Transcription
ErrorsinRadiationOncologyGeoffrey S. Ibbott, Ph.D.with slides fromJake van Dyk
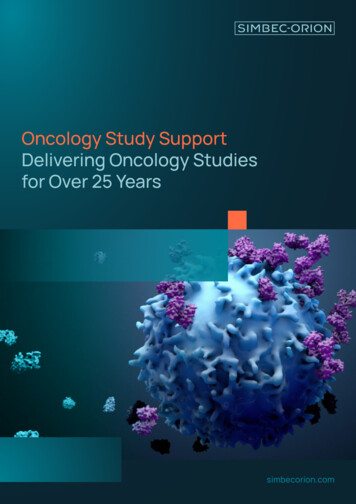
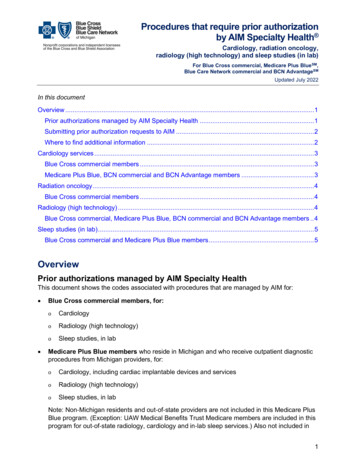
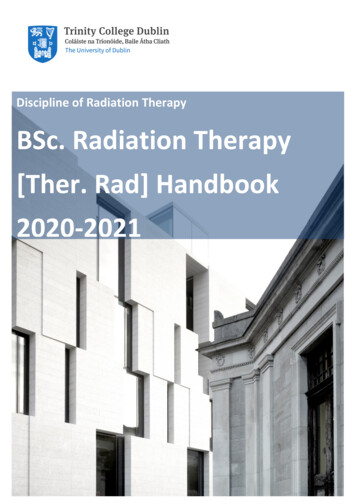
ICRU Goal in Dose Calculationand Spatial Accuracy110Real Data1990s1002%9080Realative DoseICRU 42, 1987Recommends Relative doseaccuracy inuniform doseregion: 2% Spatialaccuracy inhigh dosegradient: 2 mm Off Axis profile704 mm6050403020Measured10Computed00123456789 10 11 12 13 14 15 16 17 18 19 20Off axis distance (cm)222006-11-28RSNA
Errors in Radiation Oncology Error “The failure of planned action to be completed asintended (i.e., error of execution) or the use of awrong plan to achieve an aim (i.e., error ofplanning).”Institute of Medicine. To Err is Human: Building a Safer Health System, 2000.332006-11-28RSNA
Euphemisms for “Errors”Accidents Incidents Misadministrations Unusual occurrences Discrepancies Adverse events 442006-11-28RSNA
Medical Errors - General In United States Annual errors 5 44K-98K people die from medical errors More than motor vehicle accidents, breast cancer or AIDS Total annual cost 37.6 to 50 billionMost common types52006-11-28RSNA Technical (44%) Diagnosis (17%) Failure to prevent injury (12%) Use of drugs (10%)Institute of Medicine. To Err is Human: Building a Safer Health System, 2000.
Medical Error AnalysisRecently, more public & acceptable practice Sample references - medicine in general Sample references - RT 6Institute of Medicine. To Err is Human: Building a Safer HealthSystem, 2000.Sokol & Molzen. The Changing Standard of Care in Medicine, JLegal Med, 2002.Baker et al. The Canadian Adverse Events Study: the incidence ofadverse events among hospital patients in Canada. CMAJ 2004.62006-11-28RSNAMacklis et al. Error Rates in Clinical Radiotherapy. J Clin Oncol,1998.Cosset. ESTRO Breur Gold Medal Award Lecture 2001. IrradiationAccidents - Lessons for Oncology? Radioth Oncol, 2002
Reports of Errors in RTIAEA 2000772006-11-28RSNAICRP 2000IAEA 2001
Radiation Accidents The IAEA has tabulated 92 accidentalexposure events Radiation measurement systemsMachine commissioning & calibrationTreatment planningPatient setup and treatmentDecommissioning of teletherapy equipmentMechanical and electrical malfunctionBrachytherapy/LDR sources andapplicatorsBrachytherapy/HDRUnsealed sources
Radiation MeasurementSystems Incorrect use of calibration report Report specified ND,w but was interpreted as NkCorrection for atmospheric pressure (Bend, OR) Institution had no in-house barometer Physicist used airport or transported aneroidbarometer Airport reported pressure corrected to sealevel (elevation was actually 3,500 ft.) Aneroid barometer made one completerevolution (4”) and appeared to indicate sealevel pressure Patients received 13% overdose
Error in MachineCalibration Cobalt unit calibration errors Physicist decayed 60Co activity usinggraph paper (Riverside Hospital)Asymmetric jaws calibrated with chamber oncentral axis, in penumbraTreatment in “Physics” mode At source replacement, used 30 sec rather than 0.3min (166% overestimation of exposure time)Target, flattening filter and monitor chambernot deployed in one beam energyCalibration at 10 cm depthinterpreted as dmax 50% overdose
Machine Operation “Malfunction 54” If operator selected 25 MV x rays then switchedquickly to electrons, machine delivered 25 MVelectrons with high beam current, no target andno flattening filter. Monitor chamber switched beam off promptly,but patient had received 160-180 Gy. Malfunction occurred at four hospitals beforeproblem recognized and acknowledged bymanufacturerZaragosa, Spain Serviceman didn’t recognize bending magnetfailure Accelerator automatically delivered maximumbeam energy Beam steering failed, high recombinationlosses led to low monitor response and highpatient doses
Treatment PlanningSystem Inconsistent sets of basic machinedata Calculations with one set resulted in10% underdoseWedge factor incorporated by TPS,also by operator calculating MUsettingIncorrect application of 1/r2 forisocentric treatments when alreadyapplied by TPSError by TPS when blocks enteredclockwise vs counter-clockwise(Panama)
IAEA
Treatment Planning Fix “Shortcut” method of block entrybecause 4 blocks
Treatment Planning Fix “Shortcut” method of block entry evenwhen 4 blocksNote: Two approaches
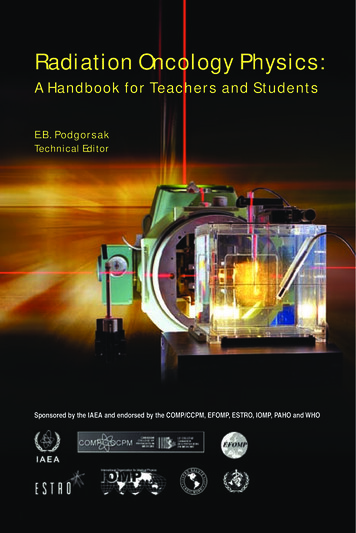
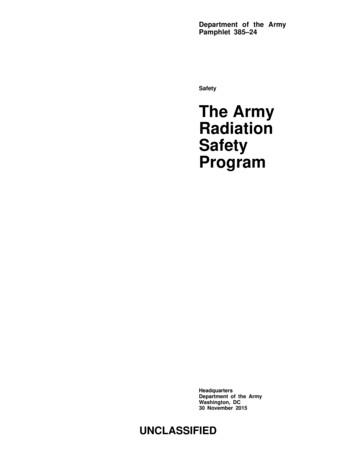
Identification ofProblem90%70%Open beam50%30%Blocksenteredtogether withtwo CWcontours
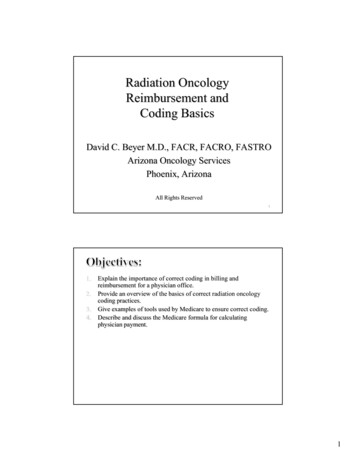
RTPS Calculated CentralAxis DataOpenBlockedDifferenceslead tooverdosingby 2
Clinical Summary - March2002 28 patients treated with incorrectdoses 17 have since died13 had rectal complications
Factors Contributing toErrors Inadequate instructions in the RTPSmanualInsufficient QA in treatmentplanning process No manual checksNo written procedure of changes whenentering the blocksWork organizationExcessive workloadLack of coordination between membersof radiation therapy team
PhysicistsJailedNovember 2004Two of the indicted physicists are condemned to four years in prison andbarred to practice their profession for seven years. They appeal the sentence.The third physicist is acquitted.
Errors in RT: ContributingFactors Insufficient educationLack of procedures/protocols as partof comprehensive QA programLack of supervision of compliancewith QA programLack of training for “unusual”situationsLack of a “safety culture”
Errors Related to ModernTechnology IMRT Example error Errorin transferring plan data tomachine Transferred open field data but notleaf sequence Full dose given with open field RPC phantom data Later Gamma Knife Wrong side of brain treated –coordinates were reversed
Complexity of ModernRTPS Many issues to address HardwareSoftware Networking Use of images, 3-D, IMRT, optimization, planevaluationDosimetry devicesImaging devicesTreatment machinesOncology information systemPhysicians’/physicists’ offices/homesSome capabilities not easy to test
LDR Brachytherapy TPS required entry in R cm2 h-1 rather than µGym2 h-1.TPS required entry in mg-Ra-eq rather than mCi125I sources ordered with wrong activity (4 mCivs 0.4 mCi)Calculations based on wrong nuclide137Cs source strengths incorrect137Cs source with no activity mixed in withinventoryLost sourcesPatient left hospital with sources in placeSources not removed properly or at terminationof treatment
HDR Brachytherapy Indiana, PA Source would not enter one of 5 catheters (hadalready broken off inside another catheter) Staff discontinued treatment, ignored arearadiation monitor alarm, misinterpreted consoleindications Patient with source still in catheter,transported to nursing home After 4 days, catheter fell out, placed intrash Trash disposal company detected radiation Patient received dose resulting in death, 94other staff received radiation exposures.
Lessons Learned Resources: Adequate, trained personnelIdentification of safety criticalactivities: Commissioning, validation Periodic calibration, QC Proper decommissioning of sources Identification of patient Prescription understood, communicatedaccurately Treatment procedures understood andmodifications communicated accurately Planning system, procedures and dataconfirmed, verified, and documented Sources calibrated, identified andinventory checked
Prevention andMitigation Clear job descriptions, assignment ofresponsibilities and lines of authorityAnticipation of unplanned or unusual situationsAppropriate actions: Change in supplier Change in routine dose or treatment procedure Introduction of new or unusual procedureAccurate communicationEquipment maintenance, proper operationDocumentationIntegration of safety and quality assurance
Institute of Medicine. To Err is Human: Building a Safer Health System, 2000. 4 2006-11-28 RSNA 4 Euphemisms for "Errors" .