Transcription
UNFINISHED BUSINESS:Implementation of the National SuicidePrevention Adviser’s Final AdviceFirst year progress reportApril 2022
ForewordIf you add up all the suicide prevention and mental healthinquiries over the past three years you quickly get to 21.That’s more than one every two months, the equivalentof an inquiry every 52 days.Across endless consultations people with livedexperience have bravely shared their insights,researchers have crunched many numbers andour members have been beyond generous in theirconsultation advice. We have the roadmap, and we needto keep following it.Most significant among these reviews was theFinal Advice of the Prime Minister’s National SuicidePrevention Adviser. As a sector, we worked hard to helpguide this work and were proud to see its release12 months ago.Whoever forms government after this federal electionwill take the reins of power at a critical time for suicideprevention. We know the risk of suicide rates are oftenhighest two to three years after a crisis, pandemicor natural disaster. We know there’s record levels ofdistress across our community.This report makes clear to all parties that sustained andsystemic change is required. There is progress beingmade, but there’s ‘unfinished business’ when it comes tosuicide prevention and the national reform agenda.We need to finish what we’ve started.Implementation matters and it’s time to get on with it.All recommendations from the Final Advice mustbe implemented.Thanks to the Final Advice, and other valuable work,we know what needs to be done. We know the shiftsand enablers required to turn the trend towards zerosuicides. It’s time now for action. Sustained andongoing action.As you will see in this report, there’s been some positiveprogress in the last year. Few of these recommendationscan be achieved in one year, they are long-term shiftsand several are underway.Many have worked hard to kick-off these very important,systemic and long-term reforms. Yet, there’s much moreto be done in the months and years to come. We can’ttake our foot off the pedal and now is the time todouble-down on early progress.2Nieves MurrayCEOSuicide Prevention Australiawww.suicidepreventionaust.org
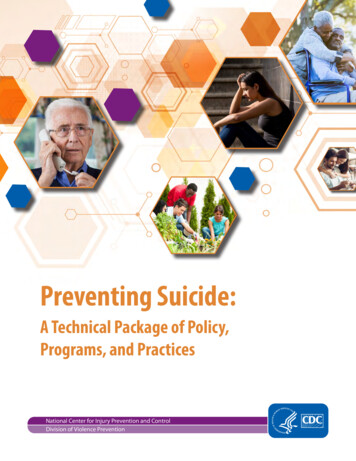
BackgroundTwelve months ago the Final Advice of the PrimeMinister’s National Suicide Prevention Adviser,Ms Christine Morgan, was released. The Final Adviceoutlines major and lasting reforms that are neededto deliver a connected and compassionate suicideprevention system.The Final Advice was the culmination of 18 months ofengagement across government, the suicide preventionsector, researchers and communities. Over 3,000people with lived and living experience of suicide sharedtheir insight and knowledge to inform this report. Itsfindings were strongly supported across the sectorand community.To drive change, it identified four key enablers: a wholeof government approach, lived experience knowledgeand insight, data and evidence to drive outcomes, andworkforce and community capability.Four further priority shifts were also recommended:responding earlier to distress, connecting people tocompassionate services and supports, targeting groupsthat are disproportionately affected by suicide anddelivering policy responses that improve securityand safety.About this reportThis report is intended to help track progress indelivering on recommendations of the Prime Minister’sNational Suicide Prevention Adviser’s Final Advice.Its first edition is released on the one-year anniversaryof the Final Advice and future reports will bereleased annually.There’s no doubt this reform agenda is systemicand long-term, it will take time and sustained actionto achieve. This requires bipartisan support andcommitment above and beyond politics.The Final Advice made recommendations acrossfour key enablers and four key shifts. Each includes anumber of priority actions to drive a more connected andcompassionate approach to suicide prevention.These include a number of significant reforms and itwould not be reasonable to expect their full deliveryovernight or within the first 12 months. The varied statusof many recommendations is not intended as a criticismof material work to date, but rather to transparentlydemonstrate that while progress is being made, muchmore is still needed and that systemic change requiressustained funding and reform commitments.www.suicidepreventionaust.orgThe report tracks progress on each of the Final Advicepriorities and rates progress over the past twelve monthsas one of the following:Major progressModerate progressNil/minimal progressIn the context of a federal election and as the FinalAdvice was commissioned by and accepted on behalf ofthe Australian Government, this report tracks progressat the Commonwealth level. This does not discountthe critical role State and Territory jurisdictions play insuicide prevention, including across a number of theserecommendations. The progress of State and TerritoryGovernments will be the subject of a separate reportlater in 2022.3
Final AdviceLeadership andgovernanceto drive a whole-of-governmentapproachknowledge & leadershipDataand evidenceWorkforceand communityRespondConnecting peopleto drive outcomesearlier to distressTargeting groupsthat are disproportionatelyimpacted by suicide4Lived experiencecapabilityto compassionate servicesand supportsPolicy responseto improve securityand safetywww.suicidepreventionaust.org
Leadership and governance todrive a whole-of-governmentapproachFinal Advice Recommendation: All governments work together to deliver a whole-of-government approach – atthe national (cross-jurisdictional), jurisdictional (cross-portfolio) and regional levels; with national outcomes to bedeveloped and adopted by all governments.Priority Actions1.1 A ll governments to continue or shift toa whole of government approach, withsuicide prevention authorised by FirstMinisters and mechanisms to drivecross-portfolio action implemented.StatusProgress of AustralianGovernment Response (Year One) The National Suicide Prevention Office (NSPO) has beenestablished with a whole-of-government focus. The NSPOsits within the National Mental Health Commission (NMHC)and Health portfolio. The Final Advice states that thiswas preferred by some jurisdictions, but consultationsindicated that it should operate as a separate authoritywith enabling legislation The Assistant Minister for Suicide Prevention reports to thePrime Minister and is supported by both the Departmentof Health and Department of Prime Minister and Cabinet The National Agreement commits to a whole-ofgovernment approach including commitments to considersuicide prevention in a range of human services areas1.2 A National Suicide Prevention Strategyis developed to align with the NationalAgreement on Mental Health andSuicide Prevention, identifyinginitiatives which require a strategicnational approach. A public commitment to a National Strategy hasbeen identified as a priority but the strategy is yet tobe developed1.3 A National Suicide Prevention Officeis established in 2021 to set strategicdirections, build capabilities, supportcross-jurisdictional and cross-portfolioaction and report on agreed outcomes. The NSPO was established in late 2021 and its advertisedremit includes strategic directions, capability building,cross-jurisdictional and cross-portfolio action The National Agreement does not reference a NationalSuicide Prevention Strategy It is not clear whether reporting on agreed outcomes willbe included in the NSPO list of responsibilities The National Agreement was announced in March 2022 andhas been signed by a majority of jurisdictions The Agreement commits to more integration andthe development of national guidelines on regionalcommissioning and planning within the first twelve months1.4 T he National Agreement on MentalHealth and Suicide Prevention to includestrengthened and resourced regionalarrangements for suicide prevention. T he National Mental Health and Suicide PreventionAgreement (National Agreement) recognises that a whole-ofgovernment approach is required, and that many enablersof suicide prevention reform are beyond the influence of thehealth system alone and span all aspects of where peoplelive, work, learn and socialise. It commits Parties to a rangeof actions directed towards suicide prevention The 2022 Budget commits 30.2 million to deploy regionaland community-based suicide prevention systems and 10.4 million for a Suicide Prevention Regional ResponseLeader to coordinate suicide prevention activities in allPrimary Health Networkswww.suicidepreventionaust.org5
The establishment of a NSPO and a new NationalAgreement put in place the foundations for a whole-ofgovernment approach. With half of those who die bysuicide each year not accessing mental health servicesat the time, we’ll only turn the trend towards zerosuicides if we embed this approach across governmentand the community.The current location of NSPO within the Health portfolioand National Mental Health Commission will limit itsability to drive this much-needed change.6Central agency coordination and First Minister leadershipwill be critical to driving human service, education andeconomic portfolios to consider suicide in their work.At a high level, the new National Agreement sets theright direction for reform but it’s the actions that situnder it and implementation that will matter. The newNational Suicide Prevention Strategy must take thenext step towards reform with concrete actions, clearaccountability and real change.www.suicidepreventionaust.org
Lived experience knowledgeand leadershipFinal Advice Recommendation: Recognising that measurement of outcomes is essential to monitor impacts ofsuicide prevention initiatives, all governments commit to work together to identify data needed for such measurement,undertake to improve the quality and timeliness of that data, and enable sharing across agencies.Priority ActionsStatusProgress of AustralianGovernment Response (Year One) There have been some appointments to leadershippositions, including a Lived Experience Executive Directorin the NMHC and advertisement of a Director of LivedExperience in the NSPO2.1 All governments integrate livedexperience expertise into leadershipand governance structures for suicideprevention. The recruitment advertisements for other positions in theNSPO did not explicitly include prioritisation or integrationof lived experience knowledge and expertise into theplanning and delivery of the NSPO’s whole-of-governmentpriorities or governance Many more lived experience appointments will be requiredto fully integrate lived experience expertise into leadershipand governance structures for suicide prevention Lived experience engagement in the development ofthe National Agreement was limited, there was oneconfidential engagement with representative bodies andconsumer peaks but no significant opportunity to adviseon this important agreement The National Agreement commits to collaboration withpeople of lived experience however at the governancelevel this is limited to input rather than a governance role2.2 All governments include a requirementfor demonstrated engagement andco-design with people who havelived experience of suicide in fundedresearch, services and programs.www.suicidepreventionaust.org No clear progress on this priority action, the LeadershipProgram and other procurement levers could be used toinclude requirements for lived experience engagement todemonstrated engagement with people who have livedexperience7
Priority ActionsStatusProgress of AustralianGovernment Response (Year One) While there has been a commitment for peer workerscholarships for the mental health system and the releaseof mental health peer workforce guidelines, there hasbeen no investment specific to the suicide prevention peerworkforce2.3 All governments commit adequatefunding and implement supportstructures to build the lived experienceworkforce, including the livedexperience peer workforce. Specific commitments and resources are needed todevelop the suicide prevention lived experience workforceas distinct from the mental health workforce Activity funding for lived experience leadership in theNational Suicide Prevention Leadership Support Program(NSLPLP) may provide some support Activity funding for lived experience leadership in theNational Suicide Prevention Leadership Support Program(NSLPLP) includes lived experience support2.4 A ll governments increase livedexperience research, particularlyfocused on people who haveexperienced suicidal distress and/orattempted suicide.Lived experience knowledge and leadership is essentialto driving down suicide rates. Only with the courage,insight and wisdom of those who have been touchedby suicide will we create meaningful change. The FinalAdvice recognises the need for lived experience tobe integrated in all aspects of suicide prevention fromplanning and policy development through to design,delivery and implementation. The two-year 4 million extension of the National SuicidePrevention Research Fund will enable further livedexperience research and the co-design of research withpeople who have a lived experience of suicide Further concerted and cross-jurisdictional efforts will berequired to increase lived experience research, includingto evaluate suicide prevention interventions and improveunderstanding of fidelity and scalability of programs.To fully integrate lived experience into all that we dorequires change and investment. The 2022 Budgetfailed to deliver funds for supporting structures or thesuicide prevention peer workforce. Investment is neededto support people with lived experience to genuinelypartner with governments and across the sector.Much more is needed to progress this priority. There hasbeen some progress with the welcome development ofpeer workforce guidelines, a 3.1 million commitmentto scholarships and a new activity in the NSPLP. Sadly,early opportunities to prioritise lived experience acrossroles in the NSPO and in the development of the NationalAgreement have been missed.8www.suicidepreventionaust.org
Data and evidence todrive outcomesFinal Advice Recommendation: Recognising that measurement of outcomes is essential to monitor impacts ofsuicide prevention initiatives, all governments commit to work together to identify data needed for such measurement,undertake to improve the quality and timeliness of that data, and enable sharing across agencies.Priority ActionsStatusProgress of AustralianGovernment Response (Year One) Suicide registers have been established in NSW, QLD,VIC, TAS3.1 All jurisdictions maintain or, where notalready in place, establish a suicideregister and mechanisms for the routinecollection and timely sharing of data onsuicide, suicide attempts and self-harm.3.2 Regular national surveys to determinethe population prevalence of suicidalideation, self-harm and suicideattempts and to ensure adequate datacapture – including in relation to prioritypopulations. Suicide registers are progressing in ACT, NT and SA There has been no commitment to a register in WA More work is required to increase timely sharing of data atthe local level. There are major gaps in data on self-harmand suicide attempts that need to be addressed as apriority across a number of community data points The National Mental Health and Wellbeing survey wasundertaken last year however results released to datehave not included any substantial suicide preventiondata, including the estimated number of annual suicideattempts. More comprehensive results are to be releasedin mid-2022 including the number of Australians includingself-harm and suicidality This was the first time the survey was commissioned in 12years and there is no clear commitment to regular surveys The Government has also committed 30.5m fundingover 7 years to measure mental health in the Aboriginaland Torres Strait Islander population. The survey will beco-designed and implemented with Aboriginal and TorresStrait Islander peoples, to ensure it is culturally appropriateand meets the needs of the community The Government has committed 18.8 million over 3 yearsfrom 2022-23 to undertake a child mental health andwellbeing study with at least one follow-up survey3.3 The National Office for SuicidePrevention to lead: (a) the developmentof a national outcomes frameworkfor suicide prevention, informed bylived experience, to be applied at theprogram and service level as well as thenational level; and (b) the developmentof national definitions of, and standardsfor, self-harm and suicide attempts.www.suicidepreventionaust.org The NSPO has been established, with responsibility forthese actions, but it is unclear yet whether progress isbeing made on these priorities The National Agreement commits to developing andreporting on a range of indicators, outcome measuresand KPIs which reflect the objectives and goals of theAgreement9
Priority ActionsStatus3.4 A ll jurisdictions work with the NationalOffice for Suicide Prevention to setpriorities for suicide prevention researchand share knowledge for continualimprovement.Data, evidence and research need to inform all thatwe do in suicide prevention. Major progress has beenmade with the Australian Institute of Health and Welfare’sSuicide and Self-Harm Monitoring System. The systemhas reduced the delay in access to data on suicidedeaths and provided further insights into ambulanceattendances and emergency department presentations.A 4 million two-year extension to the National SuicidePrevention Research Fund has also been delivered andwill drive important translational research.Notwithstanding these developments, more is stillneeded to provide local, real-time and accessible data.Without increased access to this data, when and whereit’s needed, service providers and policy makers will be10Progress of AustralianGovernment Response (Year One) No clear progress on this priority actionconstrained to provide timely and targeted responses todistress. We still lack a full national picture and remainingjurisdictions need to establish suicide registers and toimprove attempt, distress and self-harm data.The National Agreement makes a welcome commitmentto national outcomes for suicide prevention across arange of areas. This work is urgently needed and shouldbe developed with the sector and people with livedexperience. Outcomes need to enable both sharedand individual accountability across a range of service,access and distress indicators and more broadly toassess a whole-of-government approach.www.suicidepreventionaust.org
Workforce and communitycapabilityFinal Advice Recommendation: All governments to commit to prioritising evidence-based and compassionfocused workforce development to drive cultural change in and improve the capacity and capability of all (formal andinformal) workforces involved in suicide prevention.Priority ActionsStatusProgress of AustralianGovernment Response (Year One) Activity five of the NSPLSP includes a focus on nationalsuicide prevention training A Mental Health and Suicide Prevention Unit has beenestablished in the Australian Public Service Commissionand includes a focus on public sector capability building4.1 A ll jurisdictions resource contemporaryand evidence-based training for clinicaland other health staff. All jurisdictionsimplement contemporary compassionbased training for frontline workers thatenable them to respond to distress– especially those providing financial,employment and relationship support topeople experiencing distress. The 2021-22 Budget included support for generalpractitioners and other medical practitioners by providingspecialised training and resources to enhance theircapacity to address mental health concerns of patients The government is also providing compassion-basedtraining for workers in the justice system supportingpeople with mental health conditions 60.7 million has been committed to implement the10-year National Mental Health Workforce Strategy (theStrategy), to deliver a sustainable, skilled, supported andequitably distributed mental health workforce to meetAustralia’s current and future needs. The Australian Government is working with states andterritories to establish a national Distress Intervention Trial.An agreement has been reached with NSW and QLD tofund two trials in each jurisdiction The NSPO has been established but there is no significantprogress on this priority at this stage4.2 T he National Office of SuicidePrevention works with all jurisdictionsand relevant stakeholders to lead thedevelopment of a national suicideprevention workforce strategy. The National Agreement commits to the NSPO developinga National Suicide Prevention Workforce Strategy thatwill include government departments, social services,educators, employer groups, miscellaneous serviceproviders, community-based organisations and othersettings where a risk of suicide may present for individuals The NSPO needs to be properly resources to undertakethis significant workTraining for evidence-based suicide prevention capabilityshould be as common in the community as CPR andFirst-Aid. The Final Advice recognises this for clinicaland health staff and frontline workers supporting peopleexperiencing distress. While 18 million over threeyears in the NSPLP will provide some investment in thistraining, more is required and additional resources areneeded to build community capability.Key investments in new services and supports willnot succeed without commensurate investment in thesuicide prevention workforce. The lack of progress onwww.suicidepreventionaust.orga National Suicide Prevention Workforce Strategy risksundermining other important reforms. A comprehensive,fully-funded National Suicide Prevention WorkforceStrategy and implementation plan is needed. Thisstrategy should outline the long-term vision for theworkforce and specific actions to ensure accessibility,capability, skills, supply, retention and sustainability. Thisneeds to include social supports and other non-clinicalsupports to reconnect people who have survived suicideattempts with their families and communities.11
Respond earlier to distressFinal Advice Recommendation: As a priority action and reform, all governments work together to developand implement responses that provide outreach and support at the point of distress, to reduce the onset ofsuicidal behaviour.Priority ActionsStatus5.1 C oordinated cross-jurisdictional andcross-portfolio action to interveneearly in life to: (a) mitigate the impactsof adverse childhood experiences; (b)strengthen supports for families; and(c) ensure early access to programs,treatment and support for children andyoung people.5.2 D eveloping, implementing andevaluating a scalable early distressintervention for people experiencing:(a) intimate relationship distress; (b)employment or workplace distress; (c)financial distress; and (d) isolationand loneliness.5.3 Implementing and evaluatinginterventions that support peoplethrough transitions, including: (a)entering or being released from justicesettings; (b) leaving military service; (c)finishing or disengaging from educationor vocational settings; (d) enteringretirement; and (e) engagement withaged or supported care services.Unequivocally, the evidence supports responding earlierto distress. Early intervention delivers better socialand economic outcomes and benefits individuals andthe broader community. The Final Advice importantlyrecognises the need for governments to work togetherand better support people earlier and at the point ofdistress.There has been limited progress to date on the priorityactions outlined in the Final Advice. A new NationalChildren’s Mental Health and Wellbeing Strategy and12Progress of AustralianGovernment Response (Year One) The National Children’s Mental Health and WellbeingStrategy was launched in 2021 supported by 317million in funding including new Head to Health Kidsmultidisciplinary hubs, parenting education and support,perinatal mental health intimations and Kids Helpline. Thisbuilds on the existing National Support for Child and YouthMental Health Program A number of 2021-22 Budget initiatives support interveningearlier in life, including perinatal mental health screening,new child mental health and wellbeing hubs, onlineparenting education programs and initiatives to preventand better respond to child sexual abuse in all settingsas well as other initiatives focused on child mental healthand wellbeing The 2021 Budget committed to a brief distressintervention trial. The Commonwealth has entered agreements with NSW,QLD and Victoria to trial this intervention, it is not includedin other bilateral agreements. The National Agreement commits to improve mental healthand suicide prevention outcomes for those who interactwith the justice system including through implementingbest practice programs and increased data collection The Government has established a Royal Commissioninto Defence and Veteran Suicide. The systemic analysisof the contributing risk factors, including the possiblecontribution of transition arrangements, has been includedas an area of focus within the Royal Commission’s Termsof Reference The National Suicide Prevention Leadership SupportProgram has also funded activities to address thisrecommendationseveral Budget announcements commit to earliersupports for children, but it is unclear how thesespecifically address priorities of the Final Advice.Funding has been committed to a trial a Distress BriefIntervention Trial. To date, not all jurisdictions haveagreed to progress a trial under bilateral agreements.More is required to implement and evaluate a range ofinterventions that support people through transitions thatmay occur at a point of distress.www.suicidepreventionaust.org
Connecting people tocompassionate servicesand supportsFinal Advice Recommendation: All governments work together to progress service reform to achieve integrated,connected and quality services for people experiencing suicidal distress, people who have attempted suicide as wellas caregivers and people impacted by suicidal behaviour.This includes all governments working together to implement priority actions from the National Suicide PreventionStrategy for Australia’s Health System 2020-2023 and the National Mental Health and Wellbeing PandemicResponse Plan.Priority ActionsStatusProgress of AustralianGovernment Response (Year One) Head to Health Centres have been announced and fundedacross Australia and a focus will be on the integration ofdigital and face-to-face services Testing of digital transformation is underway and followsextensive engagement6.1 I ntegrated digital and face-to-facesupports to improve accessibility,service options and appropriate levelsof service. Standards have been released by the AustralianCommission on Safety and Quality in Health Care toimprove the quality of digital mental health serviceprovisions and describe the level of care andsafeguards required The Initial Assessment and Referral Tool (IAR) has beenrolled out in Head to Health Centres as part of phoneservice. This is designed to improve accessibility, promoteintegration, support consistency and enable referral toappropriate services6.2 N ew service models incorporatingcompassionate community-basedsupport for people experiencingsuicidal distress.6.3 A ftercare services for anyone who hasattempted suicide or experienced asuicidal crisis.6.4 Timely and compassionate supportsfor families, friends, caregiversand impacted communities,including bereavement andpostvention responses.www.suicidepreventionaust.org No signiifcant progress on this priority action The 2021 Budget included 6.6 million to implementnational standards for Safe Spaces services The 2021 Budget committed to universal aftercare subjectto a National Agreement with States and Territories Agreement has been reached to deliver universal aftercarein NSW, the Northern Territory, Queensland and the ACTbut not South Australia The 2021 Budget committed to universal aftercare subjectto a National Agreement with States and Territories Agreement has been reached to ensure all people in NSW,QLD and the NT have access to postvention but not in theACT and SA13
Priority ActionsStatus6.5 Connecting alcohol and other drugprevention and treatment services toour suicide prevention approachAny Australian experiencing or impacted by suicidaldistress should have access to compassionate, qualityand connected services when they need them. Thisrecommendation makes critical suggestions to delivermuch-needed support to those at-risk, those who haveattempted suicide or those who are bereaved by suicide.Despite substantial Commonwealth investment, muchmore work is required to achieve universal access toaftercare. Bilateral agreements with New South Walesand Victoria, the Northern Territory, Queensland andthe Australian Capital Territory commit to universalaftercare in these jurisdictions. However, no such clear14Progress of AustralianGovernment Response (Year One) The National Agreement commits to improve coordinationbetween services, clear pathways for people withco-occurring alcohol and other drug use and mentalillness, ensuring warm referrals from services andintegrated services The Agreement also commits to develop a nationallyconsistent approach to data collection to understandprevalence, sharing research and findings and buildworkforce capabilitycommitment has been reached with South Australia.Similarly, postvention is not included in bilateralagreements with the South Australian and AustralianCapital Territory Governments.A previous suicide attempt is among the highest riskfactors for a future suicide death. Aftercare has beenproven to reduce suicide, yet around half of thosedischarged from an emergency department followi
made, but there's 'unfinished business' when it comes to suicide prevention and the national reform agenda. We need to finish what we've started. Implementation matters and it's time to get on with it. All recommendations from the Final Advice must be implemented.