Transcription
Developmental Trauma:Child Advocacy CenterHope Changes Everything ConferenceWhat is “Stress” any uncomfortable "emotional experience accompanied bypredictable biochemical, physiological and behavioral changes."APA Dave Melnick, LICSWNortheastern Family Institute, Vermont (NFI)StressWhat is Trauma Trauma is an unexpected, body based event or experience thatoverwhelms a person’s ability to elopmental Trauma:(focus on interpersonal trauma)1.It is an Event, Experience and EffectVulnerabilityMultiple incidents of trauma, over longperiods of time2. Perpetrator is within the child’s intimate circleof adults: “The Care-giving System”Traumatic Stress:Signature Clinical IssuesWhat was adaptive (survival behavior) at the timeof the trauma, is now maladaptive when the threat(objective) no longer exists.3. The 7 Domains of Impairment1
Stress Response System:FFFFTraumatic Stress:Signature Clinical Issues“The alarm system for the emotional body is fear”“Being traumatized means continuing to organizeyour life as if the trauma were still going on—unchanged and immutable—as every newencounter or event is contaminated by the past”—van der KolkFightFEARFlightFreezeAdapted from "The Mastery of Love" DonMiguel RuizTrauma Informed Systems“A Trauma-informed System Realizes the widespread impact of trauma and understandspotential paths for recovery; Recognizes the signs and symptoms of trauma in clients,families, staff, and others involved with the system; and Responds by fully integrating knowledge about trauma intopolicies, procedures, and practices, and seeks to actively resist retraumatization.” Restorative--SAMSATrauma-Informed Systems:Primary ResourcesGeneral Concepts: Trauma-informedAdult Assets of the Caregiver1.1. National Child Traumatic Stress Network:http://www.nctsn.org/2. UCSF HEARTS: http://www.coe.ucsf.edu/coe/spotlight/ucsf hearts story.html3. The Sanctuary Model: http://www.sanctuaryweb.com4. THRIVE Maine: http://thriveinitiative.org5. SAMSA: http://www.samhsa.gov6. The Trauma-Informed Care Project:http://www.traumainformedcareproject.org7. Child Welfare Information ding/trauma/2.3.A resilient sense of self: Open minded Self reflective Curious, even when stressed Acceptance of emotional discomfort Ability to enjoy youthOffer a secure base: with an understanding of child development andtrauma Identify attachment patterns and child's miscues Being sensitive and able to challenge MindfulRelational capacity: ability to build and sustain relationship especiallyin times of stress Balance of authoritative and warm Setting good boundaries Attunement Capacity to connect with emotional distress Reparative focus4. Ability to manage behavior connect then correct Flexible response patterns Good impulse control Attune to internal experience whilemisbehavior is occurring5. Ability to handle rejection6. Willingness and openness to exploring ownattachment history7. Engaged in a reflective practiceAdapted from: "Assessing Adoptive andFoster Parents" Alper and Howe2
The Impact of Developmental Trauma:NCTSN: The 7 Domains of Impairment1.2.3.4.5.6.7.Impact of Developmental Trauma:Domain #1: Physical Health(Brain and Body)Physical Health: Body and BrainAttachment & RelationshipsEmotion ResponsesThinking and LearningBehavioral ControlDissociationSelf-Concept & FutureNational Child Traumatic Stress Network:Seven Domains of ImpairmentOrientationWe don’t truly know ourselves unless we canfeel and interpret our physical sensations”(Bessel van der Kolk, MDhttp://www.nctsn.org/The Brain: Form and FunctionThe Brain: Form and FunctionAreas of the BrainAreas of the BrainNeocortex: Logic & ReasonPrimary Strategy:Logic and ReasonLimbic: Relationship & Emotions:Primary Strategy:RelationshipPrimary Strategy:Co-RegulateHousekeeping FunctionsReptilian: Survival NFI Vermont 2016 NFI Vermont 2016adapted from materials by www.ChildTrauma.orgadapted from materials by www.ChildTrauma.org3
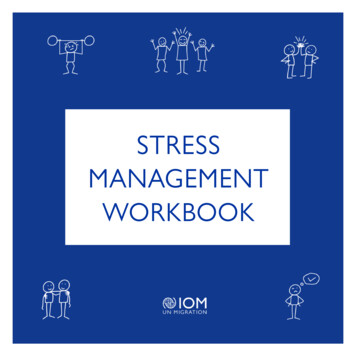
Percentage of available resources:Regulated ChildPercentage of available resources:Distressed/Alarmed/Reactive Child50%30%30%50%SurvivingSurviving20%20% NFI Vermont 2016 NFI Vermont 2016Percentage of available resources:Dysregulated/Reflexive ChildInterventionsNeocortex: Logic & Reason10%40%Surviving50% NFI Vermont 2016 NFI Vermont 2016adapted from materials by rtex: Logic & ReasonNeocortex: Logic & ReasonLimbic: Relationship & Emotions:Limbic: Relationship & Emotions: PACE Validation Movement,breathing Sensory breaks The 4 “R’s“ Rhythms andsynchrony Touch Get to YesReptilian: Survival Reptilian: Survival NFI Vermont 2016Physical HoldMovementPhysical contactEmpathyCo-regulationSilenceAdult affect regulation NFI Vermont 2016adapted from materials by www.ChildTrauma.orgadapted from materials by www.ChildTrauma.org4
Interventions The Brain on DessertNeocortex: Logic & ReasonCBT/DBTPrior behavior reference pointsContingency planningPoint/level systemsFBALimbic: Relationship & Emotions: PACE Validation Movement,breathing Sensory breaks The 4 “R’s“ Get to Yes!Reptilian: Survival NFI Vermont 2016MovementPhysical contactEmpathyCo-regulationSilenceAdult affect regulationadapted from materials by www.ChildTrauma.orgAdditional strategies:PACE (Dan Hughes, PhD.)Strategies: Biology and Brain1. Congruence and “matching systemsPlayfulness:2. Provide a coherent and predictable response to their stress:Acceptance/Attunement:3. Enriched Relational Experiences: This leads to co-regulation4. Get to Yes!5. Rhythm and Movement6. Mindfulness Generates hope Reduces resistance/shame and increases joy/pleasure Authenticates experienceBreeds connection before correctionCuriosity: Decreases defensive positioningHelps caregivers inhibit their first reactions to a teen.Empathy: Cannot exist at the same time as anger—cannot co-existEmotional and body based experienceauthenticates NFI Vermont 2016Impact of Developmental Trauma:Domain #2: Attachment and RelationshipDomain #2: Attachment and RelationshipGeneral Concepts ‘The emotional energy that lives in our home (as young children) is going to tune ouremotional body to that frequency” Ruiz page 33 Relationship are the “firewall” that pretends the virus of trauma from spreadingthroughout all three operating systems of our brains We must create a disparity between what the child expects (the rhythm of his earlylife) and your caregiving/professional rhythm We must be “bigger, stronger, wiser and kind (circle of security) Lieberman“Being able to feel safe with other people is probably thesingle most important aspect of mental health” van der Kolk NFI Vermont 20165
Healthy Attachment Sequence:Unhealthy Attachment:physical or psychological onState of higharousalMental MapsOrRoad Mapsphysical or psychological needActivation ofthe “StressResponse System”Insecurity & Self DoubtMistrustShamePoor Self-RegulationState of high Arousal“Road Map”Attunement/satisfaction of needNeeds are disregarded/attunement disrupted(Beverly James)(Beverly James) NFI-Vermont, 2013Domain #2: Attachment and RelationshipReenactmentsWhy negative reenactments occurs: (Sandra Bloom)1.Disrupted attachments: 2.direct request for comfort were not met.Child learns to indirectly signal for what they need.State Dependent Learning: The adult ‘help’ often repeats past patterns4.The Addictive Potential of Arousal:5.Loss of Language: trauma can be speechless.6.Guilt and shame: 1. Over-reactive to nonverbal comm. Poorly evaluate the client’s intentions3. The stress activates a defensivestance: Become at odds with your client (competitive,angry),the child’s original action plan did not stop the trauma.The persons signals are misread by others and ‘are often responded to in ways that directly counter what the traumatized person requires in order tochange”.Strategies: Attachment1.(Dan Hughes, Ph.D & JonBaylin, Ph.D.)fear becomes deeply imbedded in child’s minds This emotion memory is outside of his/her conscious awareness.A trauma trigger provokes a behavioral sequence from the child that originated in the “context of something frightening or life threatening” “The reward is temporary relief of the fear” p.763.Professionals: Impact of Stress2. Experience their client as a threatFear Conditioning: “Reenactment” NFI-Vermont, 2013Impact of Developmental Trauma:Domain #3 Emotion ResponsesAdult Affect Regulation: You must be able to understand and feel your own emotions in order to empathize with others Traumatized youth are highly influenced by the affect state of adults2.Attunement: Create a “we state”: Relationships mediate stress3.4.5.6.Enriched relationship: recreate purposeful interactional patterns ofcontinuity, trust, containment. Be “bigger, stronger, wise and kind”Co-regulate affectMinimize/Prevent Reenactment: Deconstruct the relational patternsto understand what the child is playing out. It takes time.“ Stage Not Age”—the child’s functional age is driven by the stressresponse system and self-regulation ability Brandt NFI-Vermont, 20136
Emotion RegulationFunction of Emotions:Self-Regulation:1. Tell us what is meaningful2. Readies us for actionCatalogue ofpriorexperienceAttunement/MisattunementBody BasedAwarenessEmotionResponse3. “Evokes Motion”Adapted From: "Working with EmotionalIntelligence", Daniel GolemanHow Trauma Effects EmotionRegulationEmotion RegulationOur initial decisions are made by gut feelings and we cannot “dictate” what we aregoing to feelDissociation:Retreat from the external sensory world We cannot control our emotions or initial physiological response. We can controlour response to these emotions and physiology. This is what is meant by emotionregulation.Anger mobilizes energy and focuses attention to remove an obstacle to achieve agoal.–Anger is a motor experience while empathy is a sensory/attachment experience NFI Vermont 2016Common Forms: Avoidance, Refusals, Indifference ‘Spaced out’, inattentive, ‘trance like’, stilling, mental escape,detached, not embodied, numbing Surrender, Possum, Capitulate, Retreat and Defeat, Submissive,obedience, feigned death, collapse Helpless, freezing, indifferent, apathy, passive, victim, lifeless NFI Vermont 2016Getting to YesEmotion Regulation: Strategies:1. Getting To Yes!2. .and “Listen more and Lecture Less“people behave their worst when they feel the most powerless” (Mark Goulston, MD)Goal:Method:1.Step #1: Make Contact:Help move a brain frompanic to control. Thisgives the cortex a “toehold” and you can . “I bet you feel that nobody really understands just how .” “It sounds like you think I ” “I bet you think that I am trying to ” ”It sounds as though you think that nobodyunderstands you”Step #2: Name it 1. “It seems that you are .is that correct?”Step #3: “Scale it” “How are you right now”?7
Getting to YesEmotion Regulation: Strategies:“people behave their worst when they feel the most powerless” (Mark Goulston, MD)Step #4: Link it3.Mindfulness: “The reason you are so is because , do I have that right”. Build abridge from cause—to—effectshifts our brains emotional “set point” to attend to inner states and not just outer states (hypervigilance to inner awareness).4. Mental rehearsal: Step #5: Solve it How can I help? What part can I playing. What can you do to .activates the same neuronal activity as the real activity—imagine and practice a different outcome.5.Watch the “somatic narrative”6.Tell child what they can do, not what they cant7.Neutralize: Take the energy out of the interaction8.Give ChoicesStep #6: Relate and Connect9.Step #7: Reflect and Plan10. Change sensory experience: move, breathe, stretch, music.Promote reflective practice with clients:oooWhat do you need?What is your plan?What are you noticing right now? NFI Vermont 2016Impact of Developmental Trauma:Domain #4 Cognition and LearningImpact of Developmental Trauma on CognitiveDevelopment:1.2.3.4.5.6.7.8.9.Black and white thinkingPoor cause and effectDifficulty sustaining curiosity and attentionNegative belief systemCant filter out irrelevant informationIntellectual functioning- Often varied cognitive profilesDelayed or disrupted language developmentDifficulty with executive functioningMemory challenges (distraction, misperception, poor short-termmemory, overwhelmed, anxiety)9. Focus on non-verbal information and lack of ability to accurately NFI Vermont 2016Impact Areas:CognitionIt is not often the task or request that leadsthe person toMisbehave It is the feeling and negative thoughts thatis evokes Helpful Reframes for professionals:Client Says:Client Believes:“this is stupid”“I cant do this”“You’re an“why do you always ”“I’m outta here”“I am stupid”“I am helpless/powerless”“ I am not safe”“ I am to blame”“ I am powerless to changehow I am feeling”“ I can’t do this”“I am weak and vulnerable”“I won’t do this”“You can’t make me” NFI Vermont 2016 NFI Vermont 20168
Impact Areas: Common NegativeCognitionsI am stupidI am unlovableI am worthlessStrategies for addressing problems withCognition and Learning1.2.3.4.5.6.“Regulate before you educate”Stress ManagementAddress the cognitive “self-evaluations” before the external behaviorswhen you can.Client may require scaffolding to support executive functioning challengesMany clients will need multi-disciplinary services to address learningneedsPredictability and Routines will rule the dayI am powerless, out of control, vulnerableI am not safe NFI Vermont 2016 NFI-Vermont, 2013Impact of Developmental Trauma:Domain #5: Behavioral ControlImpact of Developmental Trauma:Domain #5: Behavioral Control“Hurt People Hurt Other People” (Bloom)Behavioral Interventions:General Considerations1. Behavior modification/management does not typically recognize the reciprocal nature of anger andexchange of affect:“Co-constructed”2. Misbehaviors are strategies for self-protectionBehavioral Interventions:General Considerations Behavior modification/management does not typicallyrecognize the reciprocal nature of anger and exchange ofaffect:“Co-constructed”3. “Acting out is a form of remembering” (Lieberman)4. challenging behaviors represent deficits with: Misbehaviors are strategies for self-protectionLanguage and communicationAttention and working memoryEmotion and self-regulationCognitive flexibilitySocial thinking“Acting out is a form of remembering” Lieberman5. Challenging behaviors are highly predictable NFI Vermont 2016 NFI Vermont 20169
Behavioral Interventions:General Considerations If professionals are not careful, and activate the client’s defensive systeminstead of the social engagement then behavioral problems may escalate.Behavioral Interventions:General Considerations Make sure you know the intention of the behavior: related to survival Skill deficit and unmet need Professionals are most competent when open-minded: this enhances selfregulating, creativity and attunement. Some of the professional—client problems that emerge, emerge from within theprofessional—client relationship and are not merely “behavioral” Discipline is not an ideal way to establish a relationship with a client. NFI Vermont 2016 Sensory seeking or avoiding Traumatized adults have to be mistrustful before they cantrust. Any evaluative process creates a defensive position (even praise) NFI Vermont 2016Emotion Regulation:Window of Tolerance (Pat Ogden, Ph.D.)“The cure for the pain is in the pain” RumiBehavioral Plans vs. Emotion Regulation plansBehavioral PlansCo-regulation Plans Tend to be responsive andpreventative Focuses on and builds emotionalregulation Focus on emotional well-beingof the person Focus on “mutual” regulation Addresses the underlyingfunction of the behavior Helps person learn how otherscan helpTend to be reactiveFocus on behavior managementFocus on reduction of behaviorsLittle or no focus on partnerbehavior May not be developmentallyappropriate Focuses on superficialantecedents and consequencesof the behavior Less focused on earlyintervention and preventive skillbuildingBased on the work of Nancy Clements, M.A., CCC–SLP; Socialthinking.comDifferential Diagnosis of DevelopmentalTrauma and Bipolar Disorder shares some qualities of impulsivity,affect dysregulation and breaks inreality The associated impulsivity does nothave a tension reduction goal Affect dysregulation (of even rapidcycling BD) occurs much slower Psychotic symptoms are moodcongruent Less interpersonal impairment Generally respond well to disorderspecific treatmentDevelopmental Trauma shares some qualities of impulsivity, affectdysregulation and breaks in reality The associated impulsivity does have thegoal of reducing tension Affect dysregulation can be moment tomoment Psychotic symptoms associated withfragmentation, depersonalization Impaired personal functioning and alteredexpectations of others Do not respond well to disorder specifictreatment (when diagnoses with BP andtrauma history), but respond well to traumainformed practices.From: Understanding Interpersonal Trauma in children”, in Am J or Orthopsychiatry. W. D 'Andrea et. al.Differential Diagnosis of DevelopmentalTrauma and ADHD:Developmental Trauma: Includes deficits in attention,hyperactivity and impulsivity Similar deficits possible with differentetiology and presentation (inattentionrelated to dissociation, freeze response) May engage in risky behaviorthrough dysregulated impulses Inattention and hyperactivity notthought to result from emotionaldistress Not typically characterized byaffective, relational or somaticdysregulation Generally respond well to disorderspecific treatment May engage in risky behavior because ofaffective instability and attempts to selfsoothe Inattention and hyperactivity often resultsfrom emotional distress Often characterized by affective, relationalor somatic dysregulation Do not respond well to disorder specifictreatment (when diagnoses with BP andtrauma history), but respond well totrauma-informed practices.From: Understanding Interpersonal Trauma in children”, in Am J or Orthopsychiatry. W. D 'Andrea et. al.10
Resources:Authors to Read1.2.3.4.5.6.7.8.9.10.11.12.Bruce PerryDaniel HughesPat OgdenDaniel SiegelAlan N. SchoreStephen PorgesBessel van der KolkDiana FoshaJoseph LeDouxEd TronickJudith HermanBeverly JamesWebsites to Visit http://www.childtrauma.org http://www.traumacenter.org/index.php http://learn.nctsn.org/ http://www.nctsn.org/ http://www.trauma-pages.com/ http://www.nfivermont.org NFI-Vermont, 201311
Adapted from "The Mastery of Love" Don Miguel Ruiz Fight Flight Freeze FEAR "A Trauma-informed System Realizes the widespread impact of trauma and understands potential paths for recovery; Recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system; and