with most of those laws passing in the 1980s.33Since 2004, however, as the overdose crisis started itsupswing, an additional eight states34 have passed involuntarycommitment laws that permit the institutionalization ofpeople who use drugs without their consent, and states withold laws are reinvigorating their enforcement. Pennsylvania,New Jersey, Alabama, Maryland, New Hampshire, andWashington have either introduced involuntary commitmentlaws for the first time or are proposing changes to existinglaws in order to make commitment less difficult.35 In NewHampshire and Washington, the bills provide for involuntarycommitment specifically as applied to opioid use.36 Inaddition, since just November 2015, 25 states have passedlegislation to increase various fentanyl-related penalties.37Perhaps most draconian of all, prosecutors are increasinglycharging people who supply the drug that contributes toan overdose death with murder or manslaughter underdecades-old drug-induced homicide laws. Politicians arealso introducing legislation to establish new drug-inducedhomicide laws or to increase penalties for drug-inducedhomicide laws already on the books, with one federal proposalgoing so far as to call for the death penalty.387
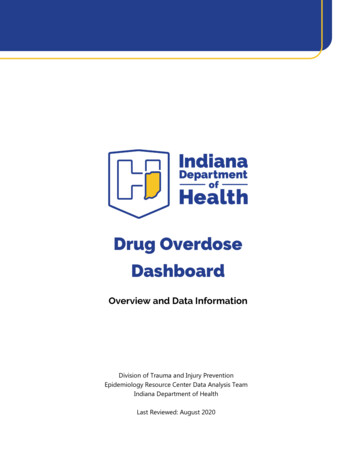
Drug-Induced Homicide:A Legal OverviewFederal and State Laws“Drug-induced homicide” broadly refers to a criminaloffense wherein the illegal manufacture, sale, distribution, ordelivery of a controlled substance that causes death results ina specific charge, usually manslaughter or murder. The federallaw, passed in 1986 as part of the Controlled SubstancesAct, provides a penalty of 20 years to life for anyone whodispenses a controlled substance that results in death orserious bodily injury.39 Currently, 20 states40 – Colorado,Delaware, Florida, Illinois, Kansas, Louisiana, Michigan,Minnesota, New Hampshire, New Jersey, North Carolina,Oklahoma, Pennsylvania, Rhode Island, Tennessee, Vermont,Washington, West Virginia, Wisconsin, and Wyoming –also have drug-induced homicide laws on the books thatcould be used to charge someone who delivers a drug thatresults in an accidental overdose death (see Appendix A).The Colorado, Rhode Island, and Wyoming laws, however,are limited to those who deliver a controlled substance toa person under the age of 18. State law penalties vary fromtwo years to capital punishment. In six states – Colorado,Florida, Louisiana, Oklahoma, Rhode Island, and WestVirginia – the minimum penalty is life in prison. A host ofother states, while without specific drug-induced homicidestatutes, still charge the offense under various felony-murder,depraved heart, or involuntary or voluntary manslaughterlaws (see Appendix A).Map 1. DIH Laws8An Overdose Death Is Not Murder: Why Drug-InducedHomicide Laws Are Counterproductive and Inhumane
Legislative HistoryLegal ChallengesEvidence of the legislative intent behind these statutes isscarce. From the legislative history that does exist, however,we know that some state legislatures emphasized theimportance of punishing major drug suppliers. The Vermontstatute penalizing the sale or dispensation of a drug resultingin death, for instance, explicitly states: “Many people whobecome addicted to illegal drugs resort to small-scale sale ofdrugs to support their addiction. This act is not directed atthose people, but rather at the entrepreneurial drug dealerswho traffic in large amounts of illegal drugs for profit.”41 TheNew Jersey statute was similarly intended to penalize so-calleddrug “kingpins”:Opponents of drug-induced homicide statutes have arguedthat such laws are unconstitutional, primarily because theyare vague with respect to whom the law is intended to cover,the required mental state of the defendant when committingthe prohibited act, and the tenuous connection betweenthe delivery of the controlled substance and the host ofother factors that often contribute to death. Courts haverejected these challenges, however, largely in efforts to avoiddetermining the constitutionality of the law. The case ofPeople v. Boand44 is illustrative.[The statute] must target for expedited prosecution and enhancedpunishment those repeat drug offenders and upper echelonmembers of organized narcotics trafficking networks who posethe greatest danger to society. In order to ensure the most efficientand effective dedication of limited investigative, prosecutorial,judicial and correctional resources, it is the policy of this State todistinguish between drug offenders based on the seriousness of theoffense, considering principally the nature, quality and purity ofthe controlled substance and the role of the actor in the overalldrug distribution network. It is the intention of the legislature toprovide for the strict punishment, deterrence and incapacitationof the most culpable and dangerous drug offenders, and tofacilitate the rehabilitation of drug dependent persons.42Other states more explicitly focused on the potential deterrentfactor of the law, whether applied to “upper echelon”manufacture and distribution or low-level exchanges. InMichigan, one argument in support of the legislation positedthat “perhaps friends, acquaintances, and drug dealersalike would think twice about selling or providing drugs toanother if faced with life imprisonment should that friend,acquaintance, or customer die.”43www.drugpolicy.orgThe defendant in Boand first argued the drug-inducedhomicide statute was unconstitutionally vague because thelegislature intended the statute “to stop drug traffickers, theprofessional drug dealers,” but the law held liable anyone whodelivered a controlled substance, even the lowest-level personin a drug supply chain.45 The court responded that the plainlanguage of the statute criminalized the “delivery” of drugsand defined “delivery” to include any transfer of a controlledsubstance whatsoever, so the law was not unconstitutionallyvague – the law gave citizens notice that any drug transfercould potentially incur liability.46The defendant next argued the statute was unconstitutionallyvague because it did not specify what mental state wasrequired to incur liability (most criminal laws specify a mentalstate a defendant must have when performing the prohibitedact in order to incur liability).47 The court responded thatthe drug-induced homicide statute imposed liability when adeath occurred as a result of someone violating the IllinoisControlled Substances Act, and that because that Actprohibited the knowing delivery of a drug, the drug-inducedhomicide statute incorporated the “knowing” mental stateas well.48 Drug-induced homicide statutes that impose strictliability – that expressly state a defendant will be held liablefor the conduct regardless of mental state (even if the conductwas done unintentionally or unwittingly) – have also widelybeen upheld.499
Drug-Induced Homicide:A Legal Overview, cont.Finally, the defendant argued the statute wasunconstitutionally vague because it did not specify howdirectly the drug delivery had to cause the death in orderfor the defendant to be held liable.50 In other words, thedefendant argued that the statute was too vague because aperson would not know whether he or she would be heldliable for delivery of drugs that were remotely related to adeath – say, if the defendant delivered drugs to someone whoused them, decided to partake in a dangerous activity whileintoxicated, and then died from the activity rather than thedrugs themselves.The court, in response, imputed the causality requirementfrom the similar felony-murder statute into the drug-inducedhomicide statute, and held that liability would only beimposed if the delivery of the drugs “proximately caused”the death.51 Felony murder is a legal doctrine that imposesmurder liability for a death that occurs in the commission ofa felony, even if the killing is unintentional. Under bothfelony murder and drug-induced homicide, “proximate cause”refers to an action or event that results directly and foreseeablyin a result, sufficiently enough that it can legally be consideredthe cause of that result. The argument that “proximate cause”is lacking in drug-induced homicide cases is the strongestof the vagueness claims, but the widespread acceptance ofthe felony-murder doctrine – which often requires a minimalshowing of proximate cause, if any – suggests courts wouldlikely not overturn drug-induced homicide statutes onthese grounds.5210Though legal challenges like Boand and others have beenunsuccessful, their failure is not due to meritless arguments.Rather, the doctrine of constitutional avoidance largely shieldsthese statutes from judicial intervention. Under the doctrineof constitutional avoidance, a court faced with an ambiguousstatute must read the law to be constitutional if any suchinterpretation is reasonably plausible, even if the most naturalinterpretation is unconstitutional.53 The Boand court, forinstance, invoked constitutional avoidance in considering thecausation challenge. Even though the most natural readingof the statute contai
acquaintances, and people who sell small amounts of drugs, often to support their own drug addiction. Despite police and prosecutor promises to go after upper echelon drug manufacturers and distributors, that rarely happens. Out of the 32 drug-induced homicide prosecutions identified by the New Jersey Law Journal in the early 2000s, 25 involved