Transcription
CANCERDIAGNOSTICSHEARTLUNGSTROKEEnd of life care in heart failureA framework for implementation
AuthorsMichael Connolly, James Beattie, David Walker and Mark DancyHeart Improvement Programme, NHS ImprovementWith contributions from Anita Hayes and Claire HenryNational End of Life Care ProgrammeWe gratefully acknowledge the support of Candy Jeffries and Sheelagh Machinof NHS Improvement in the preparation of this document.
Contents4Foreword5Introduction5The burden of heart failure6The heart failure disease trajectory8Advance care planning9Multidisciplinary working10 What is end of life care in heart failure?The end of life care pathway121416181920Discussions as end of life approachesAssessment, care planning and reviewCoordination of careDelivery of high quality servicesCare in the last days of lifeCare after deathAppendices21 End of life care in heart failure22 Features of a commissioning framework23 Common disease trajectories in heart failure24 References26 Acknowledgements3
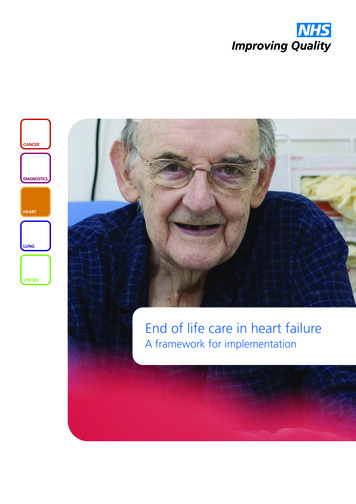
End of life care in heart failure: A framework for implementationForewordIn recent years, we have made enormousstrides in our understanding of heartdisease. We have a wealth of evidenceon what care and treatment approacheswork, the role of new interventions toimprove the outcomes for patients and the quality of services. Consequently, many peoplewith heart disease are now living longer, more productive and more comfortable lives. Wehave also seen great strides in the consistency of care, thanks to the clinical frameworkthat has underpinned and driven the changes.While we celebrate this success, we should also acknowledge that heart disease remains thesecond biggest killer in England. It is also changing its profile; people with heart disease areolder with more long-term care needs. This requires a different approach to ensure that thehigh quality care we have come to expect elsewhere is available at the end of peoples’ lives.Though cancer patients have until recently been the focus of much of the expertisedeveloped by hospices and specialist palliative care services, the National End of Life CareStrategy aims to ensure provision of expert end of life care moves beyond this, to include allthose with life limiting conditions in all care settings. Commissioning end of life care forheart failure patients is particularly challenging. Progression of heart failure is variable andunpredictable, the population often have multiple, and complex needs.For some years the Heart Improvement Programme have been in the vanguard of promotingsupportive and palliative care for people with heart failure and this framework has beendeveloped in collaboration with members of the National End of Life Care Programme. It aimsto help commissioners to understand the complex care environment in which people with heartfailure live and ensure the NHS can deliver sufficiently flexible and responsive services tomeet their needs.We recommend this document to you.Professor Roger BoyleNational Director for Heart Disease and Stroke4Professor Sir Mike RichardsNational Clinical Director for Cancer
End of life care in heart failure: A framework for implementationIntroductionIn 2008, the National End of life CareProgramme published Information forCommissioning End of Life Care1 whichcomprehensively described the issues relevant tocommissioning the complex service provision ofgeneral end of life care. Of necessity, thatpublication offered a relatively genericapproach. This document, End of life care inheart failure - a framework for implementation,sets out to raise awareness of the supportiveand palliative care needs of people living ordying with progressive heart failure, to facilitatethe commissioning of services specificallytailored to meet those needs. It does so in thecontext of the End of Life Strategy2 which aimsto ensure that all adults receive high quality careat the end of life, regardless of their age, placeof care or underlying diagnosis.The burden of heart failureHeart failure is a complex clinical syndromecausing patients to experience breathlessness,fatigue and fluid retention due to functional orstructural cardiac abnormalities. The NationalService Framework for Coronary Heart Disease3described heart failure as the final commonpathway for the many cardiac conditions thataffect heart pump function, with coronary arterydisease and high blood pressure as the mostcommon antecedent conditions.Although the increasingly successfulmanagement of these diseases, particularlyintervention for heart attacks, has improvedsurvival, the trade off lies in a burgeoningclinical cohort living with left ventriculardysfunction. Heart failure is now the onlycardiovascular disease increasing in prevalence.In the United Kingdom, heart failure affectsabout 900,000 people with 60,000 new casesannually, and is predominantly a disease of olderpeople with all their attendant comorbidities4, 5.At least 5% of those aged over 75 years areaffected, rising to about 15% in the very old.Given the relative ageing of the generalpopulation, those with heart failure willcontinue to consume a major and increasingproportion of clinical and public healthresources. Heart failure is a high costHealthcare Resource Group (HRG) and multiplehospital admissions, a common feature ofadvanced heart failure, account for a significantamount of this health care expenditure. For theyear 2007- 2008, there were almost 60,000admissions with heart failure in England andWales, requiring more that 750,000 bed days6.Some of these admissions might be avoidedwith anticipatory care planning and theprovision of community health and social caresupport.Despite therapeutic advances, heart failureremains a progressive, incurable and ultimatelyfatal long term condition which has a majoreffect on affected individuals and their families.The symptomatic burden and mortality risks aresimilar to common cancers and of all generalmedical conditions heart failure has the greatestimpact on quality of life. Despite a growingrecognition of the requirement to providesupportive and palliative care for this clinicalcohort7, 8, the recent National Heart FailureAudit demonstrated continuing significantunmet needs: only 6% of those dying withheart failure were referred to palliative care6.Several factors may contribute to this paucity ofsupport but this often results from prognosticuncertainty and difficulties in defining end-stageheart failure, as evident in the heart failuredisease trajectory.5
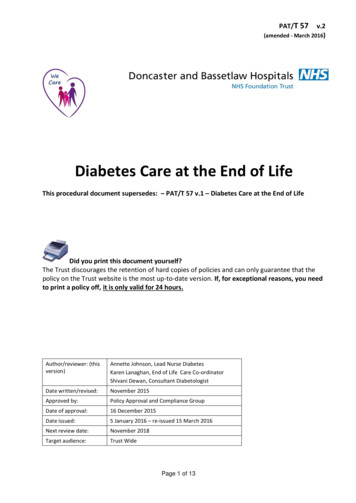
End of life care in heart failure: A framework for implementationFigure 1. The typical course of heart failureModified from Goodlin SJ10, Copyright JACC (2009), with permission from Elsevier.The heart failure diseasetrajectoryCentral to commissioning a high quality, costeffective service is a better understanding of thenature of advanced heart failure and, inparticular, the end of life phase.As described below, the trajectory of heartfailure is comparable to clinical populations withother forms of progressive organ failure such aschronic obstructive pulmonary disease and evento some cancers. However, the course of heartfailure is exceptional in its unpredictability, andfor an individual patient, no specific trajectorycan be reliably anticipated9.A representative disease trajectory for heartfailure is shown diagrammatically in Figure 1.Typically five phases may evolve.6Phase 1 represents symptom onset, diagnosisand initiation of medical treatment. This oftenoccurs as the patient is admitted to hospitalwith a life-threatening episode ofbreathlessness. Some patients may die at thispoint. However, for other patients the onset ofsymptoms is more gradual, and they maypresent to the general practitioner (GP) withslowly progressive fluid retention and/orbreathlessness. With either presentation, oncethe diagnosis is confirmed, treating the patientwith drug therapy, combined with cardiacsurgery if required, will often produce adramatic improvement in symptoms. In theinitial stage patients and carers need educationon the nature of heart failure, the treatmentoptions, and advice on diet and fluidmanagement. Patients usually now enter aplateau period of variable duration, sometimeslasting several years.
End of life care in heart failure: A framework for implementationPhase 2 - During this period, in which patientsgenerally remain under the care of their GP,they should be advised how to monitor theircondition at home and when to call for help.Ongoing support and education for patientsand their carers promote autonomy, self care,adherence to therapy and a reduction in therisk of inappropriate admission. Because lifeexpectancy is so difficult to predict and patientsfeel relatively well, most clinicians are reluctantto talk to patients or carers about prognosis atthis time.Phase 3 occurs when patients develop periodsof instability with recurrence of symptoms linkedto deterioration in heart function. Rebalancingof treatment may restore stability, but often anew approach is required with the use ofimplantable cardiac devices to improve heartpump performance (cardiac resynchronizationtherapy) or to shock the heart back to normalrhythm (implantable cardioverter defibrillator(ICD)) in the event of a life-threateningarrhythmia. Increased patient and carer supportis required here, and there is a major role forBOX 1Poor prognosis is likely in heartfailure patients:11 of advanced age with refractory symptoms despiteoptimal therapy who have had at least three hospitaladmissions with decompensation in lessthan six months who are dependent for more thanthree activities of daily living with cardiac cachexia with resistant hyponatraemia with serum albumen of less than 25g/l who experience multiple shocks fromtheir device with a comorbidity confering a poorprognosis, such as terminal cancercommunity heart failure nurses. Regular reviewincluding home visits may help to avoidunnecessary hospital admissions.As functional deterioration continues, Phase 4 ismarked by the patient experiencing increasingsymptoms and exhibiting declining physicalcapacity, despite optimal therapy. Considerationfor other treatment options such as cardiactransplantation may be considered in this phase.Judging the right time to discuss prognosis andadvance care planning with a patient can bevery difficult, but the reappearance of symptomsin phases 3 and 4 and raising the question ofthe possible need for aggressive interventionoften present an opportunity to initiatediscussion.The course of heart failure and the time spentprogressing through these illness phases is veryvariable and it is important to emphasise thatclinical deterioration and death may occur at anytime (Appendix C). However, as shown (Box 1),clinical features often become evidentsuggesting that the situation is irrecoverablewhen formal end of life care is required.Phase 5. Goals of care need to be openlyreviewed with the treatment emphasis shiftingto the management of symptoms rather thanthe futile continuation of therapy offered onlyfor prognostic benefit. Formal assessment ofsupportive and palliative care needs is requiredat this time and specialist palliative care mayneed to be involved. Multi-organ failure is theusual terminal mechanism in Phase 5, whereassudden arrhythmic cardiac death is morecommon in earlier phases. Review ofresuscitation status and reprogramming ofcardiac devices may be important managementissues. Deactivation of ICDs is frequently leftalmost to the point of death when agonalarrhythmias may trigger device discharges,disturbing the patient and distressing thefamily12. When the patient enters the terminalphase, the situation often progresses rapidly,and unless treatment policies have been definedin advance, care may become disorganised.7
End of life care in heart failure: A framework for implementationAdvance Care PlanningAdvance care planning allows the patient torecord their wishes for care prospectively againstthe possibility of later clinical events limitingtheir ability to engage meaningfully in decisionmaking or communication relevant to theirfuture healthcare.Forms of advance care planning include anadvance statement, advance decision to refusetreatment (ADRT), and lasting power of attorney(LPA). In appointing a LPA, the patient assignsauthority to another individual to contribute todecisions on treatment if capacity is later lost.The LPA requires to be registered with the Officeof the Public Guardian.While not legally binding, advance statementsmust be taken into account by those makingproxy decisions in the patient's best interest. Incontrast, ADRT and LPA are legally binding ifproperly formulated and recorded when thepatient has capacity. All forms of advance careplanning may inform decisions by clinicians onthe policy for cardiopulmonary resuscitation.As outlined in the recently published guidancefrom the General Medical Council, judgingwhen and how to discuss changes in treatmentemphasis, goals of care and advance careplanning with a patient is difficult and often it isleft too late13. Heart failure specialists have onlyrecently started to engage in this practice14. Theresources highlighted may help to facilitate thisprocess. Commissioners should encourageproviders to develop advance care planning, andit is important that such decisions are fullyinformed, regularly reviewed, properly recordedand accessible to providers across all caresectors.8Useful resources:Royal College of Physicians. Advance careplanning. National guideline. London:RCP. (2009).NHS End of Life Care Programme. (2007)Advance care planning: a guide for healthand social care lications/eolc-ccp-and-acp.aspx)NHS End of Life Care Programme. (2010)The differences between general careplanning and decisions made in advance.(http://www.nhsiq.nhs.uk/8595.aspx)
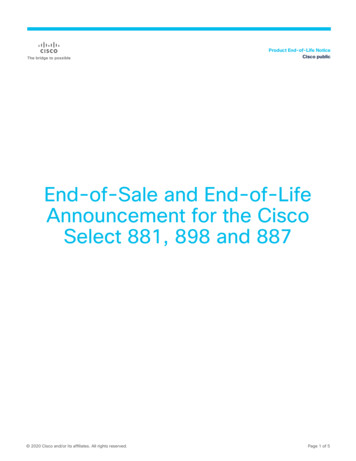
End of life care in heart failure: A framework for implementationMultidisciplinary workingFigure 2 shows the core elements required ofthe necessary multidisciplinary team (MDT)approach to care provision for those withprogressive heart failure.This service model requires contributions from abroad range of social and health service sectorsand good care coordination is necessary toavoid fragmentation. Personalisation of care iscentral; the relative importance of the differentcomponents will be unique to each patient andtheir families and will vary in intensity over thecourse of the illness. Commissioners will need toensure service specifications enable services thatcan be tailored to the needs of individualpatients and their carers and responsive tochanges in those needs.Commissioning of services through a singlepoint of contact may mitigate some of this risk.Successful provision of social caresupport to the carers of patientswith end-stage heart failure hasFigure 2. Patient centred heart failure carebeen developed in the Care-Plusproject, sponsored by the King'sInformationFund, in the London Borough ofAdvance Care PlanningTower Hamlets (www.carerscentrePrimary ve CarePATIENTEmergency CareFunding streams for clinical,social care and voluntary sectorproviders are often discrete.Consequently, tSupportcommissioning requiresinformalfailurepartnership working between thecarerprofessionalSymptomSpiritual CareControlNHS, social services and their localpartners who are significantlyPsychologicalEnd of Life Careinvolved in end of life care.SupportA Joint Strategic NeedsAssessment, which is a statutoryFamily/Bereavement Careresponsibility of the primary caretrust (PCT) and local authority,should establish a shared evidencebased consensus on key local priorities andfacilitate whole system care. In addition, theTransition between different care settingsNational Council for Palliative Care haspresents particular organisational hazards.produced a population-based needs assessmentAt times it can be difficult to ascertain wherefor palliative and end of life care, a national dataresponsibility for care sits, the health service orset to inform commissioners of the needs oflocal authorities and deficiencies and inequitiestheir local populations, including those dying ofin social service provision for older people withcardiovascular diseases such as heart failure17.heart failure have been emphasised15, 16.SpecialistPalliative CareOptimisingDevice Therapy9
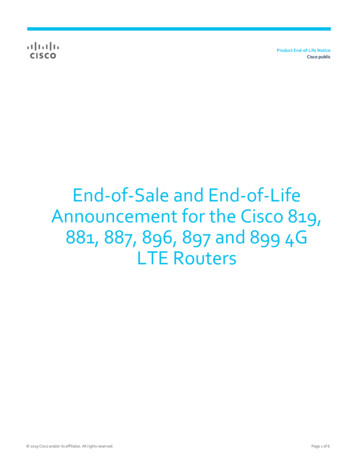
End of life care in heart failure: A framework for implementationWhat is end of life care inheart failure?As shown below, the National Council forPalliative Care has described the features of endof life care18.‘End of life care is care that helpsall those with advanced,progressive and incurableconditions to live as well aspossible until they die. It enablesthe supportive and palliative careneeds of both patient and familyto be identified and metthroughout the last phase of lifeand into bereavement. It includesphysical care, management of painand other symptoms and provisionof psychological, social, spiritualand practical support.’Palliative care providers are expert in holisticassessment and intervention to attend to theneeds of patients and their families. There is aclear role for specialist palliative care in theterminal phase of heart failure and this may beprovided in hospices or hospital baseddepartments or on a consultancy basis in thecommunity. There are several examples ofprofessional collaboration between specialistpalliative care and cardiologists19. However,much general palliative care and supportive carecan be provided by the GP, community or heartfailure specialist nurses. A British HeartFoundation (BHF) initiative exploring thepotential impact of developing a specialist heartfailure nursing service with enhanced palliativecare skills is currently being evaluated. Heartfailure specialist nurses are increasingly working10with palliative care services and may be ideallyplaced to act as care coordinators as proposedin Figure 220. Collaboration between the BHFand Marie Curie Cancer Care in the BetterTogether programme has been shown to benefitthe care of advanced heart failure patients inthe community21. Economic analysis of theMarie Curie Delivering Choice programme inLincolnshire, where local service reconfigurationsuccessfully accommodated patients' wishes todie at home, showed this to be cost neutral22.In this project, 77% of the service users hadcancer and, as proposed in the National AuditOffice review of end of life care, developingsimilar service structures for non-cancer patientssuch as those with heart failure, are likely to becost saving given their greater utilisation ofacute services23.End of life care should be available in all placesof care be it the patient's home, a care home,hospice or hospital - including coronary careunits where many heart failure patients areadmitted. All of the tools highlighted in the Endof Life Care Strategy - such as the GoldStandards Framework, and the PreferredPriorities for Care - are applicable to heart failurepatients, and should be available in all caresettings. These are described fully in the End oflife Care Strategy document which also providesa basis for an integrated approach tocommissioning2. The End of Life Care Strategy isshown in schematic form in Figure 3.Useful ce.org.uk
Figure 3. In the End of life Care Strategy, a whole system care pathway is proposedas a model for commissioning integrated end of life care servicesSTEP 1STEP 2STEP 3Discussionsas the end oflife approachesAssessment,care planningand reviewCoordinationof careSTEP 4STEP 5STEP 6Delivery ofhigh qualityservices indifferentsettingsCare in the lastdays of lifeCare afterdeath Open, honest Agreed care Strategic High qualitycommunication plan andcoordinationcare provision Identifyingregular review Coordinationin all settingstriggers forof needs andof individual Acute hospitals,discussionpreferencespatient carecommunity, Assessing Rapid response care homes,needs of carersserviceshospices,communityhospitals,prisons, securehospitals andhostels Ambulanceservices Identification Recognitionof the dyingthat end of lifephasecare does not Review ofstop at theneeds andpoint of death.preferences for Timelyplace of deathverification and Support forcertification ofboth patientdeath or referraland carerto coroner Recognition Care andof wishessupport of carerregardingand family,resuscitationincludingand organemotional anddonationpracticalbereavementsupportSPIRITUAL CARE SERVICESSUPPORT FOR CARERS AND FAMILIESINFORMATION FOR PATIENTS AND CARERSAdapted from the pathway, National End of Life Care Strategy (2008)11
End of life care in heart failure: A framework for implementationDiscussions as end of lifeapproachesSTEP 1Discussionsas the end oflife approachesSTEP 2STEP 3Assessment,care planningand reviewCoordinationof care‘Effective communicationbetween patients and clinicians isfundamental. We know patientsand their carers value it highly.We also know it is sometimespoor.’Professor Sir Mike RichardsSpecific issues in heart failure The treatment of confirmed heart failurefavours a guideline driven medical model.Clinicians need to explore and address healthand social care issues often more relevant tothe needs of patients and their carers andlook beyond the specific remit of heartfailure24. Clinicians, including heart failure personnel,are reluctant to embark on discussions aboutend of life issues in the face of prognosticuncertainty and a perception of impliedprofessional failure. There may also be a fearof upsetting patients or carers. Prognostic tools (‘trigger tools’) can help toidentify patients who are entering the end oflife phase of their illness. Once this point isreached, the patient should be part of a12STEP 4STEP 5STEP 6Delivery ofhigh qualityservices indifferentsettingsCare in the lastdays of lifeCare afterdeathdiscussion within the MDT to confirm thattreatment has been optimised, to reassessgoals of care and to ensure that informationrelating to a change of emphasis tosymptomatic care is appropriate anddisseminated to all those involved with thepatient. Generic community based palliativecare should be enabled and specialist palliativecare involvement may be helpful. The patientand family should also be informed of theresults of such deliberation and if possiblecontribute to this process with recording oftheir needs and preferences. Patients would prefer doctors to open thisdialogue but this rarely occurs. Few heartfailure specialists have been trained toconduct these difficult conversations. Theperson delegated to discuss end of life carewith the patient should have had this training,be someone familiar to the patient and be in aposition of professional trust. Heart failurenurses may be ideally placed to broach thisdifficult subject in conjunction with the GP. Patients and carers may still have little insightinto the significance and implications of thediagnosis of ‘heart failure’. Others may havebeen informed but prefer not to know. Somemay be disempowered by the highly technicalnature of the assessment and treatment of thecondition. Cognitive impairment is alsocommon in those suffering from heart failure,impacting upon mental capacity25.
End of life care in heart failure: A framework for implementation‘Your symptoms may settle as weadjust the medication. If they donot, you may want to discuss howyou are managing and whatsupport you and your carers mightneed.” “You may want to discussthese issues with me or with theheart failure nurse. perhaps youmight discuss your questions,concerns and priorities with yourfamily.’Key messages for commissioners Service providers should agree locally onprognostic signs / indicators which can beused as a means of identifying which patientsare approaching end of life (see Box 1). Service specification should includeinvestment in communication skills trainingfor heart failure specialists designated toundertake these challenging discussions. Ensure effective mechanisms are in place tofacilitate information exchange across all caresectors.The importance of a MDT approach indeciding when a patient is reaching theend of life was highlighted at an advisorygroup meeting. It is also important toplan ongoing care in this way and it wasproposed that ALL health professionalsinvolved in communicating with patientsor involved with the care of patientsreaching the end of life should be trainedin advanced communication skills.13
End of life care in heart failure: A framework for implementationAssessment, care planningand reviewSTEP 2STEP 1Discussionsas the end oflife approachesSTEP 3Assessment,care planningand reviewCoordinationof careSpecific issues in heart failure In the last year of life there is compression ofillness and people with advanced heart failureoften have multiple crises admissions,frequently with little contact between theadmitting team and the heart failure service. Currently, heart failure care is oftenfragmented with a lack of clarity about whoshould assess, plan and review needs in aholistic way. A MDT based care provides amodel for cross sector collaboration but istime constrained and not universally applied.Specialist palliative care may be involved toolate in this process. Lack of consensus about how to assess thebroader, supportive care needs of heart failurepatients and their informal carers as theseevolve and goals of care change. This impactson anticipatory end of life care planning,including appropriate modification of drugand device therapy, and undermines patientautonomy in maintaining preferences forplace of care and death. About 90% of thelast year of life is spent at home yet 59%of patients die in hospital.14STEP 4STEP 5STEP 6Delivery ofhigh qualityservices indifferentsettingsCare in the lastdays of lifeCare afterdeath To date, the cardiology workforce has notengaged significantly in formal advance careplanning. There is a lack of cohesion between primarycare, secondary care and social care providers. At present, no favoured model of informationrecording or exchange is applicable tomultiple agencies.
End of life care in heart failure: A framework for implementationKey messages for commissioners Vertical integration between community andsecondary care providers might promotebetter care coordination and cost saving. Proactively identifying heart failure patientslikely to be in the last year of life wouldenable such patients and their carers tobenefit from established programmes such asthe Gold Standards Framework and thePreferred Priorities for Care. Advance care planning should be endorsed.People with many symptoms oftenbenefit from a full re-assessment from theGP and district nurse services. Thisincludes checking out the concerns of thepatient and their carers, asking aboutwhat the patient or carer wants or needsin terms of help. Financial and social(practical) helping services, emotionalsupport services may become importantat this point.‘Because your heart failure hasbeen unstable recently, I suspectthat I should be discussing withyour GP how the next period oftime might pan out. Do you haveconcerns or questions about whatthis period of unstable healthcould mean for you?’15
End of life care in heart failure: A framework for implementationCoordination of careSTEP 3STEP 1Discussionsas the end oflife approachesSTEP 2Assessment,care planningand reviewCoordinationof careSpecific issues in heart failure Increasingly, patients with severe heart failureare managed in the community by specialistheart failure nurses, and their input is crucial.They are in the best position to detect earlysigns that the condition is worsening and toact to prevent acute exacerbations. Specialist nurses cannot cover 24/7 and as thecondition deteriorates, more generic out ofhours services provided by community nursesand/or ambulance services may be calledupon. The relationship between theseelements of the service, the patient’s GP andthe hospital services is pivotal. Because a variety of healthcare professionalsmay be involved in an individual patient’s care,it is important that the patient’s care plan,multidisciplinary record, advance care planand any other relevant documentation areavailable and accessible in that patient’shome. Patients with heart failure commonly miss outon the advantages models of carecoordination such as the Gold StandardsFramework provide because they are rarelyidentified as being suitable to be placed on a‘supportive care register’ in primary care.16STEP 4STEP 5STEP 6Delivery ofhigh qualityservices indifferentsettingsCare in the lastdays of lifeCare afterdeathBOX 2A heart failure patient’s wish to die athome may be thwarted by: Insufficient anticipation of expectedsymptoms Uncertain or poorly documentedpreferences and priorities for care A lack of discussion with family andcarers prior to the terminaldeterioration Exhaustion or fear amongst family / carers Hypoxia, leading to confusion anddistress: this can trigger families orhealth professionals to call an ambulance Inadequate collaboration with ‘out ofhours’ medical and nursing services The need for intravenous diuretic therapy. The quality of care available in the home atthis point is central to management ofsymptoms and respecting the wishes of thepatient. When patients with heart failuredeteriorate it is frightening for them and theircarers and they tend to end up in hospital.
End of life care in heart failure: A framework for implementationKey messages for commissioners Appointing a single point of contact tocoordinate care and access support maysignificantly improve care navigation. Established mechanisms for care coordinationat the end of life disproportionately favourcancer patients, but many of the sameprocesses can be adapted for heart failurepatients. Specialist heart failure nurses are in an idealposition to act as care coordin
End of life care in heart failure: A framework for implementation The heart failure disease trajectory Central to commissioning a high quality, cost effective service is a better understanding of the nature of advanced heart failure and, in particular, the end of life phase. As described below, the trajectory of heart