Transcription
VA/DOD CLINICAL PRACTICE GUIDELINE FORTHE MANAGEMENT OF POSTTRAUMATICSTRESS DISORDER AND ACUTE STRESSDISORDERDepartment of Veterans AffairsDepartment of DefenseClinician SummaryQUALIFYING STATEMENTSThe Department of Veterans Affairs and the Department of Defense guidelines are based upon the bestinformation available at the time of publication. They are designed to provide information and assistdecision making. They are not intended to define a standard of care and should not be construed as one.Neither should they be interpreted as prescribing an exclusive course of management.The Clinical Practice Guideline is based on a systematic review of both clinical and epidemiologicalevidence. Developed by a panel of multidisciplinary experts, it provides a clear explanation of the logicalrelationships between various care options and health outcomes while rating both the quality of theevidence and the strength of the recommendation.Variations in practice will inevitably and appropriately occur when clinicians take into account the needs ofindividual patients, available resources, and limitations unique to an institution or type of practice. Everyhealthcare professional making use of these guidelines is responsible for evaluating the appropriateness ofapplying them in the setting of any particular clinical situation.These guidelines are not intended to represent TRICARE policy. Further, inclusion of recommendations forspecific testing and/or therapeutic interventions within these guidelines does not guarantee coverage ofcivilian sector care. Additional information on current TRICARE benefits may be found at www.tricare.milor by contacting your regional TRICARE Managed Care Support Contractor.Version 3.0 – 2017
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryTable of ContentsI.Introduction. 3II.How to Use the Clinical Practice Guideline . 3III. Recommendations . 5A.Grading Recommendations. 8IV. Algorithm . 10Module A: Acute Stress Reaction/Disorder . 11Module B: Assessment and Diagnosis of Posttraumatic Stress Disorder . 13Module C: Management of Posttraumatic Stress Disorder . 15V.Scope of the Clinical Practice Guideline . 16VI. Guideline Work Group . 16VII. Recommendation Discussion . 17A.General Clinical Management . 17a.b.c.Patient-centered Care . 17Shared Decision Making . 17Collaborative Care . 18B.Diagnosis and Assessment of Posttraumatic Stress Disorder . 18C.Prevention of Posttraumatic Stress Disorder . 19a.b.D.Treatment of Posttraumatic Stress Disorder . 19a.b.c.d.e.f.g.h.i.E.Selective Prevention of Posttraumatic Stress Disorder. 19Indicated Prevention of Posttraumatic Stress Disorder and Treatment of Acute Stress Disorder . 19Treatment Selection . 19Psychotherapy . 20Pharmacotherapy . 21Augmentation Therapy . 24Prazosin. 24Combination Therapy . 25Non-pharmacologic Biological Treatments . 25Complementary and Integrative Treatments . 25Technology-based Treatment Modalities . 26Treatment of Posttraumatic Stress Disorder with Co-occurring Conditions . 26a.Background on Co-occurring Conditions with Posttraumatic Stress Disorder. 26Appendix A: Pharmacotherapy Dosing Table . 29References . 30June 2017Page 2 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryI.IntroductionThe Department of Veterans Affairs (VA) and the Department of Defense (DoD) Evidence-Based PracticeWork Group (EBPWG) was established and first chartered in 2004, with a mission to advise the “ HealthExecutive Council on the use of clinical and epidemiological evidence to improve the health of thepopulation across the Veterans Health Administration and Military Health System,” by facilitating thedevelopment of clinical practice guidelines (CPGs) for the VA and DoD populations.[1] This CPG is intendedto provide healthcare providers with a framework by which to evaluate, treat, and manage the individualneeds and preferences of patients with posttraumatic stress disorder (PTSD) and acute stress disorder(ASD), thereby leading to improved clinical outcomes.In 2010, the VA and DoD published a CPG for the Management of Post-Traumatic Stress and Acute StressReaction (2010 PTSD CPG), which was based on evidence reviewed through March 2009. Since the releaseof that guideline, a growing body of research has expanded the general knowledge and understanding ofPTSD and other stress related disorders, such as ASD and other acute reactions to trauma (sometimesreferred to as acute stress reactions [ASR]). Improved recognition of the complex nature of ASR, ASD, andPTSD has led to the adoption of new or refined strategies to manage and treat patients with theseconditions.Consequently, a recommendation to update the 2010 PTSD CPG was initiated in 2015. The updated CPGincludes objective, evidence-based information on the management of PTSD and related conditions. It isintended to assist healthcare providers in all aspects of patient care, including, but not limited to,diagnosis, treatment, and follow-up. The system-wide goal of developing evidence-based guidelines is toimprove the patient’s health and well-being by guiding health providers who are taking care of patientswith PTSD along the management pathways that are supported by evidence. The expected outcome ofsuccessful implementation of this guideline is to:II. Enhance assessment of the patient’s condition and determine the best treatment method incollaboration with the patient and, when possible and desired, the patient’s family andcaregivers Optimize the patient’s health outcomes and improve quality of life Minimize preventable complications and morbidity Emphasize the use of patient-centered careHow to Use the Clinical Practice GuidelineThe VA/DoD PTSD CPG can be used in a variety of ways. It can be used by general clinicians or specialists tostudy and consider the latest information on management of PTSD and how and whether to incorporatethat information or recommendations into their practice. The CPG covers diagnosis and assessment,prevention of PTSD, treatment of ASD, treatment of PTSD, as well as treatment of PTSD in the presence ofco-occurring conditions. Patients can examine the guideline to educate themselves and better understandtheir treatment options and expectations. A healthcare system can use the CPG to assure that its cliniciansand patients have the resources available to compassionately and effectively offer treatment in a timely,June 2017Page 3 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician Summaryculturally sensitive manner. The guideline can also be used to suggest specific education for identifiedgaps.The guideline is not intended as a standard of care and should not be used as such. Standards of care aredetermined on the basis of all clinical data available for an individual case and are subject to change asscientific knowledge and technology advances and patterns evolve. Today there is variation among stateregulations, and the guideline does not cover the variety of ever-changing state regulations that may bepertinent. The ultimate judgement regarding a particular clinical procedure or treatment course must bemade by the individual clinician, in light of the patient’s clinical presentation, patient preferences, andthe available diagnostic and treatment options. As noted previously, the guideline can assist careproviders, but the use of a CPG must always be considered as a recommendation, within the context ofa provider’s clinical judgment and patient values and preferences, in the care for an individual patient.June 2017Page 4 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryIII. Recommendations#RecommendationA. General Clinical ManagementStrengthCategory1We recommend engaging patients in shared decision making (SDM),which includes educating patients about effective treatment options.Strong ForNot Reviewed,Amended2For patients with posttraumatic stress disorder (PTSD) who are treatedin primary care, we suggest collaborative care interventions thatfacilitate active engagement in evidence-based treatments.Weak ForReviewed,New-replacedB. Diagnosis and Assessment of PTSD3We suggest periodic screening for PTSD using validated measures suchas the Primary Care PTSD Screen (PC-PTSD) or the PTSD Checklist (PCL).Weak ForNot Reviewed,Amended4For patients with suspected PTSD, we recommend an appropriatediagnostic evaluation that includes determination of DSM criteria, acuterisk of harm to self or others, functional status, medical history, pasttreatment history, and relevant family history. A structured diagnosticinterview may be considered.Strong ForNot Reviewed,Amended5For patients with a diagnosis of PTSD, we suggest using a quantitativeself-report measure of PTSD severity, such as the PTSD Checklist forDSM-5 (PCL-5), in the initial treatment planning and to monitortreatment progress.Weak ForNot Reviewed,AmendedN/AReviewed,New-replacedStrong ForReviewed,New-replacedN/AReviewed,New-replacedC. Prevention of PTSDa. Selective Prevention of PTSD6For the selective prevention of PTSD, there is insufficient evidence torecommend the use of trauma-focused psychotherapy orpharmacotherapy in the immediate post-trauma period.b. Indicated Prevention of PTSD and Treatment of ASD7For the indicated prevention of PTSD in patients with acute stressdisorder (ASD), we recommend an individual trauma-focusedpsychotherapy that includes a primary component of exposure and/orcognitive restructuring.8For the indicated prevention of PTSD in patients with ASD, there isinsufficient evidence to recommend the use of pharmacotherapy.D. Treatment of PTSDa. Treatment Selection9We recommend individual, manualized trauma-focused psychotherapy(see Recommendation 11) over other pharmacologic and nonpharmacologic interventions for the primary treatment of PTSD.Strong ForReviewed,New-added10When individual trauma-focused psychotherapy is not readily availableor not preferred, we recommend pharmacotherapy (seeRecommendation 17) or individual non-trauma-focused psychotherapy(see Recommendation 12). With respect to pharmacotherapy and nontrauma-focused psychotherapy, there is insufficient evidence torecommend one over the other.Strong ForReviewed,New-addedJune 2017Page 5 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician Summary#b. PsychotherapyRecommendationStrengthCategory11For patients with PTSD, we recommend individual, manualized traumafocused psychotherapies that have a primary component of exposureand/or cognitive restructuring to include Prolonged Exposure (PE),Cognitive Processing Therapy (CPT), Eye Movement Desensitization andReprocessing (EMDR), specific cognitive behavioral therapies for PTSD,Brief Eclectic Psychotherapy (BEP), Narrative Exposure Therapy (NET),and written narrative exposure.Strong ForReviewed,New-replaced12We suggest the following individual, manualized non-trauma-focusedtherapies for patients diagnosed with PTSD: Stress Inoculation Training(SIT), Present-Centered Therapy (PCT), and Interpersonal Psychotherapy(IPT).Weak ForReviewed,New-replaced13There is insufficient evidence to recommend for or againstpsychotherapies that are not specified in other recommendations, suchas Dialectical Behavior Therapy (DBT), Skills Training in Affect andInterpersonal Regulation (STAIR), Acceptance and CommitmentTherapy (ACT), Seeking Safety, and supportive counseling.N/AReviewed,New-replaced14There is insufficient evidence to recommend using individualcomponents of manualized psychotherapy protocols over or in additionto the full therapy protocol.N/AReviewed,New-added15We suggest manualized group therapy over no treatment. There isinsufficient evidence to recommend using one type of group therapyover any other.Weak ForReviewed,New-replaced16There is insufficient evidence to recommend for or against traumafocused or non-trauma-focused couples therapy for the primarytreatment of PTSD.N/AReviewed,Amendedc. Pharmacotherapy17We recommend sertraline, paroxetine, fluoxetine, or venlafaxine asmonotherapy for PTSD for patients diagnosed with PTSD who choose notto engage in or are unable to access trauma-focused psychotherapy.Strong ForReviewed,New-replaced18We suggest nefazodone, imipramine, or phenelzine as monotherapy forthe treatment of PTSD if recommended pharmacotherapy (seeRecommendation 17), trauma-focused psychotherapy (seeRecommendation 11), or non-trauma-focused psychotherapy (seeRecommendation 12) are ineffective, unavailable, or not in accordancewith patient preference and tolerance. (NOTE: Nefazodone andphenelzine have potentially serious toxicities and should be managedcarefully.)Weak ForReviewed,New-replaced19We suggest against treatment of PTSD with quetiapine, olanzapine, andother atypical antipsychotics (except for risperidone, which is a StrongAgainst, see Recommendation 20), citalopram, amitriptyline,lamotrigine, or topiramate as monotherapy due to the lack of strongevidence for their efficacy and/or known adverse effect profiles andassociated risks.Weak AgainstReviewed,New-replaced20We recommend against treating PTSD with divalproex, tiagabine,guanfacine, risperidone, benzodiazepines, ketamine, hydrocortisone, orD-cycloserine, as monotherapy due to the lack of strong evidence fortheir efficacy and/or known adverse effect profiles and associated risks.Strong AgainstReviewed,New-replaced21We recommend against treating PTSD with cannabis or cannabisderivatives due to the lack of evidence for their efficacy, known adverseeffects, and associated risks.Strong AgainstReviewed,New-addedJune 2017Page 6 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician Summary#22RecommendationStrengthCategoryThere is insufficient evidence to recommend for or againstmonotherapy or augmentation therapy for the treatment of PTSD witheszopiclone, escitalopram, bupropion, desipramine, doxepin, D-serine,duloxetine, desvenlafaxine, fluvoxamine, levomilnacipran, mirtazapine,nortriptyline, trazodone, vilazodone, vortioxetine, buspirone,hydroxyzine, cyproheptadine, zaleplon, and zolpidem.N/AReviewed,New-replacedd. Augmentation Therapy23We suggest against the use of topiramate, baclofen, or pregabalin asaugmentation treatment of PTSD due to insufficient data and/or knownadverse effect profiles and associated risks.Weak AgainstReviewed,New-replaced24We suggest against combining exposure therapy with D-cycloserine inthe treatment of PTSD outside of the research setting.Weak AgainstReviewed,New-added25We recommend against using atypical antipsychotics, benzodiazepines,and divalproex as augmentation therapy for the treatment of PTSD dueto low quality evidence or the absence of studies and their associationwith known adverse effects.Strong AgainstReviewed,New-replaced26There is insufficient evidence to recommend the combination ofexposure therapy with hydrocortisone outside of the research setting.N/AReviewed,New-added27There is insufficient evidence to recommend for or against the use ofmirtazapine in combination with sertraline for the treatment of PTSD.N/AReviewed,New-replacedWeak ede. Prazosin28aFor global symptoms of PTSD, we suggest against the use of prazosin asmono- or augmentation therapy.28bFor nightmares associated with PTSD, there is insufficient evidence torecommend for or against the use of prazosin as mono- oraugmentation therapy.f. Combination Therapy29In partial- or non-responders to psychotherapy, there is insufficientevidence to recommend for or against augmentation withpharmacotherapy.N/AReviewed,New-replaced30In partial- or non-responders to pharmacotherapy, there is insufficientevidence to recommend for or against augmentation withpsychotherapy.N/AReviewed,New-replaced31There is insufficient evidence to recommend for or against startingpatients with PTSD on combination pharmacotherapy New-replacedg. Non-pharmacologic Biological Treatments32There is insufficient evidence to recommend for or against the followingsomatic therapies: repetitive transcranial magnetic stimulation (rTMS),electroconvulsive therapy (ECT), hyperbaric oxygen therapy (HBOT),stellate ganglion block (SGB), or vagal nerve stimulation (VNS).h. Complementary and Integrative Treatments33There is insufficient evidence to recommend acupuncture as a primarytreatment for PTSD.N/AReviewed,New-replaced34There is insufficient evidence to recommend any complementary andintegrative health (CIH) practice, such as meditation (includingmindfulness), yoga, and mantram meditation, as a primary treatment forPTSD.N/AReviewed,New-replacedJune 2017Page 7 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician Summary#Recommendationi. Technology-based Treatment ModalitiesStrengthCategory35We suggest internet-based cognitive behavioral therapy (iCBT) withfeedback provided by a qualified facilitator as an alternative to notreatment.Weak ForReviewed,New-replaced36We recommend using trauma-focused psychotherapies that havedemonstrated efficacy using secure video teleconferencing (VTC)modality when PTSD treatment is delivered via VTC.Strong ForReviewed,AmendedE. Treatment of PTSD with Co-occurring Conditions37We recommend that the presence of co-occurring disorder(s) notprevent patients from receiving other VA/DoD guideline-recommendedtreatments for PTSD.Strong ForReviewed,New-added38We recommend VA/DoD guideline-recommended treatments for PTSDin the presence of co-occurring substance use disorder (SUD).Strong ForReviewed,New-replaced39We recommend an independent assessment of co-occurring sleepdisturbances in patients with PTSD, particularly when sleep problemspre-date PTSD onset or remain following successful completion of acourse of treatment.Strong ForReviewed,New-replaced40We recommend Cognitive Behavioral Therapy for Insomnia (CBT-I) forinsomnia in patients with PTSD unless an underlying medical orenvironmental etiology is identified or severe sleep deprivationwarrants the immediate use of medication to prevent harm.Strong ForReviewed,AmendedA. Grading RecommendationsThe Champions and Work Group used the Grading of Recommendations Assessment, Development andEvaluation (GRADE) system to assess the quality of the evidence base and assign a grade for the strengthfor each recommendation. The GRADE system uses the following four domains to assess the strength ofeach recommendation: [2] Balance of desirable and undesirable outcomes Confidence in the quality of the evidence Patient or provider values and preferences Other implications, as appropriate, e.g.,: Resource use Equity Acceptability Feasibility Subgroup considerationsUsing this system, the Champions and Work Group determined the relative strength of eachrecommendation (Strong or Weak). A strong recommendation indicates that the Work Group is highlyconfident about the balance between desirable and undesirable outcomes. If the Work Group is lessconfident of the balance between desirable and undesirable outcomes, they give a weak recommendation.June 2017Page 8 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryThey also determined the direction of each recommendation (For or Against). A recommendation for atherapy or preventive measure indicates that the desirable consequences outweigh the undesirableconsequences. A recommendation against a therapy or preventive measure indicates that the undesirableconsequences outweigh the desirable consequences.Occasionally, instances may occur when the Work Group feels there is insufficient evidence to make arecommendation for or against a particular therapy or preventive measure. This can occur when there isan absence of studies on a particular topic that met evidence review inclusion criteria, studies included inthe evidence review report conflicting results, or studies included in the evidence review reportinconclusive results regarding the desirable and undesirable outcomes.Using these elements, the grade of each recommendation is presented as part of a continuum: Strong for (or “We recommend offering this option ”) Weak for (or “We suggest offering this option ”) No recommendation for or against (or “There is insufficient evidence ”) Weak against (or “We suggest not offering this option ”) Strong against (or “We recommend against offering this option ”)June 2017Page 9 of 34
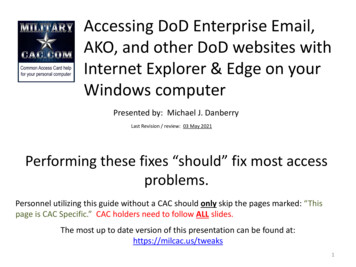
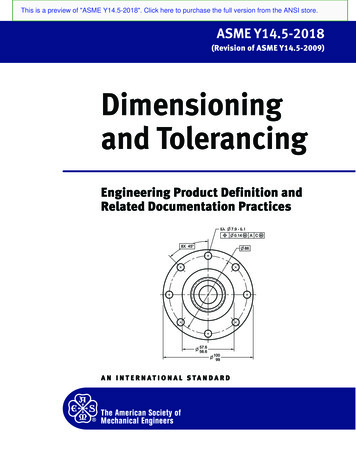
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryIV. AlgorithmThis CPG includes an algorithm that is designed to facilitate understanding of the clinical pathway anddecision making process used in management of PTSD. The use of the algorithm format as a way torepresent patient management was chosen based on the understanding that such a format may promotemore efficient diagnostic and therapeutic decision making and has the potential to change patterns ofresource use. Recognizing that some clinical care processes are non-linear, the algorithm format attemptsto help the provider to follow a more simplified approach whenever possible in assessing the criticalinformation needed at the major decision points in the clinical process, and includes: An ordered sequence of steps of care Recommended observations and examinations Decisions to be considered Actions to be takenA clinical algorithm diagrams a guideline into a step-by-step decision tree. Standardized symbols are usedto display each step in the algorithm, and arrows connect the numbered boxes indicating the order inwhich the steps should be followed.[3]June 2017Page 10 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryModule A: Acute Stress Reaction/DisorderJune 2017Page 11 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryJune 2017Page 12 of 34
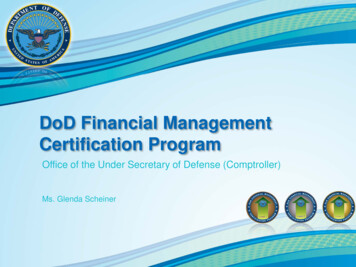
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryModule B: Assessment and Diagnosis of Posttraumatic Stress DisorderJune 2017Page 13 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryJune 2017Page 14 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryModule C: Management of Posttraumatic Stress DisorderJune 2017Page 15 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryV.Scope of the Clinical Practice GuidelineThe VA/DoD PTSD CPG is designed to assist providers in managing or co-managing patients with PTSD andrelated conditions (e.g., ASD). Moreover, the patient population of interest for the CPG is adults who areeligible for care in the VA and DoD healthcare delivery systems. It includes Veterans as well as deployedand non-deployed active duty Service Members, Guard, and Reserve. The CPG does not providerecommendations for the management of PTSD in children or adolescents. Regardless of setting, anypatient in the healthcare system should ideally have access to the interventions that are recommended inthis guideline after taking into consideration the patient’s specific circumstances.While these guidelines are broadly recommended, their implementation is intended to be patientcentered. Thus, treatment and care should take into account a patient’s needs and preferences. Goodcommunication between healthcare professionals and the patient is essential and should be supported byevidence-based information tailored to the patient’s needs. Use of an empathetic and non-judgmentalapproach facilitates discussions sensitive to gender, culture, ethnic, and other differences. The informationthat patients are given about treatment and care should be culturally appropriate and available to peoplewith limited literacy skills. It should also be accessible to people with additional needs such as physical,sensory, or learning disabilities. Family involvement should be considered, if appropriate.VI. Guideline Work GroupGuideline Work GroupDepartment of Veterans AffairsDepartment of DefenseNancy C. Bernardy, PhD (Champion)Charles W. Hoge, MD (Champion)Matthew J. Friedman, MD, PhD (Champion)David S. Riggs, PhD (Champion)Paula P. Schnurr, PhD (Champion)Megan J. Ehret, PharmD, MS, BCPPKathleen M. Chard, PhDMaj Joel T. Foster, PhDLori Davis, MDCOL Shawn F. Kane, MD, FAAFP, FACSMBradford Felker, MDKate McGraw, PhDJessica L. Hamblen, PhDCDR Jeffrey Millegan, MD, MPH, FAPAMatthew Jeffreys, MDElaine P. Stuffel, BSN, MHA, RNSonya Norman, PhDCOL Lisa A. Teegarden, PsyDMary Jo Pugh, RN, PhD, FACMPHCDR Meena Vythilingam, MDSheila A.M. Rauch, PhD, ABPPCOL Wendi M. Waits, MDTodd P. Semla, MS, PharmD, BCPS, FCCP, AGSFJonathan Wolf, MDOffice of Quality, Safety and ValueVeterans Health AdministrationOffice of Evidence Based PracticeU.S. Army Medical CommandEric Rodgers, PhD, FNP, BCJames Sall, PhD, FNP-BCRene Sutton, BS, HCACorinne K. B. Devlin, MSN, RN, FNP-BCElaine P. Stuffel, BSN, MHA, RNJune 2017Page 16 of 34
VA/DoD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder – Clinician SummaryGuideline Work GroupLewin GroupECRI InstituteClifford Goodman, PhDChristine Jones, MS, MPH, PMPErin Gardner, BSAnjali Jain, MDJames Reston, MPH, PhDAmy Tsou, MD, MScRebecca Rishar, MLISJeff Oristaglio, PhDSavvas Pavlides, PhDSigma Health Consulting, LLCDutyFirst ConsultingFrances Murphy, MD, MPHAnita Ramanathan, BAMegan McGovern, BAVII. Recommendation DiscussionA.General Clinical Managementa. Patient-centered CareVA/DoD CPGs encourage clinicians to use a patient-centered care approach that is individualized based onpatient needs, treatment goals, prior treatment experience, and preferences. Whenever possible, allpatients in the healthcare system should be offered access to evidence-based interventions. Whenproperly executed, patient-centered care may decrease patient anxiety, increase trust in clinicians, andimprove knowledge and treatment adherence.[4,5] As part of the patient-centered care approach,clinicians should review the outcomes of previous self-change efforts, past treatment experiences, anddiscuss these outcomes (including reasons for treatment dropout) with the patient. Clinicians shouldexplain treatment options to patients including the benefits of accepting a referral to a mental healthspecialist, an expert in evidence-
18 We suggest nefazodone, imipramine, or phenelzine as monotherapy for the treatment of PTSD if recommended pharmacotherapy (see Recommendation 17), trauma-focused psychotherapy (see