Transcription
NationalaccreditationstandardsStandardsWORKBOOKfor trauma recovery programmes– posttraumatic stress disorderDay programmesVersion 1.02015
Australian Government 2015This work is copyright. Apart from any use as permitted under the Copyright Act 1968, no part may be reproduced by any processwithout prior written permission from the Australian Government. Requests and enquiries concerning reproduction and rightsshould be addressed to the publications section of the Australian Government Department of Veterans’ Affairs (DVA) or emailed topublications@dva.gov.au.Published by DVA, Canberra, 2015.Technical editing and design by Biotext Pty Ltd Canberra MelbourneACKNOWLEDGEMENTSDVA thanks all those who contributed to the development and design of the Standards workbook, which supports the 2015 Nationalaccreditation standards for trauma recovery programmes – posttraumatic stress disorder, including: Professor Margaret Banks, Australian Commission on Safety and Quality in Health Care Phoenix Australia – Centre for Posttraumatic Mental Health, formerly known as the Australian Centre for Posttraumatic MentalHealth Biotext Pty Ltd representatives from private mental health hospitals and public hospital providers.
CONTENTSAbbreviations and glossary.ivIntroduction.1How to use the standards workbook . 1Programme evaluation. 2Use of data by services.6Standard 1Clinical governance.7Criterion 1.1Governance. 8criterion 1.2Clinical workforce. 9Criterion 1.3Clinical workforce support and supervision . 10Criterion 1.4Clinical workforce skills and expertise. 10Standard 2 Access and targeting.11Criterion 2.1Information provision. 11Criterion 2.2Programme criteria. 12Criterion 2.3Accessibility. 13Standard 3 Veterans’ rights and providers’ responsibilities .14Criterion 3.1Carers. 14Criterion 3.2Informed consent to participation. 15Criterion 3.3Veterans’ rights to programme services. 15Criterion 3.4Diversity. 16Standard 4 Clinical pathways.17Administrative system. 17Clinical system. 18Criterion 4.1Continuity of care. 19Criterion 4.2Intake and assessment. 20Criterion 4.3Review and discharge. 22Criterion 4.4Relapse prevention . 23Criterion 4.5Nine-month post-discharge follow-up . 23Attachment 4.1Clinical data collection consent form – Phoenix Australia copy. 24Attachment 4.2Clinical data collection consent form – veteran’s copy. 26Department of Veterans’ Affairsi
Attachment 4.3‘'Office use only’ box administrative requirements. 27Attachment 4.4Clinical assessment (CA-PTSD) . 28Attachment 4.5Clinician-administered PTSD scale (white cover; CAPS-5; CA-PTSD supplement) . 38Attachment 4.6Veteran intake questionnaire (blue cover; VI-PTSD) . 60Attachment 4.7Clinical discharge questionnaire at programme completion (yellow cover; CD-PTSD) .77Attachment 4.8Veteran discharge questionnaire at programme completion (green cover; VD-PTSD) . 82Attachment 4.93-month follow-up questionnaire (orange cover; V3-PTSD) . 98Attachment 4.109-month follow-up questionnaire (purple cover; V9-PTSD) . 114Standard 5 Treatment.130Criterion 5.1Treatment standards. 130Criterion 5.2Evidence-based treatment: individual therapy. 131Criterion 5.3Evidence-based treatment: group treatment. 132Standard 6 Clinical data collection.133Criterion 6.1Programme data collection and monitoring. 133Attachment 6.1Clinical data collection return form. 135Attachment 6.2Clinical data collection data audit form. 136References.137iiNational accreditation standards for trauma recovery programmes – posttraumatic stress disorder
TABLESTable I.1Selected measures – primary outcome measures. 3Table I.2Selected measures – secondary outcome measures. 5Table 1.1Criterion 1.1: Governance – how to achieve this criterion. 8Table 1.2Criterion 1.2: Clinical workforce – how to achieve this criterion. 9Table 1.3Criterion 1.3: Clinical workforce support and supervision – how to achievethis criterion. 10Table 1.4Criterion 1.4: Clinical workforce skills and expertise – how to achieve this criterion. 10Table 2.1Criterion 2.1: Information provision – how to achieve this criterion. 11Table 2.2Criterion 2.2: Programme criteria – how to achieve this criterion. 12Table 2.3Criterion 2.3: Accessibility – how to achieve this criterion. 13Table 3.1Criterion 3.1: Carers – how to achieve this criterion. 14Table 3.2Criterion 3.2: Informed consent to participation – how to achieve this criterion. 15Table 3.3Criterion 3.3: Veterans’ rights to programme services – how to achieve this criterion. 15Table 3.4Criterion 3.4: Diversity – how to achieve this criterion. 16Table 4.1Criterion 4.1: Continuity of care – how to achieve this criterion. 19Table 4.2Criterion 4.2: Intake and assessment – how to achieve this criterion. 21Table 4.3Criterion 4.3: Review and discharge – how to achieve this criterion. 22Table 4.4Criterion 4.4: Relapse prevention – how to achieve this criterion. 23Table 4.5Criterion 4.5: Nine-month post-discharge follow-up – how to achieve this criterion. 23Table 5.1Criterion 5.1: Treatment standards – how to achieve this criterion. 131Table 5.2Criterion 5.2: Evidence-based treatment: individual therapy – how to achieve thiscriterion. 131Table 5.3Criterion 5.3: Evidence-based treatment: group treatment – how to achievethis criterion. 132Table 6.1Criterion 6.1: Programme data collection and monitoring – how to achievethis criterion. 134Department of Veterans’ Affairsiii
ABBREVIATIONS AND GLOSSARYADFAustralian Defence ForceCAPSclinician-administered PTSD scaleCA-PTSDclinical assessment – posttraumatic stress disorder questionnairecarerIncludes partners or significant others who provide support to veteransCD-PTSDclinical discharge – posttraumatic stress disorder questionnaireCDCclinical data collectionDVAAustralian Government Department of Veterans’ AffairsEMDReye movement and desensitisation reprocessingIDidentificationNSMHSNational Standards for Mental Health Services (2010)participantrefers to serving members of the ADF or first responders who participate in a TRPPhoenix AustraliaPhoenix Australia – Centre for Posttraumatic Mental HealthPTSDposttraumatic stress disorderTF-CBTtrauma-focused cognitive behavioural therapyTRPtrauma recovery programmeV3-PTSDveteran 3-month follow-up – posttraumatic stress disorder questionnaireV9-PTSDveteran 9-month follow-up – posttraumatic stress disorder questionnaireVD-PTSDveteran discharge – posttraumatic stress disorder questionnaireVI-PTSDveteran intake – posttraumatic stress disorder questionnaireveterangeneric term for veterans and/or former serving members of the ADF eligible for DVA treatment servicesVVCSVeterans and Veterans Families Counselling ServiceivNational accreditation standards for trauma recovery programmes – posttraumatic stress disorder
INTRODUCTIONThe Department of Veterans’ Affairs (DVA) contracts privateand public hospitals throughout Australia to provideevidence-based trauma recovery day programmes (TRPs)for veterans who have posttraumatic stress disorder (PTSD).Current serving members of the Australian Defence Force(ADF) and first responders (e.g. police emergency services)may also access the programmes, if funding is provided bytheir employer.These programmes are not intended to be stand-aloneservices, nor will they meet all the treatment needs ofveterans with PTSD and related problems. They are partof the continuum of care for veterans funded by DVA,which often includes general practitioners, Veterans andVeterans Families Counselling Service (VVCS), communitybased psychiatrists, psychologists, other mental health andrehabilitation (clinical and vocational) practitioners, andhospital-based acute assessment and inpatient services.TRPs provide highly specialised, time-limited, evidence-basedtreatment for PTSD and its common comorbidities.HOW TO USE THE STANDARDSWORKBOOKProviders can use this workbook with the TRP standards(Australian Government 2015) to prepare their programmesfor TRP accreditation. The workbook will help themdetermine if they have sufficient evidence to demonstratethat their systems and processes meet the accreditationrequirements. The workbook can also be used to determine ifthe evidence available to meet the relevant TRP standard alsofulfils the requirements for the matched National Standardsfor Mental Health Services (NSMHS) criteria (AustralianGovernment 2010).In many cases, the examples of evidence required to meetcriteria for each set of standards are similar (e.g. accreditorswill be looking for policies, procedures and protocols forsome items, file audits and working documents for others,and results of consumer and carer feedback). The workbookdoes not, however, cover all possible sources of evidence;the ones suggested are examples only. Providers are freeto use any evidence to satisfy the criteria. The evidencewill typically come from the usual business improvementstrategies already in place, rather than from additionalstrategies developed specifically for accreditation.Not every NSMHS standard is relevant to targeted grouptreatment such as the TRP – PTSD; only some NSMHSstandards can be linked directly to the TRP standards. It isassumed that many of the more generic NSMHS standardswill be addressed through the accreditation of the broaderhospital service in which each TRP sits. Services need tobe aware that satisfying the accreditation criteria forthe TRP will not qualify them for their hospital’s overallaccreditation.RESOURCESTRP services are strongly advised to consider the informationprovided on DVA’s ‘health professional’ section of the At Easewebsite (https://at-ease.dva.gov.au/professionals).The website provides up-to-date information on training,mental health resources and mobile phone applications thatwill provide assistance and support when working with theveteran community.Department of Veterans’ Affairs1
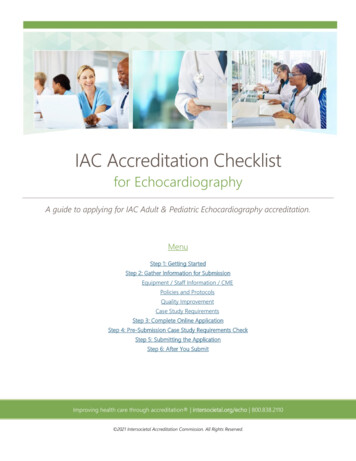
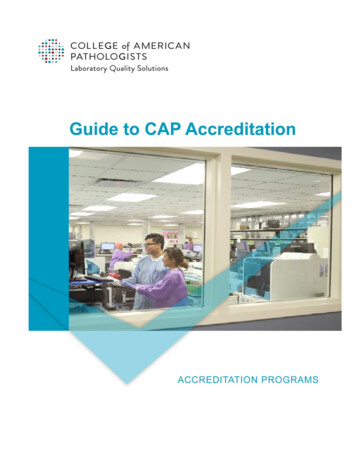
PROGRAMME EVALUATIONDVA will evaluate the clinical effectiveness of a TRP bycollecting outcome data from veterans through PhoenixAustralia – Centre for Posttraumatic Mental Health, undercontract arrangements.TRP clinical data collection (CDC) has two main aims: to describe the population characteristics of veteransentering the programmes to measure change across time of an individual’s clinical,social and functional profile that the programme istargeting.Data are collected through: a clinician-administered assessment interview before thegroup programme starts a brief clinician-completed questionnaire at end ofgroup treatment a veteran self-report questionnaire at four time points-- before the group treatment starts-- after the group treatment ends-- 3 months after discharge-- 9 months after discharge.DVA’s Human Research Ethics Committee has approved themonitoring of TRP outcomes (E096/002 – Evaluation of PTSDTreatment Offered by Programmes). The ethics approvalhas been granted to collect data from veterans and formerserving members.ACCESSING ELECTRONIC COPIES OFQUESTIONNAIRESEach service has access to electronic copies of theassessment questionnaires through the Phoenix Australiawebsite. The user name and password for accessing thematerials are provided via email by Phoenix Australia (seestandard 4). It is the service’s responsibility to print thesequestionnaires and ensure that the cover page for eachquestionnaire is printed on the correctly coloured paper.WHAT IS THE CLINICAL DATA USED FOR?Clinical outcomes from the TRPs are referred to as ‘primaryoutcomes’, and social and functional outcomes are referredto as ‘secondary outcomes’. How each construct is measuredand the rationale for the measure used are shown in Tables I.1(primary outcomes) and I.2 (secondary outcomes).Primary outcomes PTSD. The TRP is primarily a PTSD treatment programme,with measures of PTSD identified as the primary outcomemeasure. PTSD will be measured by both structuredclinical interview and a self-report questionnaire. Thestructured clinical interview will be used to ensure thatthose entering the programme have a clinical diagnosisof PTSD, which is a DVA requirement of entry into theprogramme. Where a veteran falls short of the fulldiagnostic criteria and the clinician believes they willbenefit from the programme (based on their PTSD-relatedsymptoms, level of distress and/or impairment), they canbe considered for inclusion. Complex PTSD symptoms. Complexities often seen inthe trauma presentations of veterans will be measured.These include emotional dysregulation, relationshipdysfunction and negative self-concept. Anxiety. Anxiety symptoms are often comorbid with PTSD. Depression. Similar to symptoms of anxiety, depressionsymptoms are often comorbid with PTSD. General distress. This is a general mental health measurethat has community norms and allows for comparisonwith means of other populations of interest – forexample, veterans attending the TRP. Substance use. Alcohol and nicotine are the two keymeasured outcomes for substance use. Data on use ofillicit substances are often unreliable and often unusablein an environment such as the PTSD group programmes;therefore, questions around illicit substance use are notconsidered appropriate. Anger and aggression. Anger is a key target for theprogramme. In addition to anger, aggression (behaviourthat is hostile or attacking) will be measured, because it isa key issue of concern. Sleep. Sleep is increasingly identified as a sensitivemarker of mental health status.The measures are selected based on their consistency withthose in the Diagnostic and statistical manual of mentaldisorders (DSM-5; APA 2013), for their psychometric strengthand their brevity.From the data, several key indicators of change (‘constructs’)can be measured. These indicators have been selected basedon the previous PTSD group programme protocols, andinclude some changes because of updates to questionnairesor addition of constructs.2National accreditation standards for trauma recovery programmes – posttraumatic stress disorder
Table I.1Selected measures – primary outcome measuresConstructMeasureDescriptionValidity and reliability ScoringPTSDPosttraumaticStress Checklist(PCL-5; (Weatherset al 2013)PCL-5 provides patients with a list of the20 symptoms of PTSD (as defined by DSM5). Patients are asked how much they havebeen bothered by each symptom in the pastmonth. Patients are instructed to answerthese questions, keeping their worst eventin mind.Information aboutthe reliability of PCL-5is not yet available.The PCL for DSM-IVhas excellent test–retest reliability over2–3 days. Internalconsistency is veryhigh for each of thethree groups of itemscorresponding to theDSM-IV symptomclusters, as well as forthe full17-item scale(Blanchard et al 1996).Each item is scoredon a 5-point Likertscale from 1 (‘not atall’) to 5 (‘extremely’).Total possible scoresrange from 20 to100. Cut-off scoreswill be released bythe authors shortly.ComplexPTSDsymptomsComplex PTSDScale (Cloitre,Roberts, Bisson,Brenin 2015)This new, complex PTSD scale has beendeveloped by the team who are proposingComplex PTSD for ICD-11. It comprises threeclusters of symptoms, including emotionaldysregulation, negative self-concept andinterpersonal difficulties. It also includesquestions around functional impairment.Information aboutthe reliability of theComplex PTSD Scale isnot yet available.Each item is scoredon a 5-point Likertscale from 0 (‘notat all true’) to 4(‘extremely true’).AnxietyHospital Anxietyand DepressionScale (HADS)(Zigmond andSnaith 1983)HADS was developed to assess anxietyand depression among patients in nonpsychiatric hospital settings. It is divided intotwo subscales (anxiety and depression), eachconsisting of 7 questionsHADS is a particularly useful tool forpopulations with a high prevalence ofphysical injury or illness (e.g. veterans),because it excludes the somatic symptomsthat also and often relate to physicaldisorders. For example, sleep problems andfatigue are common physical symptoms inveterans, and scoring positively on thesewould not necessarily reflect that theveteran is positive for the somatic symptomsof anxiety and depression.HADS has shownexcellent discriminantvalidity and internalconsistency, as wellas a stable factorstructure (Bjelland et al2002).Each item is rated ona 4-point Likert scalefrom 0 to 3, withtotal scores for eachsubscale rangingfrom 0 to 21. Higherscores indicate higherlevels of distress. Acut-off of 10 or 11is used to identifyrespondents with ahigh probability ofsuffering from ananxiety or depressivedisorder.DepressionHospital Anxietyand DepressionScale (HADS)As aboveAs aboveAs aboveGeneraldistressKesslerPsychologicalDistress Scale(K10) (Kessler etal 2002)K10 was developed to screen populationsfor non-specific psychological distress. Itwas used in the National Mental Health andWellbeing Survey, permitting comparisonsof veterans’ scores with the nationalaverage. The questions focus on anxiety anddepression, and respondents are instructedto answer all questions about how they havebeen feeling during the past 30 days.K10 shows strongconvergent validitywith cliniciandiagnosed anxiety andmood disorders, and issignificantly associatedwith the presence ofany mental healthdisorder (Andrews andSlade 2001).Responses are scoredon a 5-point Likertscale from 1 (‘noneof the time’) to 5 (‘allof the time’), withtotal scores rangingfrom 10 to 50. Higherscores indicate higherlevels of psychologicaldistress.Department of Veterans’ Affairs3
ConstructMeasureDescriptionValidity and reliability ScoringAlcohol useAlcohol UseDisordersIdentification Test(AUDIT) (Babor etal 1989)AUDIT is a WHO-recognised brief screeningtool that identifies currently active,hazardous and harmful drinkers. TheAUDIT questionnaire consists of 10 itemsthat measure alcohol consumptionand dependence symptoms, as wellas the personal and social harm thatreflects drinking. All items in the AUDITquestionnaire refer directly to drinking andits effects. It is suitable for both men andwomen (Aertgeerts et al 2001).The AUDIT shows goodreliability and validityacross a number ofpopulations.Each item is scored ona 4-point Likert scale,with total AUDITscores ranging from 0to 40. A cut-off of 8 isgenerally accepted asidentifying individualswith a potentialalcohol problem(Reinert and Allen2002).Tobacco useQuestions fromthe ADF Healthand WellbeingSurveyFour-item questionnaireNot applicableNot applicableAngerDimensionsof AngerReactions-5(DAR-5) (Forbeset al 2014)DAR-5 was developed after research revealedthat two items could be removed from theoriginal 7-item scale without compromisingpsychometric strength. Four items addressanger responses, and one addresses theimpact of anger on social relationships.Respondents are asked to consider theamount of time they have felt each of theresponses or relationship impairment in thepast 4 weeks.DAR-7 has been shown to be predictive ofchange in not only veterans’ anger levels, butalso PTSD symptoms, alcohol use and familyfunctioning after PTSD treatment (Evans et al2003, Forbes et al 2003, Forbes et al 2008).Internal consistencyis high, and the scaledemonstrates goodconvergent validitywith other measures ofanger and PTSD, anddiscriminant validitywith measures ofdepression (Forbes etal 2014).Each item is scoredon a 5-point Likertscale from 1 (‘noneor almost none ofthe time’) to 5 (‘allor almost all of thetime’), with totalscores ranging from5 to 25. A cut-off of12 is recommendedfor identifying thosewith high anger levels(Forbes et al 2014).AggressionWar StressA 12-item excerpt that assesses frequency ofInventoryanger-related behaviours(aggressionexcerpt) ( Johnsonet al 1996).Used as an excerpt inprevious DVA PTSDprogramme monitoringwith this populationA combination of‘yes/no’ responsesand free entry toindicate number ofdaysSleepInsomnia Severity The 7-item ISI assesses difficulty falling andIndex (ISI) (Morin staying asleep, and problems waking up1993)too early.ISI is a reliable andvalid instrument thatcan be used to quantifyperceived insomniaseverity and detectchanges (Bastient et al2001).Responses are scoredon a 5-point Likertscale from 0 to 4.ADF Australian Defence Force; DSM-IV Diagnostic and statistical manual of mental disorders, 4th edition; DSM-5 Diagnostic and statistical manual of mentaldisorders, 5th edition; DVA Australian Government Department of Veterans’ Affairs; ICD-11 International classification of diseases, 11th revision; PTSD posttraumaticstress disorder; WHO World Health Organization4National accreditation standards for trauma recovery programmes – posttraumatic stress disorder
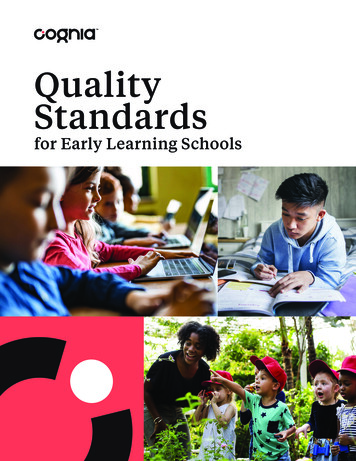
Secondary outcomesThe data collected as part of secondary outcomes includedemographic and other descriptive information, such asgender, current employment status, military service historyand health service usage. Quality of life. This refers to how a health condition ordisability may impact on broader aspects of wellbeing,Table I.2such as an individual’s perception of their position in lifein relation to goals, expectations, standards and concerns. Relationship functioning. This will be completed byveterans who have a current partner. Physical health. Somatic physical health symptoms oftenhave a psychological basis, which may improve followingpsychological intervention.Selected measures – secondary outcome measuresConstructMeasureDescriptionValidity and reliabilityScoringQuality of lifeAssessment of Qualityof Life instrument –4 Dimensions version(AQoL-4D) (Hawthorneet al 1999)AQoL-4D is a 12-item scaleassessing 4 dimensions ofhealth-related quality of life:independent living, mentalhealth, relationships andsenses. Each item requiresrespondents to evaluatetheir health status during thepast week. The scale takesapproximately 1–2 minutesto complete.The AQoL was chosen asa quality-of-life measurebecause it allows comparisonof participants in thetreatment programme andnational health economicdata.AQol-4D shows excellenttest–retest reliability( 0.80) (Richardson et al2011) and good convergentvalidity with self-reportedhealth status (Hawthorneand Osborne 2005). Thereis some evidence that theAQoL has greater sensitivityto health states than similarmeasures (Hawthorne et al2001).Each item is scoredon a 4-point scale,with higher scoresindicating poorerquality of life. Aweighted scoringalgorithm is used todetermine overallquality of life, on ascale from 0.04 (‘worsethan death’) to 1.00(full QoL) (Hawthorneand Osborne 2005).Two items fromWHOQOL-BREF(WHOQOL Group 1996)WHOQOL-BREF has 26 itemsand measures psychologicalhealth, physical health,social relationships andenvironment.RelationshipfunctioningAbbreviated DyadicAdjustment Scale(ADAS) (Sharpley andRogers 1984)ADAS comprises 7 items.ADAS demonstrates goodconstruct and convergentvalidity with objectivemeasures of maritalsatisfaction (i.e. separated,divorced, married, defacto) and with otherrelationship measures(Hunsley et al 2001,Sharpley and Rogers 1984).It also displays acceptableinternal consistency ( 0.75)(Hunsley et al 2001,Sharpley and Rogers 1984).Total scores range from0 to 36, with higherscores indicatinggreater relationshipsatisfaction.Physical healthQuestions from the ADFHealth and WellbeingSurveyA 15-item questionnaireNot applicableItems are scored ona 3-point scale from‘not bothered at all’ to‘bothered a lot’.ADF Australian Defence ForceDepartment of Veterans’ Affairs5
USE OF DATABY SERVICESEach service can use its CDC information for qualityassurance and clinical purposes only (via a request toPhoenix Australia for a statistical file of the scored data).Note that Phoenix Australia only holds de-identified veteraninformation.Data cannot be used by services for research or publicationpurposes.Services requiring access to the database for purposes otherthan listed above should contact DVA's hospital contractmanager in their state or territory.6National accreditation standards for trauma recovery programmes – posttraumatic stress disorder
STANDARD 1CLINICALGOVERNANCEThe TRP service complies with the governance frameworkthat supports a skilled clinical workforce in the delivery ofevidenced-based treatment.What will this standard deliver? TRPs that are reliable. TRPs that are monitored, reviewed and improved. A clinical workforce that has relevant clinical skillsand qualifications, and is supervised, trained andsupported. A clinical workforce that is maintaining and/orimproving its skill set.Department of Veterans’ Affairs7
CRITERION 1.1GOVERNANCEQUESTIONS TO ASK Do we have a regular strategic planning meeting? Is the strategic plan linked to the services’ qualityimprovement process? How do we match what we can do, what we plan to doand the agreed areas of clinical practice for the workforcewith the services and care we provide? How do we plan our work and then measure ourperformance to make improvements? How do we involve veterans and stakeholders in ourstrategic planning? What action have we taken to reduce safety risks andimprove the quality of care for our veterans? Do we have a well-documented and consistentlyimpl
CA-PTSD clinical assessment - posttraumatic stress disorder questionnaire carer Includes partners or significant others who provide support to veterans CD-PTSD clinical discharge - posttraumatic stress disorder questionnaire CDC clinical data collection DVA Australian Government Department of Veterans' Affairs