Transcription
The Social and Emotional Well-Being ofChildren in Foster CareBy Nina Williams-Mbenguefunctioning, physical health and development,behavioral/emotional function and social functioning.A. IntroductionJust over 415,000 children and youth in the U.S.currently reside in foster care. While this number ishigh, it represents a significant decline in foster careplacements over the past decade, with the number ofchildren in foster care decreasing by almost a quarterbetween 2002 and 2013.1A federal and state-level focus on the safety andpermanency of children in care has been an importantfactor contributing to the decline in caseloads. Despitesuch progress, state child welfare systems continue tostruggle with the social and emotional well-being ofchildren in care, particularly for children with complexbehavioral and mental health disorders.2Definition of Child Well-Being. Child well-being isdescribed by the federal Administration for Children,Youth and Families in its April 2012 InformationMemorandum (ACYF-CB-IM-12-04) as,“ children’s behavioral, emotional and socialfunctioning—those skills, capacities andcharacteristics that enable young people tounderstand and navigate their world in healthy,positive ways.” 3The administration has further identified four primarydomains for measuring well-being: cognitiveChild well-being is an important focus for statesbecause of its lifelong impact on children and theirsuccess as productive adults. State policymakers nowunderstand that children and youth in foster care facelong-term risks from their exposure to violence, childmaltreatment and other adverse childhood experiencesand are anxious to identify and implement strategiesthat will minimize the long term consequences forchildren and the costs to state budgets. Fortunately,there is also an increasing body of evidence-basedprograms that state child welfare systems can developto significantly improve children’s well-being.This extended edition newsletter focuses on the socialand emotional well-being of children and youth in fostercare. The newsletter will provide information on thesocial and emotional characteristics and needs ofchildren in care, discuss the impact of childmaltreatment and trauma on children’s developmentand examine state and local policies and practices toaddress the well-being of children in foster care.Additionally, the legislative role in improving child wellbeing will be considered.B. Why is the Social and Emotional Well-Being ofChildren in Foster Care at Risk?The social and emotional well-being of children in fostercare is jeopardized by the conditions that lead to their
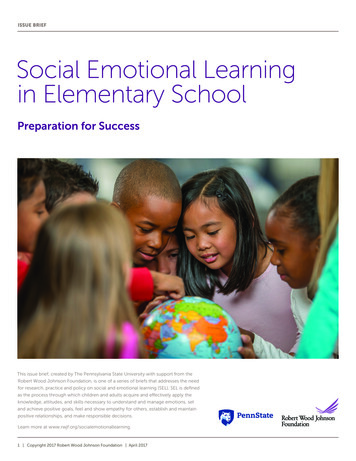
removal from home, as well as their experiences once incare. While the number of children in placement hasbeen reduced in the last decade from more than511,000 in 2005 to 415,000 in 2014, little data existsabout the well-being of children in care.4 Additionally,effective indicators of well-being have not beenidentified or measured routinely.make a child vulnerable and that may impact the child’swell-being.The Well-Being of Children Who Enter Foster CareThe Impact of a Child’s Experiences While in FosterCareChildren who are placed in foster care for theirprotection have experienced many conditions that maythreaten their safety and well-being. As the table belowindicates, the majority of children who are confirmedfor child maltreatment are victims of neglect.In addition to abuse and neglect, children who enterfoster care may have been exposed to parentalsubstance abuse, domestic and community violence andpoverty.The removal from home can be devastating andconfusing for children. Once in foster care, children mayexperience prolonged stays in care. According to 2014AFCARS data, of the 238,230 children who exited fostercare in Fiscal Year 2014, 53 percent had been in care 12months or more.6Children’s Length of Stay in Foster Care in Fiscal Year2014Number ofPercent inLength of Stay inChildrenCareCare94,35823%1 - 5 Months83,97820%6 – 11 Months62,44715%12 – 17 Months39,62010%18 – 23 Months29,4017%24 – 29 Months18,8335%30 – 35 Months36,2929%3 – 4 Years28,0587%5 Years or MoreThough defined differently from state to state, neglectis often a complex combination of conditions that mayinclude: 5 Physical neglect, such as abandonment orfailure to provide for a child’s nutritional orother physical needs.Inadequate supervision, such as exposure tohazards or lack of appropriate caregivers;Medical neglect through denial or delay ofhealth care.Emotional neglect, such as inadequatenurturing or affection, social isolation, chronicor extreme spouse abuse.Neglect of a child’s educational needs.Newborns addicted or exposed to drugs.After child neglect, the most common reason forremoval is parental substance abuse. Other removalreasons include caretaker inability to cope, childbehavior, physical abuse, and other conditions thatThe longer a child is in placement, the greater thechance that he or she will move from one fosterplacement to another, placing the child at further risk ofnegative social and emotional outcomes. 7,8 Frequentmoves mean that the child faces continuing disruptionof relationships with friends, siblings and otherrelatives, coaches, teachers, classmates, religiousleaders and others. Children may move from theiroriginal schools multiple times during the school year.Frequent changes in caseworkers, judges and legalrepresentation also interfere with child well-being andachievement of a permanent home. 9The Behavioral and Mental Health Needs of Children inFoster CareRecent research from the National Survey of Child andAdolescent Well-Being finds that children and youth infoster care have high levels of mental health needs andthat those needs are not being met. Children and youthin foster care with mental health disorders stay in foster
care longer, rely more on expensive residentialtreatment placement, experience more moves in care,have higher involvement with the criminal justicesystem and have poorer educational outcomes.10 Eighty percent of youth involved with the childwelfare system require mental healthintervention and services due todevelopmental, behavioral or emotionalissues.11Children in foster care utilize mental healthservices at five to eight times the rate of otherMedicaid-eligible children.12difficulties they may experience in foster care. Intoadulthood, children and youth who have undergonetraumatic experiences may have problems ranging fromdepression and addiction to cancer, diabetes and heartdisease.19C. The Costs of Poor Social and Emotional Well-BeingThe social and emotional well-being of children whoenter foster care has tremendous consequences— bothon the course of their lives and on the long term coststo taxpayers. Children and youth in residential treatmentcenters (the majority of whom come from thechild welfare system) have higher rates ofmental and behavioral health disorders thanchildren in the general population.13The total annual cost of child abuse and neglectin the U.S. in 2012 has been estimated to be 80.2 billion. Children in foster care are more likely to usemultiple psychotropic medications thanchildren that are not in the child welfaresystem.14Compared to other Medicaid-eligible youth,children in foster care have two to eight timesthe rates of various psychiatric medicationprescribing.15The Pew Center on the States estimates thecosts to society to pay for medical and mentalhealth services annually is more than 30,000for each abused child.20 For children in fostercare, mental health expenditures are 8 to 11.5times greater than the expenditures for otherMedicaid eligible children.21 In addition to Medicaid costs for direct healthservices of children in foster care, such as inpatient treatment or dental services, statesspend more than 1 billion in Medicaid for childwelfare services. Of the 39 states thatresponded to a recent survey of FY2010 statechild welfare expenditures, 27 reported that thenumber one use of Medicaid dollars by childwelfare systems was for rehabilitative servicessuch as residential and behavioral modificationtreatment, followed by targeted casemanagement and therapeutic foster care. 22Impact of TraumaIt is estimated that 90 percent of children in foster carehave been exposed to trauma.16 A comprehensivereview of children entering foster care in one staterevealed that one in four exhibited trauma symptomsrequiring treatment.17 The term “complex trauma”describes children's exposure to multiple or prolongedtraumatic events, which are often invasive andinterpersonal in nature. Complex trauma exposureinvolves the simultaneous or sequential occurrence ofchild maltreatment, including psychologicalmaltreatment, neglect, exposure to violence andphysical and sexual abuse. Trauma can be compoundedby the removal of children from their families, lovedones, and communities and by adverse experiences infoster care. A growing body of research reveals negativelong-term consequences of traumatic stress, especiallyrepeated exposure to trauma such as might beexperienced by children who have been abused orneglected, on physical, cognitive, social and emotionalfunctioning. 18 Children’s relationships and attachmentsto caretakers can be affected, further exacerbatingRecent research also shows that multiple, negativeevents in childhood, such as those experienced by manychildren in foster care, have costly health consequencesthat can impact state budgets for many years. TheAdverse Childhood Experiences Study (ACES) is alongitudinal examination of health outcomes for adultswho experienced a variety of multiple, negative eventsin childhood such as child maltreatment, exposure todomestic violence, living with substance abusingparents, growing up with a growing up with a mentallyill or incarcerated parent or parental abandonmentthrough divorce or death. The study indicates significanteffects well into adulthood, including:23
Child Maltreatment Impacts: Brain Function andStructureNeuroscience teaches us that the early experiences ofyoung children have a tremendous influence on theirdeveloping brains. Healthy emotional and cognitivedevelopment is shaped by responsive, dependableinteraction with adults, while chronic or extremeadversity, such as extreme poverty, caregiver substanceabuse or mental illness, exposure to violence or familyhardship without appropriate adult support, can causeexcessive amounts of the cortisol hormone to beproduced resulting in toxic stress, which disruptsdeveloping brain circuits. This kind of prolongedactivation of the stress response systems can not onlydisrupt the development of brain architecture and otherorgan systems, but can also increase the risk for stressrelated disease and cognitive impairment well into theadult years.24Despite the potential for significant harm to youngchildren’s health development, studies show thatproviding supportive, responsive relationships as earlyin life as possible can prevent or reverse the damagingeffects of toxic stress.25 In addition, emerging sciencehas deepened the understanding of adolescentcapabilities and behaviors and the ability to impactbrain development through adolescence. Neurosciencehas made clear that the brain is not “done” by age 6 aswas previously believed.26Instead, the adolescent brain continues to develop,providing a window of opportunity similar to that whichis open in early childhood. Young people can build andpractice resiliency and develop knowledge and skillsthat will positively serve them throughout adulthood.View NCSL’s Extending Foster Care Policy Toolkit formore. Alcoholism and drug abuse.Heart disease.Cancer.Lung disease.Depression and suicide.Obesity.Fetal death.Health-related quality of life.Unintended pregnancies and adolescentpregnancy.Early initiation of smoking.In addition to the long term costs associated withtreating and responding to many of theseconsequences, repeated, negative childhoodexperiences contribute to reduced economicproductivity. Dr. Robert Anda, co-principal investigatorof the ACES Study, reported that annual workforce costsdue to adverse childhood experiences included 28billion for chronic back pain, 40 to 44 billion formedical costs, reduced productivity, and absenteeismdue to depression and 246 billion for substanceabuse.27D. What State Legislators Can Do to Promote theSocial and Emotional Well-Being of Children inChild Welfare Systems To combat the damaging effects of childmaltreatment, trauma and adversity, childwelfare leaders at federal, state and local levelsare developing policies and financing strategiesto address social and emotional well-being.State lawmakers can partner with them to focuson: Prevention of maltreatment and otheradverse childhood experiences that contributeto traumatic stress and long term negativeoutcomes.Improving experiences of children who must beplaced in temporary foster care, by reducinglength of stay, multiple moves from oneplacement to another, overuse or inappropriateuse of psychotropic medications, high turnoverof caseworkers, and other harmful practices,while maintaining and strengtheningconnections with kin.Increasing access to comprehensive early andperiodic assessments that includesocial/emotional functioning.Ensuring effective treatment of trauma and ofbehavioral/mental health problems for childrenin foster care, including authorization ofevidence-based and evidence-informed servicesand training for in-home service providers,foster parents, courts, and others.Leveraging existing resources and fundingopportunities, and reinvesting in effectivepractices and strategies that contribute topositive well-being.
Needs and gaps in the service array and accessacross programs and agencies, as well asunnecessary duplication.Policy barriers and solutions.Funding opportunities and limitations.Concrete action steps to improve the well-beingof the state’s young people.Following are several examples of this type of legislativeleadership.NCSL reviewed recent state policy and legislativeinitiatives from 2008-2015 to identify areas in whichstate legislatures have been active, including conveningchild and family system leaders, promoting thecoordination of mental health, health and child welfare,encouraging comprehensive screening and assessment;implementing evidence-based services and encouragingthe use of Medicaid to improve the social andemotional well-being of children in foster care.Convening Child and Family Services System LeadersLegislators are uniquely positioned to convene keydecision makers from other branches of government, aswell as leaders of multiple state agencies, to addressthe social/emotional well-being of children. As state andlocal leaders, legislators have the ability to increaseawareness of child well-being and to bring togetherstakeholders who can impact outcomes. Thesestakeholders include the courts, which have a criticalrole in considering the social and emotional functioningof each child in their decisions and ensuring that thecourt experience itself is not traumatic, as well as stateagencies which have a role in Medicaid, child mentalhealth, health care systems, substance abuse,education, early childhood and juvenile justiceprograms, as well as the child welfare system. At thelocal level, the array of resources that contribute towell-being include schools, community serviceproviders, foster parents, and many others.28Together these stakeholders can identify: Shared outcomes and common measures forchild well-being, as well as strategies for sharinginformation to support effective treatment forchildren in foster care.Strengths, resources, and connections acrossagencies that can be maximized to improvewell-being, such as existing assessments andeffective services.Three Branch Institute. In 2013-2014, seven states—Connecticut, Illinois, Kansas, New Mexico, Virginia, WestVirginia and Wisconsin—participated in the ThreeBranch Institute on the Social and Emotional Well-Beingof Children in Foster Care, a two-year initiativefacilitated by a strategic partnership between NCSL, theNational Governors Association Center for BestPractices, Casey Family Programs, the National Centerfor State Courts and the National Council for Juvenileand Family Court Judges. Teams from each participatingstate consisted of representatives from the legislative,executive and judicial branches of government (andtribal officials in some states) working together todevelop and implement coordinated, comprehensivestrategic plans addressing well-being. The executivebranch team members included both child welfare andMedicaid leaders.States were selected through a competitive RFPprocess. In July 2013, teams participated in a two-anda-half day convening where they interacted withnational experts, foster youth, state administrators andtheir colleagues in other states to develop plans,exchange ideas, and discuss barriers and potentialsolutions. States received ongoing technical assistancefrom national experts, participated in educationalwebinars, attended a second national convening andreceived other assistance in 2014.Legislators played an active role in the three-branchpartnerships, sponsoring legislation, sharing ideas,meeting with legislators in other states and developingrelationships with child welfare administrators, judicialleaders and other important stakeholders.Examples of state strategies developed as part of theinstitute included New Mexico’s goal to strengthencollaboration between child welfare and Medicaidsystems to ensure that all children in foster care receivetrauma assessments and appropriate Medicaid-coveredservices. Wisconsin’s team worked to expand acommunity-level pilot project to integrate childhood
trauma-informed practices and policies throughout thestate’s systems that serve children, and to providetrauma-informed training for professionals such asfrontline staff, family court judges, and others. Virginiafocused on improving behavioral and mental healthservices, especially strategies to ensure that psychiatricdrugs are effectively used for children in foster care.Virginia’s child welfare and Medicaid agenciescollaborated to transition children in foster care fromfee-for-service to managed care.Several states that participated in the Three BranchInstitute have continued the partnership to further theirwork on well-being or to tackle other important issues.For more information see Governing magazine’sNovember 2013 article, Coordinating Foster Care Acrossthe Three Branches of Government or to learn aboutwork in Connecticut, see Connecticut Three BranchInstitute.State lawmakers may also want to partner with or learnabout the work of state-level and local partnerships andcollaborative efforts to provide services for children andfamilies with behavioral health needs. Some examplesof such initiatives include the following.Both Michigan and New Jersey developed similarstatewide behavioral health efforts that include highlevel collaboration between the child welfare agency,Medicaid, behavioral health and other state agencies.30While there had been collaboration between the childwelfare and behavioral health systems in Michigan, aconsent decree provided the impetus to use a MedicaidSection 115(c) Home and Community Based Services(HCBS) Waiver which allows states to provide long-termcare services in home and community-based settingsrather than in institutions. The waiver focused onchildren with serious emotional disturbances. TheMichigan effort includes an interagency operationalteam of directors from child welfare, behavioral healthMedicaid and other agencies to overseeimplementation of the partnership.New Jersey’s Children’s Interagency CoordinatingCouncils engage in cross-system planning at the locallevel for children and families with behavioral healthissues. Child-serving agencies partner with parents andyouth to offer an integrated system of care for servingthese families. The councils also identify resource gapsand priorities for resource development.All of these efforts would likely benefit from legislativeparticipation and feedback, as well as legislative abilityto convene stakeholder groups for ongoingcollaboration and planning across state agencies onbehalf children and families with behavioral healthneeds.Promoting the Coordination of Health, Mental Healthand Child WelfareMassachusetts Children's Behavioral Health Initiative.This interagency initiative consists of a comprehensive,wraparound, community-based system of services forfamilies and children with significant behavioral,emotional and mental health needs. The servicesprovide support for families and enable them to bettermaintain their family at home and not in facilities orextended out-of-home placements. The Office ofMedicaid, the Department of Children and Families, theDepartment of Mental Health, juvenile justice and otherstate agencies collaborated to design the new system.The state legislature mandated the creation of aChildren’s Behavioral Health Advisory Council to advisethe governor, the general court and the secretary ofhealth and human services on behavioral health issuesand to make recommendations on best and promisingpractices and on the implementation of the statewidebehavioral health initiative. 29Recent Federal Legislation and Initiatives. Federalpolicies require coordinated approaches to health andmental health care for children in foster care. Fostering Connections to Success and IncreasingAdoptions Act of 2008: requires that states developplans for the oversight and coordination of healthcare services for children in foster care, includingdental and mental health, in coordination withState Medicaid agencies.The Child and Family Services Improvement andInnovations Act of 2011: specifies that state plansmust outline protocols for the appropriate use andmonitoring of psychotropic medications.The Affordable Care Act: requires information abouthealth care be included in the youth’s transitionplans and extends Medicaid coverage for formerfoster youth to age 26. The act also promotesmedical homes for children which would involvecontact with a single health provider.
In July of 2013, the U.S. Department of Health andHuman Services disseminated a Federal GuidanceLetter to state child welfare directors to encouragestates to use trauma-focused screening,assessments and evidence-based practices in childwelfare to improve child well-being.Recent State Legislative Enactments. Legislators in anumber of states have enacted laws related to theoversight and coordination of health and mental healthcare, across state agencies, for children in foster care.Following are recent examples related to oversight andcoordination, health passports, psychotropicmedication oversight and delivery of health careservices. See NCSL’s Mental Health and Foster Care webpage for more.Oversight and Coordination. In 2009, California requireda plan for the oversight and coordination of health careservices for foster children with specific assurances thata child’s mental health needs are to be identified.31Public health nurses are stationed in child welfarecounty offices and are responsible for medical casemanagement to ensure that children and youth in carereceive services, including behavioral health. The nursesprovide training for health, child welfare and probationand juvenile court staff related to children’s behavioraland health needs. The nurses follow each child in careand coordinate with caseworkers, probation officersand caregivers to ensure that the child’s health, mentalhealth and developmental needs are identified andaddressed.32Other states that have enacted legislation mandating acoordinated approach to address children’s health andbehavioral health include Arizona, Connecticut, Texasand Washington.33 In 2013, Arizona legislators requiredthe development of a plan to deliver comprehensivemedical, dental and behavioral health for children infoster care. Also in 2013, Connecticut lawmakersenacted legislation that required the Department ofChildren and Families (which includes child welfare,child mental health services, and juvenile justice andyouth services) to develop a comprehensiveimplementation plan for meeting the emotional andbehavioral health needs of all children in the state. Theplan, must: (1) strengthen families through homevisitation and parenting education programs; (2)increase mental, emotional, or behavioral health issueawareness within elementary and secondary schools;(3) improve the current system of addressing suchissues in youths and (4) provide public and privatereimbursement for some mental, emotional, orbehavioral health services. In 2015, Texas lawmakersdirected the establishment of an integrated managedhealth and behavioral health plan for foster childrenenrolled in Medicaid.Health Passports. In efforts to better coordinatedelivery of important health-related services andsharing of information on such services to children infoster care, at least 32 states have developed someform of health passport system to contain information,accessible to specified entities such as child welfare,Medicaid, and foster parents. 34 A recent example isOklahoma’s 2009 legislation which created a “PassportProgram” to include educational, medical andbehavioral health information for all children in care.The passport must accompany each child to whereverthe child lives while in care.Psychotropic Medications Oversight. Concerns aboutthe overuse of psychotropic medications and newfederal requirements for states to develop protocols forthe use of such medications have prompted states toexamine the use and oversight of psychotropicmedications for children in foster care. California,Colorado, Connecticut, Florida, Illinois, Nevada, NewMexico, Oregon, Texas and Washington all haveaddressed the issue in statute. In 2011, Illinois createdthe Administration of Psychotropic Medications toChildren Act.35 The law required the Department ofChildren and Family Services to promulgate rulesestablishing and maintaining standards and proceduresto govern the administration of psychotropicmedications to children and youth in state care. Suchrules include administration to youth in correctionalfacilities, residential facilities, group homes andpsychiatric hospitals.In 2015, California legislation provided specified rightsfor children who are prescribed psychotropicmedications; required a foster care public health nurseto monitor and oversee a foster child’s use ofpsychotropic medications, provided training for thenurses; and, allowed group foster homes to usepsychotropic medications under certain conditions. Thedepartment is also required to collect data related topsychotropic medication use by children and youth incare and to identify group homes that have high levelsof use, through confidential discussions with formergroup home residents and medical personnel.36
(Early and Periodic Screening, Diagnostic, andTreatment) benefit which provides comprehensive andpreventive health care services for children under age21 who are enrolled in Medicaid.Delivery of Health Care Services. In 2014, lawmakers inCalifornia required the State Department of SocialServices to convene a stakeholder group to identifybarriers to, and make recommendations about, theprovision of mental health services by mental healthprofessionals with specialized clinical training inadoption or permanency issues to children receivingthose medically necessary specialty mental healthservices.37 Also in 2014, Delaware legislators mandatedthe establishment of a task force to analyze the healthand delivery and receipt of health services of children incustody of the state.38North Dakota created a task force on substanceexposed newborns and required a report to thelegislature.39 The task force is charged with researchingthe impact of substance abuse and neonatal withdrawalsyndrome; collecting data on costs associated withtreating expectant mothers and newborns sufferingfrom withdrawal substance abuse; and, identifying andevaluating programs for mothers and newbornssuffering from addiction.Rhode Island mandated a transition plan for all olderchildren under the family court’s jurisdiction and whoare developmentally delayed or seriously emotionallydisturbed, which addresses housing, support services,health insurance and education.40 In 2015, Washingtonlegislators directed the Health Care Authority toestablish an integrated managed health and behavioralhealth plan for foster children and Montana lawmakerscreated a pilot project to improve outcomes for thechildren’s mental health system and an interim study ofevidence- based outcomes.41Promoting Comprehensive Screening and AssessmentState lawmakers are recognizing the importance of thecomprehensive screening and assessment for childrenin care to better identify and address children’s mentaland behavioral health needs. Many states are nowrequiring an immediate assessment of a child’s needsupon entry into foster care. States can use the EPDSTTrauma Assessment and Crisis Intervention. In 2010,West Virginia legislators established a pilot program (tobe known as Jacob’s Law) for children ages 4 to 10 infoster care to provide children in crisis with earlyintervention, assistance with emotional needs, medicalevaluations, independent advocates and foster familytraining and education.42 The law also requiredimmediate evaluation of the child for emotional andphysical trauma following removal from a home.Screening and Assessment of Mental Health TreatmentNeeds. Lawmakers in several states have addressed theissue of appropriate screening and assessment ofchildren in public child welfare systems. In 2011,Michigan lawmakers enacted a bill that required theDepartment of Human Services to use a standardizedassessment tool to ensure greater cooperation betweenHuman Services and the Department of CommunityHealth and to measure the mental health treatmentneeds of every child in care.43 Also in 2011, Minnesotarequired
C. The Costs of Poor Social and Emotional Well-Being The social and emotional well-being of children who enter foster care has tremendous consequences— both on the course of their lives and on the long term costs to taxpayers. The total annual cost of child abuse and neglect in the U.S. in 2012 has been estimated to be 80.2 billion.