Transcription
Cognitive Behavioral Therapy forSuicide PreventionGregory K. Brown, Ph.D.VA/DoD Clinical Practice Guideline for SuicidePrevention Webinar SeriesApril 27, 2021Penn Center for the Prevention of Suicide
Disclaimer and Disclosure Dr. Brown’s views and opinions expressed in thispresentation do not necessarily state or reflect those ofthe United States Government including the Departmentof Veterans Affairs and the Department of Defense. Dr. Brown receives royalties from the ResearchFoundation for Mental Hygiene for the commercial useof the Columbia Suicide Severity Rating Scale.1
Learning Objectives1. Describe the general approach, rationaleand evidence supporting CognitiveBehavioral Therapy for Suicide Prevention(CBT-SP)2. Describe specific cognitive and behavioralstrategies for reducing risk3. Describe a competency-based training forlearning CBT-SP2
VA/DoD Clinical Practice Guidelinefor the Assessment and Management ofPatients at Risk for Suicide (2019)Strong recommendation for“using cognitive behavioraltherapy-based interventionsfocused on suicideprevention for patients witha recent history of selfdirected violence to reduceincidents of self-directedviolence” (p 27).3
Conceptual Underpinnings of CBT-SP Suicidal behavior is viewed as the primaryproblem rather than a symptom of a disorder Cognitive therapy for suicide prevention is viewedas an adjunctive treatment Suicidal behavior is viewed as a problematiccoping behavior Treatment is brief and focused (10 to 16 sessions)4
Suicidal Thoughts and Behaviorsas Primary TargetsBrown et al. (2005). JAMA, 295, 563-570.5
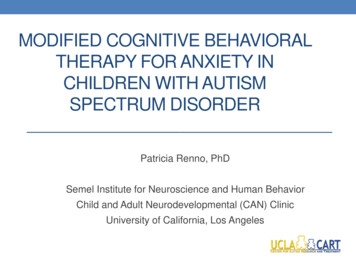
Survival Functions for Repeat Suicide Attemptby Study ConditionCT-SP was associatedwith a 50% reduction insuicide attempts in asevere sample with ahigh rate of repeatattempts.Cumulative Survival1.00.9CT-SP0.80.7*p .05Control0.60.50182364546728DaysSource: Brown et al. (2005). JAMA, 294, 563-370.6
7
Brief Cognitive-Behavioral TherapySoldiers in briefCBT wereapproximately60% less likely tomake a suicideattempt duringfollow-up thansoldiers intreatment asusual.Source: Rudd, Bryan, et al. (2015).AJP, 172, 441-449.8
Cognitive Therapy for Suicide Prevention Initial Phase Informed Consent Motivational Enhancement Suicide Risk Assessment and Narrative Timeline Interview Safety Planning Intervention (Stanley & Brown, 2012) Reasons for Living & Dying and Hope Kit Treatment Goals and Case ConceptualizationMiddle Phase Cognitive & Behavioral Strategies Case Management StrategiesFinal Phase Skill Consolidation Relapse Prevention Task Treatment PlanningWenzel, A., Brown, G. K., & Beck, A. T. (2009). Cognitivetherapy for suicidal clients: Scientific and clinical applications.Washington, DC: APA Books.9
Problems with Treatment Engagement Individuals hospitalized for suicide attemptsoften do not attend outpatient treatment.Potential reasons include: Poor economic resources or practical barriers Negative attitudes toward treatment– Feels hopelessness about getting better, won’t behelpful Culturally-based beliefs about mental healthtreatment (e.g., don’t talk about things like that; helpshould be found within family/church/community, etc.) Mistrust of mental health treatment– Belief is common and valid among Black,Indigenous, people of color (BIPOC) populationsdue to discrimination and racism10
Assess Treatment Expectations Assess attitudes and expectations fortherapy: “What do you expect therapy to be like?” “Do you think therapy will be helpful?” “How willing are you to attend a few therapysessions to see if it would be helpful?” Discuss previous experiences in therapyand how it contributed to any negativeattitudes and expectations: “What happened the last time you went to therapy?How was it helpful? How was it unhelpful?”11
Address the Risks of Treatment Possibility of emotional discomfort Discuss potential strategies that can beimplemented should the client feel upsetfollowing a treatment session Potential negative effects of breachingconfidentiality Collaborate around involving others (includingemergency services) as a general rule Keep clients informed if confidentiality isbroken in emergency situations where youwere not able to discuss this first12
“Case Management” during CBT-SP Go the “extra mile” and reach out to patientsBe flexible in scheduling appointmentsMake reminder and check-in callsSend birthday and holiday cardsDiscuss cases in regular team meetings;frequent use of consultation (“huddles”) toreceive support13
Narrative Interview of Suicidal Crisis Obtain a detailed description of a suicidal crisis(e.g., recent attempt or recent moment whensuicidal ideation increased) Patients are asked to recall the suicidal crisis inas much detail as possible, including theactivating events and reactions to the events. Construct a timeline that indicates the majorexternal events and cognitive, emotional, andbehavioral factors proximal to the crisis Forms the basis of the case conceptualization Understand that suicidal thinking and behavior“makes sense” to the individual in the contextof his or her history, vulnerability, andcircumstances.14
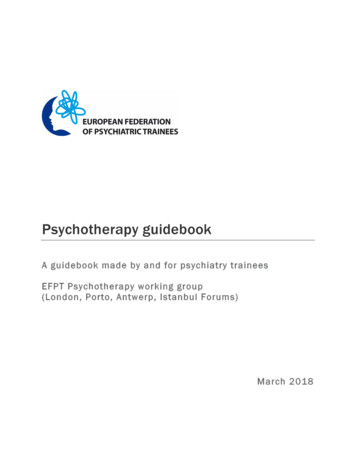
Timeline of Suicide Attempt: ExampleDISTALACTIVATINGEVENT4.5 months ago,wife moves toMichigan w/ kidsKEY AUTOMATICTHOUGHTSWhat do you dowhen everythingis starting to fallapart?AFFECTIVERESPONSEAngerKEY AUTOMATICTHOUGHTSACTIVATINGEVENT”I never thought itwould come tothis.“Commander laidinto me andcalled meirresponsibleBEHAVIORALRESPONSEHad a few beers15
Timeline of Suicide Attempt: ExamplePROXIMALACTIVATINGEVENTArgued with wifeon EHAVIORPut gun to chinand call from afriend interruptedthe attemptTold friendeverything; wentto his place andtaken to clinicoffice.KEY AUTOMATICTHOUGHTS(MOTIVATION)KEY AUTOMATICTHOUGHTS(SUICIDE INTENT)I can’t take thisanymore. I don’tknow what to do.I’m helpless.“”Maybe it wouldbe easier if Iended it.Everything wouldbe fixed.REACTION TOSUICIDALBEHAVIORI don’t want to die16
CBT-SP Focuses on Modifiable Risk Factors Case Conceptualization and Selection of CBTStrategies: Each treatment session addresses thoughts,beliefs, and behaviors that are most proximallyrelated to the suicidal crisis and contribute to andmaintain hopelessness. Select CBT-SP strategies that are perceived byboth the clinician and patient to be the mosthelpful in preventing a future suicidal act.17
Hope Kit Identify and discuss reasons fordying and reasons for living Construct a Hope Kit or Survivor Kitto create a representation ofreasons for living Pictures Letters Poetry Prayer Card Coping Cards Meaningful mementos or tokens18
Common CBT-SP Strategies Behavioral Activation Used to increase meaningful or purpose-drivenactivities, strengthen or enhance reasons forliving, increase social connectedness, etc. Cognitive Restructuring Used to help individuals to identify and evaluatesuicide-related thoughts; increase cognitiveflexibility. Coping Cards Used to remind individuals of importantconclusions from therapy that can be easily usedin a crisis.19
Thought Record ExampleDate Situation12/18Automatic FeelingsThoughtsAlternativeResponseOutcomeWhat eventled to theunpleasantemotion?Whatthoughtswent throughyour mind?Whatemotionswere youfeeling?Use questions toWhatevaluate the thought. emotion doyou feel now?What will youdo?Checked themailNothing butbillsNo holidaycardsNo onewould careif I wasdead (95%)Sad (80)Lonely (90)Not many peoplesend cards anymore.It doesn’t meanpeople don’t care. Igot a call from mycousin the other dayand Carlene invitedme to Christmasdinner. They wouldtake it really hard if Ikilled myself becausethey really do care.I believe theoriginalthought 20%now.Not so down,actually, moreoptimistic(50)Still a littlelonely (30)I’ll call afriend andmake plans.20
Sample Coping Card Automatic Thought: “It’s too much; it’sover, there’s nothing you can do about it.” Adaptive Response: “Things have beenbad before. You always come out of itbetter in the end.”21
Common CBT-SP Strategies Planful Problem Solving Used to help individualsbrainstorm andevaluate potentialsolutions to solveproblems withoutresorting to suicide. Examine Pros and Cons Used to help individualsresolve ambivalenceand make importantdecisions.Locking firearm in safe andgiving key to KeatsProsConsStaying on trackin treatment; If Ikill myself,treatment won’thelpI would be givingin to what otherstell meIt would makemy family feelbetterI won’t have it forprotectionIt might make itmore “out ofsight, out ofmind”22
Review and Consolidate Skills Reviewing coping skills: “Which skills were most helpful in reducing your suicidalideation and desire for suicidal behavior?” “What have you learned through this experience?” “What further goals do you have for yourself?” If the patient has difficulty generating a list ofspecific CBT coping strategies, then they maynot be ready for the later phase of treatment Preparation for the Relapse Prevention Task23
Relapse Prevention Task Goals Rehearse coping with future crises. Assess treatment progress. Determine if additional sessions are alCrisiswith 4
Age-adjusted Suicide Rates, by Sex: US, 1999-2019Hedegaard et al. NCHS Data Brief. 2021 Feb;(398):1-8.25
Suicide Rates for Females by Age Group: US, 1999-2019Hedegaard et al. NCHS Data Brief. 2021 Feb;(398):1-8.26
Suicide Rates for Males by Age Group: US, 1999-2019Hedegaard et al. NCHS Data Brief. 2021 Feb;(398):1-8.27
Risk Factors for Suicide Among Older Adults Older adults have a lower lifetime prevalence ofsuicide attempts than younger adults Suicidal ideation is a major risk factor for death bysuicide for older adults Older adults often experience significant loss (e.g.,death of partner, medical problems, independence,etc.) that increases risk Older men are often reluctant to disclose suicidalideation to others Older men are likely to engage in “passive” suicidalbehavior (e.g., failing to take prescribed medications)28
Adapting CBT-SP for Older Men Greater focus on reducing suicidal ideation Treatment length was extended from 10 sessionsto 16/20 sessions to address persistent ideation Pacing was slower. Take your time! Used whiteboards to stay on the agenda andprevent drift Used worksheets and forms with LARGE FONTS Used post-it notes; laminate important informationsuch as Coping Cards Provided written summary of the session andwritten homework assignment with rationale(reminders)29
Cognitive Therapy for Suicidal Older MenAssessed for Eligibility(N 332)Baseline Assessment(N 110)Randomization(N 95)Cognitive Therapy16 Sessions(N 46)Follow-up Assessments1, 3, 6, 9, 12 months(N 34 completed 12M)Case Management16 Telephone Sessions(N 49)Follow-up Assessments1, 3, 6, 9, 12 months(N 42 completed 12M)NIMH: R01MH086572-1A2, PI: Brown GK; ClinicalTrials.gov: NCT0153548230
Cognitive Therapy for Suicidal Older MenInclusion Criteria:1. Suicidal desire or intent in the past month (SSI Items 4 or 5 0)2. Male gender3. 50 years of age or older4. English speaking5. Able to provide informed consent6. Able to attend the study assessment and therapy sessions7. Provide at least 2 verifiable contacts for tracking purposes8. Cognitive Functioning: MMSE 24 and EXIT-25 14Exclusion Criteria:1. Needed priority treatment for a substance use disorder or PTSD2. Taking antidepressant medication for less than four weeks orchange in antidepressant medicationNIMH: R01MH086572-1A2, PI: Brown GK; ClinicalTrials.gov: NCT0153548231
Demographics Mean age 60.68 (SD 5.68; Range 50-80) Race: 51.6% Black 41.1% White 1.1% Asian/Pacific Islander 1.1% American Indian 5.3% Other Ethnicity: 0% Hispanic/Latinx 95% were VeteransNIMH: R01MH086572-1A2, PI: Brown GK; ClinicalTrials.gov: NCT0153548232
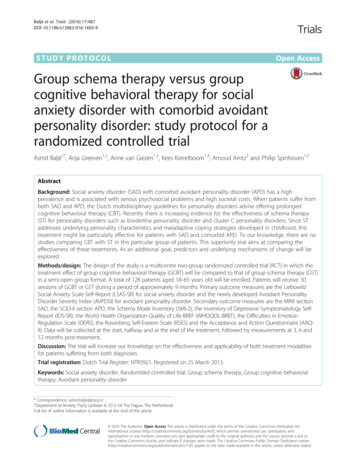
Columbia Suicide Severity Rating ScaleSeverity of Ideation Scale:Worst Point Since Last Assessmentb -0.05; p .02; 95% CI: -0.10 to -0.01NIMH: R01MH086572-1A2, PI: Brown GK; ClinicalTrials.gov: NCT0153548233
Columbia Suicide Severity Rating ScaleIntensity of Ideation Scale:Worst Point Since Last Assessmentb -0.24; p .01; 95% CI: -0.43 to -0.05NIMH: R01MH086572-1A2, PI: Brown GK; ClinicalTrials.gov: NCT0153548234
Acknowledgements Co-Investigators Research PersonnelKelly L. Green, PhDAaron T. Beck, MDDavid W. Oslin, MDMichael Thase, MDWarren Bilker, PhDGabriela Khzanov, PhDAshley Bush, MMHJae S. Cha, PsyDPatrizia Salani Platt, MSEdGuy Weissinger, PhD, RNBridget Moran, MPH Study TherapistsAriel Domlyn, MAShari Jager-Hyman, PhDKristin Pontoski Taylor, PhD Peter Awad, MAJennifer Greene, MSLaura Mowery, PsyDMichelle Gordon, MPHAbby Adler Mandel, PhDKaroline Myhre, MEdKeith Bredemeier, PhDSpecial thanks to the VISN 4 MIRECC, CPL Michael J Crescenz VA Medical Center35
VA CBT-SP Telehealth Pilot ProgramWell Vets: CBT-SP for Veterans with Substance UseDisorders (N 300): RCT comparing CBT-SP vs supportivepsychotherapy on suicide outcomes over 2-year follow-up.VA OMHSP: Pilot of CBT-SP using a telehealth “hub andspoke model” at VISN 10 and VISN 19.36
VA CBT-SP Telehealth Pilot Program VA OMHSP “SP 2.0” Initiative: National telehealthexpansion of Evidenced-Based Psychotherapies(EBPs) for suicide prevention Adapted CBT-SP for telehealth delivery with Drs.Gregory Brown and Craig Bryan: Developed VACBT-SP Therapist Manual and CBT-SP Workbookfor Veterans Delivered via VA Video Connect with Veteransparticipating primarily from home Pilot clinics received over 375 referrals from VISNs10 and 19; Over 190 Veterans were enrolled andcompleted at least 1 CBT-SP session37
Overview of VA CBT-SP Training Program16Weeks3 Weeks1 WeekSelf-StudyWeek Readingfoundationalliterature Becomingfamiliar with themanual Completing anumber of webbased trainingsTrainingWorkshopPhase Instruction fromSMEs Groupdiscussions Role Plays ExperientialexercisesIndependentStudy Manual Review Listening to recordedexample sessions Partnered Role Plays Telehealth PracticeConsultPhase Beginning to seeVeterans Attending weeklyconsultation calls Submittingrecorded sessionsfor Adherence andCompetencyevaluationCertificateofCompletion Successfulcompletion oftrainingrequirements38
VA CBT-SP Team and Acknowledgements Leads: Mark Ilgen, PhD & Jennifer Olson-Madden, PhD Master Trainer: Erin Goldman, LMSW Pilot/Training Coordinator: Samantha Lhermitte, MSW Special thanks to: VISN 19: Ann Weatherby, LICSW, Lisa M. Betthauser,PHD, MBA, Matthew Podlogar, PhD, Herbert Nagamoto,MD VISN 10: Susan Shadley, LMSW, Sarah Emeritz, LMSW,Ann Jones, LMSW, Jessica Curtis, LMSW, ChristinaBoozer, LMSW, Jesse Burgard, PhD, Reiko Buckles,LMSW, Lisa Valentine, PhD, Nicole Stromberg, MD OMHSP: Jessica Walker, PhD, Andrew Moon, PhD,Catherine Rotolo, MSSA, LISW-SQuestions?: Samantha.Lhermitte@va.gov39
Advanced Training in theSafety Planning Intervention (ASPI) For VA providers who regularly encounter Veterans at elevated riskfor suicide and routinely complete safety plans Sponsored by the VA Office of Mental Health and Suicide Prevention(OMHSP)Training Program StaffRoleDr. Wendy BatdorfASPI Program CoordinatorDr. Greg BrownASPI Master Trainer and Subject Matter ExpertSheena SharmaASPI Program AdministratorDrs. Chris Crowe, Mandy Kumpula, EricDedert, Kristine Day, Wendy Batdorf,ASPI Program Development, Leadership, andGreg Brown, Barbara Stanley, Jeff Hoerle Evaluation Team40
ASPI Program SummaryTrainingComponentTraining Participant ActivitiesComponent 1:DidacticTrainingInteractive training with video skill demonstrations: Program Orientation Review VA Safety Planning Manual, SPI competencymeasures & Safety Plan Note Template User Guide ASPI Web-based Training courseComponent 2:ExperientialTrainingExperiential role-play exercises with individualized feedback fromTraining ConsultantsComponent 3:ParticipantEvaluationIndividual evaluation of SPI using standardized patient role playsand standardized rating measures of fidelityComponent 4:Follow-UpEvaluationFollow-up individual evaluation of SPI using standardized patientrole plays and standardized rating measures of fidelityDiscussion of implementation challenges41
Advanced Training in the Safety PlanningIntervention: Resources and Contact ASPI Program SharePoint VA Safety Planning Intervention Manual Brief SPI Checklist for VA Providers Safety Planning and suicide prevention articles Links to additional VA Suicide Prevention resources andtrainings ASPI Web-based Training Course (TMS #43804) Available to all VA providers ASPI Training Program Overview - Rocky MountainMIRECC CPG Series presentation by Dr. Wendy Batdorf August 24th at 12pm ET Contact Dr. Wendy Batdorf, ASPI Training ProgramCoordinator: wendy.batdorf@va.gov42
THANK YOU!43
Risk assessmentFree consultation and resources forany provider in the community or VAwho serves Veterans at risk for suicide.Request a consult: srmconsult@va.govLethal means safety counselingConceptualization of suicide riskBest practices for documentationStrategies for how to engageVeterans at high riskProvider support after a suicide loss(Postvention)www.mirecc.va.gov/visn19/consult
Join us next month for theMay 2021 CPG WebinarVirtual Webinar onWHO BIC as a Strategyto Prevent SuicideAfter Hospitalization5/25/21 @ 12:00 ETFor virtual webinar registration details go to:https://www.mirecc.va.gov/visn19/cpg/presented byDr. Natalie Riblet
Apr 23, 2021 · “using cognitive behavioral therapy-based interventions focused on suicide prevention for patients with a recent history of self-directed violence to reduce incidents of self-directed v