Transcription
AcalltoactionImproving clinician wellbeingand patient care and safety1February 2020
TMAcknowledgmentsThe Health Policy Institute of Ohio partnered withThe Ohio State University College of Nursing HeleneFuld Health Trust National Institute for Evidencebased Practice in Nursing and Healthcare to createA Call to Action: Improving Clinician Wellbeing andPatient Care and Safety.HPIOAuthorsMolly Schmidt, MA candidateReem Aly, JD, MHAData analysis leadZach Reat, MPAGraphic design and layoutNick Wiselogel, MAContributorsHailey Akah, JD, MABecky Carroll, MPAAmy Bush Stevens, MSW, MPHAlana Clark-Kirk, BAAirregina Clay, MPAL candidateAmy Rohling McGee, MSWJacob Santiago, MSW candidateThe Ohio State University College of NursingHelene Fuld Health Trust National Institutefor Evidence-based Practice in Nursing andHealthcareBernadette Mazurek Melnyk, PhD, APRN-CNP,EBP-C, FAANP, FNAP, FAAN, Vice President forhealth promotion, University Chief Wellness Officer,Dean of the College of Nursing and ExecutiveDirector, Fuld InstituteLaurel Van Dromme, MAStakeholder engagementThis project was informed by a multi-stakeholderAdvisory Committee made up of representativesfrom public and private organizations. This brief wasalso informed by interviews with state and nationalsubject matter experts listed below: Lesly Kelly, CommonSpirit Health and ArizonaState University Susan B. Hassmiller, Robert Wood JohnsonFoundation Arthur S. Hengerer, Co-Lead on NationalAcademy of Medicine’s Action Collaborative onClinician Well-Being and Resilience Michael B. Holliday, University of CincinnatiCollege of Medicine Joe Rotella, American Academy of Hospice andPalliative Medicine Amy Witkoski Stimpfel, New York University RoryMeyers College of NursingThis brief builds on the work of the NationalAcademy of Medicine’s Action Collaborative onClinician Well-Being and Resilience. The ActionCollaborative’s recent report, Taking ActionAgainst Clinician Burnout: A Systems Approach toProfessional Well-Being, informed the developmentof this brief and is referenced throughout.A lcalto ionactngellbeiian w safetydclinicoving nt care anImprpatieandDownload the full report and access the resource page atwww.hpio.net/a-call-to-action/Note: Blue, bolded text throughout this report indicate hyperlinks in the electronic version2
OverviewA growing body of research indicates that healthcareclinicians are facing serious problems related totheir overall health and wellbeing. This includesexperiencing relatively high rates of burnout,depression, addiction and suicide.Poor wellbeing also impacts a clinician’s ability toprovide high-quality care by increasing medicalerrors and unsafe prescribing behaviors, decreasingempathy and compromising patient-centeredinteractions. At the same time, when care andtreatment do not go as planned, clinicians facetrauma and despair that threatens their health.This brief serves as a call to action to improve clinicianwellbeing and its impacts on patient care and safety,providing a: Framework for the relationship between clinicianwellbeing and patient care and safety Summary of research findings Review of evidence-informed policies, programsand practices that improve clinician wellbeing andsupport high-quality, safe patient care Set of evidence-informed state policy optionsFocus of this briefThe term “clinician,” used throughout this brief,includes members of the healthcare team thatprovide direct patient care. Much of the researchon clinician wellbeing in the United States focuseson physicians, with emerging research on nurses,pharmacists and clinicians in educational orresidency programs (health professional students).Far fewer research studies have focused on thehealth and wellbeing of other clinicians. Becauseof these gaps in research, this brief focuses primarilyon findings for physicians, nurses and pharmacists.However, findings from this brief can also be appliedto other clinicians within the healthcare team.Throughout the literature, the terms “wellbeing,”“wellness” and “health” are used to describeclinician wellbeing. Each of these terms are usedthroughout this brief.In addition, this brief focuses on state-level policies,programs and practices that can improve clinicianwellbeing. Much of the data and informationprovided in this brief is derived from nationalresearch studies and findings. When possible, Ohiospecific data or programs are also highlighted.3key takeaways forstate policymakers andhealthcare leaders1. There is a bidirectional relationship betweenclinician wellbeing and patient careand safety (see figure 1). There are alsomediating factors that impact clinician andpatient outcomes.2. Clinicians face serious problems related totheir overall health and wellbeing, includinghigh rates of burnout, depression, addictionand suicide. This contributes to poor patientoutcomes and is associated with high costsdue to increased clinician absenteeism,presenteeism, turnover and lost productivity.3. Improving outcomes for clinicians andhealth professional students requires acomprehensive approach that provides acontinuum of prevention, treatment andrecovery supports. This includes establishinga positive organizational culture thatsupports wellness, implementing evidenceinformed policies and programs andimproving access to mental health andaddiction treatment and recovery supports.Inside1. Overview — 32. What is the relationshipbetween clinician wellbeingand patient care and safety?—43. What is the scope of theproblem? — 84. What can be done toimprove clinician wellbeingand improve patient careand safety? — 115. Evidence-informed policyoptions for improvement — 193
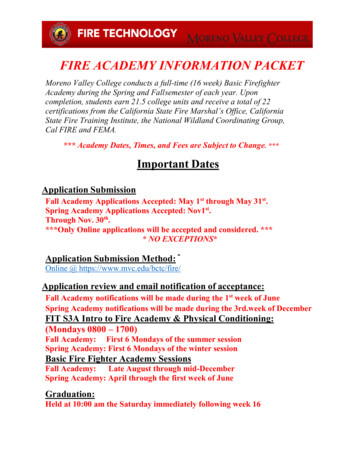
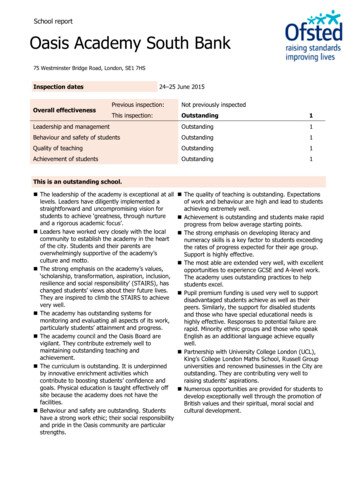
What is the relationship betweenclinician wellbeing and patient careand safety?Understanding the relationship between clinicianwellbeing and patient care and safety enables statepolicymakers and healthcare leaders to allocateresources, implement programs and develop policiesthat effectively improve both clinician and patientoutcomes.Figure 1 outlines a bidirectional relationship betweenclinician wellbeing and patient care and safety:1. Improving clinician wellbeing, including preventingand treating burnout, mental health conditions andaddiction, improves patient care and safety.2. Improving patient care and safety, includingdecreasing rates of medical errors and adversepatient events, improves clinician wellbeing.Impact of clinician wellbeing on patient careand safetyOverall wellbeing, including mental, physical,social and emotional health, impacts a clinician’sperformance. Poor wellbeing impacts a clinician’sability to provide high-quality care by increasingmedical errors and unsafe prescribing behaviors,decreasing empathy and compromising patientcentered interactions.BurnoutBurnout is a severe type of work-place stresscharacterized by emotional exhaustion, cynicismand a reduced sense of personal accomplishment.4Research identifies burnout as a significant threat tosafe, high-quality patient care, leading to decreasedwork effectiveness and performance among clinicians,an increase in medical errors and decreased patientsatisfaction.5Figure 1. The relationship between clinician wellbeing and patient care and safetyImproving clinician wellbeing, including preventing andtreating burnout, mental health conditions and addiction,improves patient care and safetyClinicianwellbeingExamples of the impactof improved patient careand safety on clinicianwellbeing: Reduced traumaassociated with secondvictim phenomenon* Decreased clinicianstress Decreased clinicianburnout Decreased depression Increased clinicianaccountability High-functioning clinicalcare teamMediating factors Laws, rules, regulations and the role of statepolicymakers, including legislators, state agenciesand state health professional licensing boards Societal or cultural norms, including the role ofracism, discrimination, stigma and other biases Organizational culture, including a focus on wellness Clinical environment, including health informationtechnology, documenation and administrativeresponsibilities Research and data, including collection,compilation and reporting of factors that impactclinician wellbeing Personal factors, including social support, familyissues and socioeconomic concerns, among othersPatientcare andsafetyExamples of the impactof improved clinicianwellbeing on patientcare and safety: Increased quality ofpatient-centeredinteractions Decreased medicalerrors Safe prescribing DecreasedcomplicationsImproving patient care and safety, includingdecreasing rates of medical errors and adversepatient events, improves clinician wellbeing.*Second victim phenomenon: Psychological trauma endured by clinicians after being involved in an adverse event (Stehman, et al, 2019)Note: Framework informed by literature review conducted by the Health Policy Institute of Ohio and the National Academy of Medicine ActionCollaborative on Clinician Well-Being and Resilience’s Factors Affecting Clinician Well-Being and Resilience – Conceptual Model (2018).4
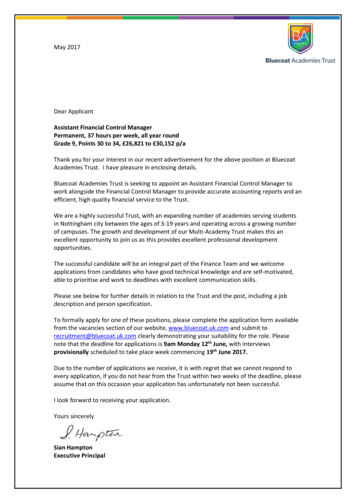
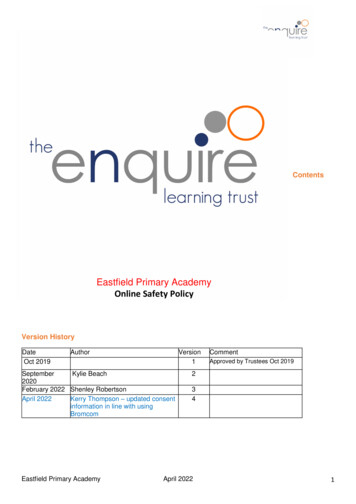
Much of the research on burnout focuses on its linkto increased medical errors among clinicians: A 2018 study published in Mayo ClinicProceedings showed that physicians, acrossspecialties, who showed signs of burnout were2.2 times more likely to report a perceivedmedical error.6 The findings suggest burnout, poorwellbeing and perceptions of poor safety areassociated with major medical errors.7 A 2012 study published in the American Journalof Infection Control found that high nurse burnoutwas associated with a higher rate of patientinfections.8In addition to being harmful to the clinician anda threat to patient care and safety, burnout isexpensive for hospitals and health systems. A2019 cost-consequence analysis, published in theAnnals of Internal Medicine, found that turnoverassociated with physician burnout can cost anorganization approximately 7,600 per physician,per year.9DepressionDepression in clinicians is associated with poorpatient care.10 Several studies have demonstratedthat clinicians experiencing depression are morelikely to make medical errors. Sometimes thesemedical errors are due to presenteeism, which iswhen workers are physically present at work but arenot functioning to the best of their abilities due totheir mental or physical health. For example: Of the physicians surveyed by Medscape forthe National Physician Burnout, Depression andSuicide Report 2019, 35% of physicians who aredepressed say they are easily exasperated withpatients, 26% say they are less careful with patientnotes and 14% say they make errors they mightnot normally make.11 A 2018 cross-sectional survey of U.S. nurses, whichdescribed the relationship between nurses’ healthand medical errors, found that nurses with poorhealth have a 26% (at best) to a 71% (at worst)higher likelihood of making medical errors.12The study found depression to be the strongestpredictor of medical errors.13 A 2017 prospective longitudinal study observedresident interns from 55 universities throughout theU.S. and found that depressive systems amonginterns was strongly linked to presenteeism.14 Thestudy estimated that, across all residents workingin the U.S., depression-related presenteeism addsan additional 1,226,142,642 to U.S. healthcarecosts.15 A 2016 literature review found that depressionamong registered nurses is linked to increasesin presenteeism, and nurses who reportpresenteeism are more likely to report moreBurnout, racism and discriminationResearch suggests that a clinician’sempathy, compassion and professionalismmay be compromised by burnout.16 Thenegative emotional state associated withburnout can increase a clinician’s expressionof racial prejudice towards their patients,impacting the quality of care they provide.A 2019 study published in JAMA NetworkOpen followed U.S. medical students andresident physicians from 2010 through 2017.Among resident physicians, symptoms ofburnout were associated with greater racialbias, specifically in non-black physicianstoward black patients.17 Other studies haveshown non-black physicians with higher biastoward black patients have fewer patientcentered interactions, leading to distrust andnon-adherence to treatment among theirblack patients.18medication errors, patient falls and overall poorerquality of patient care.19 A 2010 study from the Mayo Clinic, whichsurveyed over 7,900 American surgeons, showeddepression was among the strongest factorsassociated with reporting a major medical error.20Addiction and substance useState regulatory boards frequently take disciplinaryaction against clinicians for substance use thatimpairs their ability to practice. Ohio-specific datais highlighted below to indicate the scope of thisissue.As of June 30, 2019, the State Medical Board ofOhio (SMBO) regulates 88,039 active licenses.21In state fiscal year (SFY) 2019, the SMBO initiateddisciplinary action against 135 clinicians. The largestpercent of these disciplinary actions (27%) wereon the basis of clinician impairment (i.e., “habitualor excessive use or abuse of drugs, alcohol orother substances that impair ability to practice”).22Impairment has been the most common reason fordisciplinary action through the SMBO over the pastfive years (see figure 2).For clinicians licensed through the Ohio Boardof Nursing, 750 complaints (10%) were made onthe basis of drug or alcohol use in SFY 2019.23Additionally, the Ohio Board of Pharmacy opened249 new disciplinary cases on the basis of theftof drugs, 206 for deception to obtain dangerousdrugs, 133 for questionable prescribing and 58for questionable dispensing in SFY 2019.24 Details5
Figure 2. Top reasons for disciplinary action, State Medical Board of Ohio, state fiscalyear (SFY) 2015-2019SFY2019(n 135)SFY2018(n 114)SFY2017(n 165)SFY2016(n 200)SFY2015(n 156)Impairment (e.g., due to drugs, alcohol, orother substances)27%32%28%25%35%Prescribing issues25%27%19%20%19%Criminal acts/convictions17%8%14%13%12%Actions by other boards or agencies12%10%10%8%11%Top reasons for disciplinary actionNote: Impairment for the State Medical Board of Ohio is defined in the Ohio Revised Code as “ impairment of ability to practiceaccording to acceptable and prevailing standards of care because of habitual or excessive use or abuse of drugs, alcohol, or othersubstances that impair ability to practice.”Source: State Medical Board of Ohio, 2019 Annual Reportof these claims, such as whether questionableprescribing was for personal use, are not publiclyavailable.Impact of patient care and safety onclinician wellbeingClinicians who provide direct patient care faceintense individual, organizational and socialpressures not to make mistakes. The mental healthand wellbeing of clinicians is at stake when they donot have adequate support from their employers tocope with adverse events, including medical errors,that arise in the healthcare setting. Two examplesof how this can manifest are described below.Second victim phenomenonPoor patient care and safety have emotionalconsequences for clinicians, which impacts theiroverall health. The term “second victim” describesa clinician who suffers emotionally when the carethey are involved in results in harm to the patient,or the clinician is involved in an adverse event.25Potential emotional consequences of second victiminclude anxiety, depression, decreased confidence,consideration of leaving their profession andsuicidal ideation.26 For example, a 2011 study of7,905 U.S. surgeons found the perception of havingmade a medical error was strongly associated withsuicidal ideation.27 Second victim can be both acause and a consequence of burnout.286Compassion fatigueThe day-to-day responsibilities involved with caringfor patients, especially those who are suffering, canbe highly emotional. “Compassion fatigue” is thesecondary traumatization a caregiver endures asa result of continuous exposure to emotional andinterpersonal stress involved with patient care.29 Itis a well-documented problem among clinicians,particularly in emergency and critical careenvironments, that contributes to poor clinicianwellbeing and often co-exists with burnout.30Further, compassion fatigue is associated withclinician retention problems.31Mediating factorsThere are also a number of mediating factors thatimpact clinician wellbeing and patient care andsafety highlighted in figure 1. These include: Laws, rules, regulations and the role ofpolicymakers, including legislators, state agenciesand health professional licensing boards. A state’spolicy landscape can determine whether acomprehensive approach to improving clinicianwellbeing can be achieved. Societal or cultural norms, including the role ofstigma, racism, discrimination and other biases.These factors impact systemic, institutional andindividual drivers of poor clinician wellbeing. Organizational culture, including leadership,values, policies and practices. A healthcareorganization’s culture is shaped by its leadershipand is influenced by both internal and externalfactors (policies and practices, laws andregulations, societal norms).
Clinical environment, including health informationtechnology, documentation and administrativeresponsibilities and workforce staffing practices.These factors impact a clinician’s workload andwork-life balance. Research and data, including collection,compilation and reporting of factors that impactclinician wellbeing. Policymakers, healthcareMediating factor examplesApproaches to improving clinician wellbeingmust consider the influence of mediating factors,both individually and in combination. Examples ofmediating factors that are often discussed in theresearch and that can be barriers to improvedclinician wellbeing are highlighted below.The role of stigma cuts across all factors thatimpact clinician wellbeing. Stigma amongclinicians, healthcare organizations, academicinstitutions and state policymakers impactsperceptions of clinician mental health andwellbeing. In doing so, stigma serves as a barrier toa comprehensive approach to improving clinicianmental health and wellbeing.For example, an important aspect of clinicianwellbeing is making sure clinicians can ask forand receive help for a mental health condition.Generally, clinicians are not educated orprepared to care for their own mental health,or to ask for help when they are struggling.33 Thestigma of clinician mental health conditions, whichbegins in the educational environment, may deterclinicians from asking for help or accessing care.Further, clinicians may choose not to seek helpor access treatment out of fear of personal orprofessional consequences.organizations and academic institutions needreliable data to accurately identify problems anddevelop effective solutions. Personal factors, including social support, familyissues and socioeconomic concerns. Eachclinician has unique experiences, circumstancesand responsibilities beyond their professional rolethat impact their overall wellbeing.32Longer shift lengths are associated with poorclinician wellbeing, burnout and poor patientoutcomes.34 Increased fatigue, errors, adverseevents/outcomes and burnout have beenassociated with shifts that exceed 8 hours.35Shifts longer than 12 hours have been shownto negatively affect nurses’ health and result inlower-quality patient care.36 Research has shown,however, that flexibility and choice in shift lengthcan contribute to a positive work environment.37While there is not consensus in the research on a“one size fits all” shift length that best supports bothclinician wellbeing and patient care and safety,considering all of these factors in the creation ofshift length policies can positively impact clinicianwellbeing.38Health information technology, including the useof electronic health records (EHRs), is associatedwith burnout among clinicians.39 A 2016 studypublished in Annals of Internal Medicine foundthat for every hour physicians have direct facetime with patients, almost two hours is spenton the EHR and administrative work.40 Further,clinicians may spend up to two hours of personaltime each night on documentation and clericalresponsibilities.41While research has shown use of EHRs takesaway time spent with patients and contributes toburnout, there are also documented benefits.42 Forexample, the use of health information technologyhas the potential to improve the quality and safetyof patient care.43 Taking all this into considerationis important in addressing clinician wellbeing andpatient care and safety.7
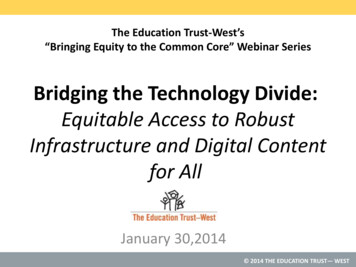
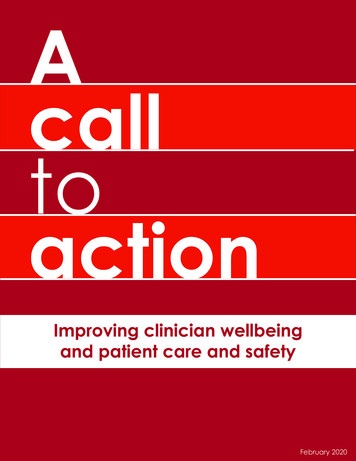
Figure 3. Consequences of burnout for cliniciansPhysical consequences Exhaustion Fatigue Inattentiveness Irritability Risk of motor vehicle accidentsPsychological consequences Stress Substance abuse Disruptive behavior Mood disorders Depression Suicidal ideationSource: Adapted from Patel, Rikinkumar S.,et.al. “Factors related to physician burnout and its consequences: A review.” BehavioralSciences 8, no. 11 (2018): 98.What is the scope of the problem?Clinicians are at a high risk for burnout and emotionalexhaustion, leading to depression, addiction andother mental health conditions that negatively impactwellbeing and increase risk for suicide. At the sametime, poor clinician wellbeing contributes to anincreased risk for medical errors and other adversepatient events. A 2016 analysis estimated medicalerrors as the third leading cause of death in the U.S.,resulting in over 250,000 deaths per year.44 While poorclinician wellbeing is not the only factor contributingto medical errors, its increasing prevalence poses asignificant threat to patient outcomes.Notably, clinician burnout is also associated withincreased clinician absenteeism, presenteeism (lostproductivity due to poor health) and turnover rates.45Modeling estimates indicate that each year in theU.S., burnout is attributed to 4.6 billion in costs relatedto physician turnover and reduced clinical hours.46Based on a survey distributed to more than 200hospitals, the 2019 NSI National Health Care Retentionand RN Staffing Report estimated costs associatedwith bedside nurse turnover ranged from 40,300 to 64,000 per nurse.47 Total costs associated with nurseturnover for an average hospital were estimated torange from 4.4 million to 6.9 million in 2018.48The following sections provide data and informationon the current state of clinician wellbeing with afocus on clinician burnout, mental health conditions,addiction and suicide. Much of the data andinformation on the prevalence of these issues amongclinicians is limited to single- and multi-institutionalstudies, many of which are not specific to clinicianspracticing in the U.S. Research was not included in thisbrief if it was (1) conducted or published outside ofthe U.S., or (2) published prior to the year 2000.BurnoutResearch indicates that burnout increases a clinician’srisk for depression, addiction and suicidal ideation.49Figure 3 highlights the potential physical and8psychological consequences of clinician burnout.According to the National Academy of Medicine’s(NAM) 2019 report, Taking Action Against ClinicianBurnout: A Systems Approach to Professional WellBeing, between 35% and 54% of U.S. nurses andphysicians experience symptoms of burnout.50 NAM’sreport also found burnout impacts clinicians earlyin their careers. For example, up to 60% of medicalstudents and residents experience burnout.51 Thesevere professional and personal consequences ofearly burnout can persist throughout a clinician’scareer and can negatively affect the quality of careprovided to patients.Mental healthA significant factor that increases risk of cliniciansuicide is untreated or inadequately treated mentalhealth conditions.52 The prevalence of mental healthconditions among clinicians, particularly depression,has been found to be alarmingly high over the pastdecade: Research indicates the rate of depression amongpharmacy residents is higher than the general U.S.population.53 A 2018 study found approximately 39%of pharmacy residents reported moderate to severedepressive symptoms.54 The same study showedthat, in March 2016, 7.3% of pharmacy residentsreported severe depressive symptoms, compared toan estimated 0.6% rate of severe depression in thegeneral U.S. population.55 A 2016 study found that almost 50% of femalephysicians believed they met the criteria for mentalillness and did not seek treatment.56 A 2015 systematic review and meta-analysisestimated the prevalence of depression ordepressive symptoms among resident physicianswas 28.8%.57 Similarly, a 2016 literature review found nursesexperience symptoms of depression at almosttwice the rate of individuals in other professions.58This same review found that young, female nurses,and nurses working in intensive care or psychiatricunits, reported higher rates of depression than nursesworking in other types of units.59
A 2013 study found the overall prevalence of anytype of depressive symptom among pharmacystudents was 52.4%.60 Even more concerning, thissame study indicated that pharmacy studentsmay be under-diagnosed with mental healthdisorders, such as depression and ObsessiveCompulsive Personality Disorder.61prevalence of alcohol abuse or dependence formale surgeons was 13.9%, and 25.6% for femalesurgeons.67 One study showed over 25% of pharmacystudents had indicators of harmful alcohol use.68Research also suggests that clinicians and healthprofessional students face unique risk factorsfor drug abuse, such as the high demands ofeducation and providing patient care, as well aseasy access to substances.69 Drug abuse may beginas self-treatment for stress and untreated mentalhealth issues.70 Notably, as compared to the generalpopulation, addiction among physicians tends tobe more advanced before it is even diagnosed asa problem.71AddictionResearch has found that alcohol misuseor dependence is associated with factorsthat negatively impact clinician wellbeing.62These factors include emotional exhaustion,depersonalization (cynicism), depression, suicidalideation, poor quality of life and low careersatisfaction. Substance use disorders and untreatedaddiction also contribute to high clinician suiciderates.63SuicideAs shown in figure 4, suicide is a “tip of the iceberg”indicator of the poor overall health and wellbeingof clinicians, signaling many challenges below thesurface.Notably, data regarding the prevalence ofaddiction and substance use disorders amongclinicians is limited, with several commonly citedresearch articles being more than two decadesold.64 However, several more recent studies highlightalcohol use as a significant problem for cliniciansand health professional students: A 2015 study found that 12.9% of male physiciansand more than one-fifth of female physicians(21.4%) met the criteria for alcohol abuse ordependence.65 Alcohol abuse and dependence was alsoidentified as a significant problem for surgeonsin the U.S.66 A 2010 survey of members of theAmerican College of Surgeons found theSuicide deaths were more common among nurses,pharmacists and physicians as compared to all U.S.workers of the same race and sex cohort, basedon an analysis of the Centers for Disease Controland Prevention’s National Occupational MortalitySurveillance (NOMS) data (see figure 5). Becausedeath from suicide is a downstream indicatorof other physical, mental or emotional healthproblems, this data serves as a call to action toaddress the root causes of poor clinician wellbeing.Figure 4. Suicide as a measure of clinician wellbeingClinician suicideMentalillnessEmotionalexhaustionPunitive workenvironmentStigmaDepressionAlcohol and illicitsubstance useBurnoutStressCompassion fatigueSecond victim phenomenonOrganizational culture thatdoes not support wellbeingLimited accessto treatment andrecovery supports9
Figure 5. Proportionate mortality ratio (PMR) for nurses, pharmacists and physicians forsuicide for adults ages 18-64, by race and sex, U.S., 1999, 2003-2004, 2007-2014*A PMR above 100 means that the cause of death (suicide) is more common among nurses,physicians or pharmacists of a specific race and sex compared to all workers of that cohortBlack femaleBlack male600White femaleWhite male600600600500500500400400300300Physicians(5 deaths)553500400394300400300Nurses(19 deaths)230193200Physicians(10 deaths)Nurses(39deaths)200212200Physicians(48 deaths)Nurses(882 deaths)Pharmacists(21 ts(92 deaths)Physicians(218 deaths)Nurses(283 deaths)* Data was collected from 26 states, including Ohio.Notes: PMR not calculated for black female and male pharmacists because there were fewer than five deaths due to suicide for these groups.PMRs cannot be used to compare outcomes across race and sex. For more information on the limitations of PMRs, see the CDCs NOMFAQ.Suicide is referred to as “intentional self harm” in this dataSource: The National Institute for Occupational Safety and Health, CDC10
What is a PMR?A proportionate mortality ratio (PMR) compares the proportion of deaths due to a specific cause withina population subgroup to the proportion of deaths due to that cause in the entire population.72 The PMRsdisplayed in figure 5 compare the proportion of deaths due to suicide among workers in three healthcarerelated occupations, disaggregated by race and sex, to the proportion of deaths due to suicide amongall workers of that race and sex.73 A PMR above 100 indicates the cause of death is more commonamong workers with a specific occupation, and a PMR below 100 indicates that the cause of death is lesscommon.Examples of how to interpret the data in figure 5:Worker populationOccupationPMRInterpretationBlack, male workersNurses230Black, male nurses are about 2.3 times as likely to die from suicide as black,male workers in general.White, female workersPhysicians212White, female physicians are more than twice as likely to die from suicide aswhite, female workers in general.PMRs cannot be used to compare outcomes
A 2016 literature review found that depression among registered nurses is linked to increases in presenteeism, and nurses who report presenteeism are more likely to report more medication errors, patient falls and overall poorer quality of patient care.19 A 2010 study from the Mayo Clinic, which surveyed over 7,900 American surgeons, showed