Transcription
Anticoagulant in Heart Failure :Who, When and WhyWahyu Aditya, MDGatot Soebroto Central Army HospitalScientific Meeting of Indonesian Heart AssociationWorking Group of Heart Failure2018
DefinitionClinical SyndromeBreathlessness, ankle swelling, fatigueElevated JVP, peripheral edema, rales,ascitesStructural and / or functional cardiacabnormalityResulting in reduced CO and/or increasedintracardiac pressures at rest or during exercise
Classification - per definitioncriteriaType of HFHFrEFHFmrEFHFpEF1Symptoms signsSymptoms signsSymptoms signs2LVEF 40 % LVEF 40 - 49 %LVEF 50 %3-1. Elevated levels ofnatriuretic peptides2. At least one additionalcriterion : Relevant structural heartdisease (LVH and / or LAE) Diastolic dysfunction1. Elevated levels ofnatriuretic peptides2. At least one additionalcriterion : Relevant structural heartdisease (LVH and / or LAE) Diastolic dysfunctionESC guidelines on CHF and AHF 2016
ESC guidelines on CHF and AHF 2016
VTE : A strong relationship betweenDVT and PEAbout 50% of patientswith proximal DVTof the leg have asymptomatic PE1DVT (mainly asymptomatic)is found in around 80%of patients with PE21. Pesavento R, et al. Minerva Cardioangiol 1997;45(7-8) : 369-3572. Girard P, et al. Chest 1999; 11(4): 903-908
Most hospitalized patients have multiple risk factors for VTEe.g :MalignancyPregnancyHormonal therapyInflammatory bowel diseaseSepsisThrombophiliae.g :Major surgeryTraumaChronic indwelling centralvenous cathetherChemotherapyVirchow’striadCirculatory stasise.g :ImmobilityVenous insufficiencyVenous obstruction from tumour, obesity, or pregnancyPolycythemia1.Adapted from Kyrle PA. Lancet 2005;365:1163-74.2.Adapted from Anderson FA, Spencer FA. Circulation 2003;107:I9-I16.3.Wong E, et al.Available from: http://www.pathophys.org/vte/
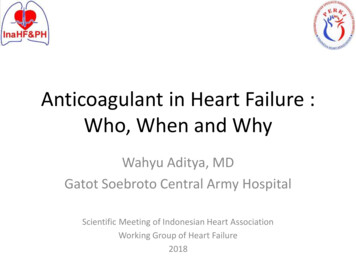
Risk of DVT with no prophylaxis inhospitalized patients1,21LroviczA, et al. Circulation. 2004;110(24 Suppl 1):IV13-9.2The Australia & New Zealand Working Party on the Management and Prevention of Venous Thromboembolism. Best Practice Guidelinesfor Australia & New Zealand. 4th Edition, December 2007.
Substantiate incidence of DVT in high risk group, especially patients confined to bedfor more than 3 days frequency (without prophylaxis) : 10% to 26%. It variesamong races.Fatal PE accounts for 5–10% of all deaths in hospitalized patients.VTE inMedically IllPatientsVTE is associated with increased mortality and long-term morbidity andsubstantial costs for its managementDespite available International guideline, there is a trend that patient is NOTscreened for DVT, especially medically ill patients.Prophylactic UFH or LMWH has shown an approximate 80% reduction in theincidence of DVT.References :Turpie AGG, Leizorovicz A.Postgrad Med J.2006;82:806 – 9; Hirsh J, Lee AYY. Blood.2002;99:3102-10); Turpie AGG, Leizorovicz A.PostgradMed J.2006;82:806 – 9; Angchaisuksiri P.Thromb Haemost.2011;106:585-90.
Majority of hospitalized patients are at risk of VTEVTE risk varied according to medical diagnosis,from 31.2% of patients withgastrointestinal/hepatobiliary diseases to100% of patients with acute heart failure,active noninfectious respiratory disease, orpulmonary infectionGlobal rate, 41.5%Bergmann JF,et al. Thrombosis and Haemostasis 103.4/2010
4.Sandler DA & Martin JF. J R Soc Med 1989; 82; 203-205.5.Cooper JW Jr & Groce J III. Consult Pharm 2001; 16 (suppl D): 7-17.
VTE is Associated with High Economic BurdenThe real-world data confirm the economic burden of in-hospitaltreatment of VTE, and the relatively low costs of thromboprophylaxisTable. Health costs for the two groups of patients, total and for each activity phase in In fact, although a large part of the costs of VTE are associated with managing the acuteevent, there are significant costs related to long-term complications such as recurrent VTE,post-thrombotic syndrome, pulmonary hypertension, and death.Gussoni G, et al.Thrombosis Research.2013;131:17-23.
VTE Management : GuidelinesProphylaxis: ACP Guideline 2016 ESC Guideline on Heart FailureTherapy: Treatment Guidance DVT and PE ACCP Guideline
VTE prophylaxis in hospitalized patientACP GuidelineRecommendationGradeRisk assessmentAssessment of the risk forthromboembolism and bleeding isrecommended in medical patientsprior to initiation of prophylaxis of VTEStrong c prophylaxis withheparin or a related drug for VTE isrecommended in medical patientsunless the assessed risk for bleedingoutweighs the likely benefitsStrong recommendationMechanical prophylaxis Use of mechanical prophylaxis withgraduated compression stockings isnot recommended for prevention ofVTEStrong recommendationAnn Intern Med. 2011;155:625-632.
Ref 564 : ‘Meta-analysis: Anticoagulant Prophylaxis to Prevent SymptomaticVenous Thromboembolism in Hospitalized Medical Patients’ – Dentali F, et al.Ann InternMed.2007;146:278-88
First step is assessing VTE risk of yourpatients Risk Assessment Model (RAM) Padua Prediction Score
Risk assessment modelsIdentify medicalpatients at significantrisk of VTEObjectives of RAMSimplify decisionmakingImprove the use ofappropriateprophylaxisCost containmentReduce the burden of VTERAM risk assessment model.Cohen AT, et al. Thromb Haemost. 2005;94:750-9.
All medical patients should be routinely assessed andconsidered for thromboprophylaxisRisk assessment modelNoIs the patient 40 years old with acute medical illnessand reduced mobility?YesDoes the patient have one of the followingacute medical illnesses/conditions?Evidence-based Acute MI Acute heart failure – NYHA III/IV Active cancer requiring therapy Severe infection/sepsis Respiratory diseases (respiratory failurewith/without mechanical ventilation;exacerbation of chronic respiratorydisease) Rheumatic disease (including acutearthritis of lower extremities, and vertebralcompression) Ischaemic stroke ParaplegiaConsensus view only Inflammatory disorder with immobility Inflammatory bowel diseaseNoDoes the patient have one of thefollowing predisposing risk factors?Evidence-based in acutely ill medicalpatients History of VTE History of malignancy Complicating acute infectious disease Age 75 yearsConsensus-based from strong evidencein other settings Prolonged immobility Age 60 years Varicose veins Obesity Hormone therapy Pregnancy/post-partum Nephrotic syndrome Dehydration Thrombophilia or thrombocytosisYesNo evidence for thebenefits ofNo thromboprophylaxis.However, patientsshould beconsidered forthromboprophylaxison a case-by-casebasisYesIs pharmacological thromboprophylaxis contraindicated?NoLMWH (enoxaparin 40 mg o.d or dalteparin 5,000 IUo.d.) or UFH (5,000 IU q 8 h)YesMechanicalthromboprophylaxis withgraduated compressionstockings or IPC isrecommended(LMWH preferred due to better safety profile)Cohen AT, et al. Thromb Haemost. 2005;94:750-9.
The Padua Prediction ScoreBaseline featuresActive cancer*Previous VTEReduced mobility 3 daysThrombophilic conditionRecent ( 1 month) trauma / surgeryElderly ( 70 years)Heart and/or respiratory failureAcute myocardial infarction / ischemic strokeAcute infection and/or rheumatologic disorderObesity (BMI 30)Ongoing hormonal treatmentScore33332111111*Patients with local or distant metastases and/or in whom chemotherapy or radiotherapy had been performed in the previous 6 monthsHigh risk of VTE : score 4 or more(VTE developed in 11.0% patients without prophylaxis and 2.2% withprophylaxis)Barbad S, et al. J Thromb Haemost.2010;8:2350-7.
DVT Wells ScoreClinical featurePointsActive cancer (treatment ongoing, within 6 months, or palliative)1Paralysis, paresis or recent plaster immobilisation of the lowerextremitiesRecently bedridden for 3 days or more or major surgery within12 weeks requiring general or regional anaesthesiaLocalised tenderness along the distribution of the deepvenous systemPatient score111Entire leg swollen1Calf swelling at least 3 cm larger than asymptomatic side1Pitting oedema confined to the symptomatic leg1Collateral superficial veins (non-varicose)1Previously documented DVT1An alternative diagnosis is at least as likely as DVT 2Clinical probability simplified scoreDVT likelyDVT unlikely2 points or more1 point or lessAdapted from: Wells PS et al. (2003) Evaluation of D-dimer in the diagnosis of suspected deep-vein thrombosis. New England Journal ofMedicine 349: 1227–35
Thromboprophylaxis of Medically ill Patients :Clear Benefits Over EVENT2P 0.0015ARTEMIS3Placebo14.9* (n 288)Enoxaparin 40 mgP 0.00149%45%47%47%45PlaceboP 0.0295.5 (n 291)5.0 (n 1,473)†Dalteparin20Patients with VTE, %2.8 (n 1,518)Placebo10.5‡ (n 323)Fondaparinux*VTE at day 14; †VTE at day 21; ‡VTE at day 15.Adapted from: 1Samama et al. N Engl J Med 1999;341:793-800.2Leizorovicz et al. Circulation 2004;110:874-9.3Cohen et al. Br Med J 2006.5.6 (n 321)NNT number needed to treat;RRR relative risk reduction.
The MEDENOX StudyPrevention ofVenous Thromboembolismin Medical PatientsThe Medenox Study GroupN Engl J Med 1999;341:793-800
MEDENOX: Study DesignRandomized, double-masked, placebo controlledn: 1,102Treatment periodFollow-up periodPlaceboDay -3 nEligible Patients:- Age 40 years- Immobilized for 3days or less- Medical Illness(heart failure, acuterespiratory failure,other conditions)Enoxaparin 20 mgEnoxaparin 40 mgDay 1InclusionRandomizationDay 6-14BilateralvenographyDay 83-110End offollow-upN Engl J Med 1999;341:793-800
Efficacy of LMWHs in Medical Patients- MEDENOX Study P 0.0011614.9 15.0RRR 63%14Patients (%)Placebo12Enoxaparin 20 mgEnoxaparin 40 mgP 0.0410865.54RRR 65%4.9 4.5P NS1.721.0 0.30All VTERRR Relative risk reductionProximal DVT0.0PESamama MM et al. N Engl J Med 1999;341:793–800
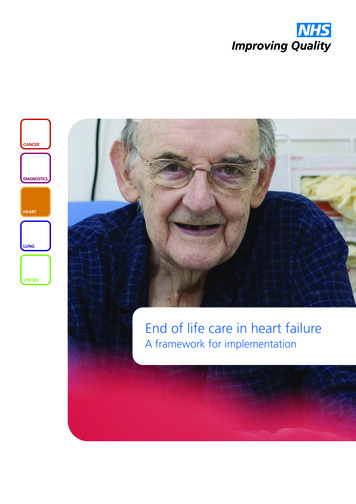
Frequency of VTE from day 1 to 14, in patient subgroups in theMEDENOX studyAcute medical illness (n)Placebo (%)Enoxaparin 40 mg (%)RR (95% CI)P valueHeart Failure (290)- NYHA class III (217)- NYHA class IV (73)14.612.321.74.05.100.29 (0.10 – 0.84)0.42 (0.13 – 1.29)-0.020.20.05Respiratory disease (457)13.13.30.25 (0.10 – 0.65)0.003Infectious disease (463)15.56.30.41 (0.20 – 0.82)0.01Rheumatic disease (78)20.710.00.48 (0.11 – 2.16)0.4A subgroup analysis of the MEDENOX study also showed thatthromboprophylaxis with enoxaparin 40 mg once daily resulted in a significant71% reduction of the risk of VTE among patients with heart failure (NYHA III or IV)compared with placebo.Alikhan R, et al.Blood Coagul Fibrinolysis.2003;14:341-6.
Haemorrhagic Events During Treatment PeriodNo difference in risk of haemorrhage between groups- MEDENOX Study NS15n 5(1.4%)n 4(1.1%)Patients(%)105n 39(10.8%)n 40(11.4%)n 27(7.5%)Injection-sitehaematomaMinor haemorrhageMajor haemorrhage0n 4(1.1%)PlaceboNS, not significantn 1(0.3%)Enoxaparin20 mgn 6(1.7%)Enoxaparin40 mgSamama MM et al. N Engl J Med 1999;341:793–800
Conclusion If neglected, DVT is associated with increased mortality,morbidity and substantial costs for its management International guidelines are available as references for bothprophylaxis and treatment of VTE There are risk assessment tools available to simplycategorize patients according to their risk of developingDVT Routine VTE prophylaxis should be considered anddiscussed after careful assessment of each individualpatients due to it’s established risk-benefit profile.
VTE can be instantly FATAL and fortunately is effectivelyPREVENTABLE
Anticoagulant in Heart Failure : Who, When and Why Wahyu Aditya, MD Gatot Soebroto Central Army Hospital Scientific Meeting of Indonesian Heart Association Working Group of Heart Failure . Relevant structural heart disease (LVH and / or LAE) Diastolic dysfunction ESC guidelines on CHF and AHF 2016. ESC guidelines on CHF and AHF 2016 .




![Heart Failure Pathophysiology.ppt [Read-Only]](/img/29/card08-heartfailurebw.jpg)