Transcription
REPORT FROMTHE CANADIANCHRONIC DISEASESURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018P R O T E C T I N G A N D E M P O W E R I N G C A N A D I A N S T O I M P R O V E T H E I R H E A LT H
TO PROMOTE AND PROTECT THE HEALTH OF CANADIANS THROUGH LEADERSHIP, PARTNERSHIP,INNOVATION AND ACTION IN PUBLIC HEALTH.—Public Health Agency of CanadaÉgalement disponible en français sous le titre :Rapport du Système canadien de surveillance des maladies chroniques :Les maladies du cœur au Canada, 2018To obtain additional information, please contact:Public Health Agency of CanadaAddress Locator 0900C2Ottawa, ON K1A 0K9Tel.: 613-957-2991Toll free: 1-866-225-0709Fax: 613-941-5366TTY: 1-800-465-7735E-mail: publications@hc-sc.gc.ca Her Majesty the Queen in Right of Canada, as represented by the Minister of Health, 2018Publication date: May 2018This publication may be reproduced for personal or internal use only without permission provided the source is fully acknowledged.Cat.: HP35-85/1-2018E-PDFISBN: 978-0-660-24021-3Pub.: 170307
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018REPORT FROM THE CANADIANCHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018I
IIREPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018TABLE OF CONTENTSEXECUTIVE SUMMARY. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11. INTRODUCTION. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .31.1 GLOBAL BURDEN OF HEART DISEASE. . . . . . . . . . . . . . . . . . . . . . . . . 31.2 DEFINING HEART DISEASE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41.3 STAGES IN THE DEVELOPMENT OF HEART DISEASE. . . . . . . . . . . . . . . . . 41.4 PURPOSE OF THIS REPORT. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52. KEY FINDINGS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .62.1 IMPROVED CARDIOVASCULAR HEALTH. . . . . . . . . . . . . . . . . . . . . . . . 62.2 HEART DISEASE IN MEN AND WOMEN. . . . . . . . . . . . . . . . . . . . . . .202.3 PAN-CANADIAN PERSPECTIVE. . . . . . . . . . . . . . . . . . . . . . . . . . . .373. ISCHEMIC HEART DISEASE AND HEART FAILURE RELATIONSHIP. . . . . . . . . . .433.1 HEART DISEASE RISK FACTORS AND TREATMENTS. . . . . . . . . . . . . . . . .433.2 ISCHEMIC HEART DISEASE AND HEART FAILURE COMORBIDITY. . . . . . . . . .44CLOSING REMARKS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .49APPENDIX A. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .50CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM. . . . . . . . . . . . . . . .50APPENDIX B. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .51HEART DISEASE CASE DEFINITIONS. . . . . . . . . . . . . . . . . . . . . . . . . . .51APPENDIX C. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .52METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .52APPENDIX D. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53LIMITATIONS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53GLOSSARY. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .54ACKNOWLEDGEMENTS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .57BIBLIOGRAPHY. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .60III
IVREPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018EXECUTIVE SUMMARYHEART DISEASESIn Canada, heart disease is the second leading cause of death, after cancer, and accountedfor almost 20% of all deaths in 2012. Also known as ischemic heart disease or coronary heartdisease, heart disease refers to the buildup of plaque in the heart’s arteries that could leadto a heart attack, a stroke or heart failure. Heart disease is the most common type of heartconditions in Canada and other industrialized countries, accounting for almost half of allheart‑disease‑related deaths.PURPOSE OF THIS REPORTThis report is the first publication to include administrative health data from the CanadianChronic Disease Surveillance System to support the national surveillance of ischemic heartdisease and acute myocardial infarction (a subset of ischemic heart disease also known asheart attack) among Canadian adults aged 20 years and older as well as heart failure amongCanadian adults aged 40 years and older. It features the most recent data available from thesurveillance system (fiscal year 2012–2013), as well as trend data spanning over a decade.KEY FINDINGSIn 2012–2013, about 2.4 million (or 1 in 12) Canadian adults aged 20 years and older wereliving with ischemic heart disease, including 578,000 with a history of an acute myocardialinfarction. Another 669,600 (3.6%) Canadians adults aged 40 years and older were living withheart failure. Heart disease outcomes are improving over time. From 2000–2001 to 2012–2013,age-standardized ischemic heart disease and heart failure incidence and all-causemortality rates declined, while the prevalence of both conditions remained relativelystable. Respectively, incidence rates declined by 45% and 35% and all-cause mortalityrates fell by 24% and 26%. A similar pattern was observed for acute myocardial infarction,although the occurrence increased by about 67% over the study period.1
2REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018 Rates of death from any cause are higher among those with a heart disease than thosewithout. Canadian adults with ischemic heart disease (IHD) were three times more likelyto die of any cause compared to those without the disease in a given year. The outcomewas least favorable for younger women and men aged 20 to 39 years old with ischemicheart disease who were about 18 and 11 times more likely to die of any cause, respectively,than individuals of the same age without IHD. Overall, individuals with a history of an acutemyocardial infarction and those with heart failure were four and six times more likely to dieof any cause than those with neither condition in a given year. Heart disease differs by sex. Heart disease appears about 10 years later in women than inmen. In addition, age-standardized prevalence and incidence rates of diagnosed ischemicheart disease and heart failure as well as the occurrence of acute myocardial infarctionwere higher among men than women over the 13-year period. Similarly, age-standardizedall-cause mortality rates were higher in men than women, except for acute myocardialinfarction where women aged 45 to 74 years old were about 30% more likely to die ofany cause than men of the same age in a given year.Although remarkable advancements in the prevention and management of heart diseasehave been made in the last few decades, sustained efforts are needed to further prevent thedevelopment of heart disease risk factors, ensure early detection and treatment, and closethe gap in disease occurrence between women and men. Finally, the absolute number ofpeople living with a heart condition is increasing, thus the need for management andtreatment resources for heart disease will continue to be high.
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20181.INTRODUCTION1.1GLOBAL BURDEN OF HEART DISEASEHeart disease is the leading cause of deathglobally. In 2015, an estimated 8.9 millionpeople died from heart disease, whichrepresent 45% of all non-communicabledisease deaths worldwide.1 In addition,heart disease is the leading cause ofdisability-adjusted life years (DALYs) lostdue to ill-health, disability or early deathworldwide.2In Canada, although major improvements intreatment, disease management and publichealth interventions have been made overthe last few decades, heart disease is thesecond leading cause of death,3 after cancerand a leading cause of hospitalization.4Moreover, in Canada, heart disease is thenumber one cause of years of life lost1 dueto premature mortality and second leadingcause of DALYs lost in 2015.245%of all non-communicabledisease deaths worldwideare due to heart disease8.9 MillionDEATHS GLOBALLYATTRIBUTABLE TOHEART DISEASE3
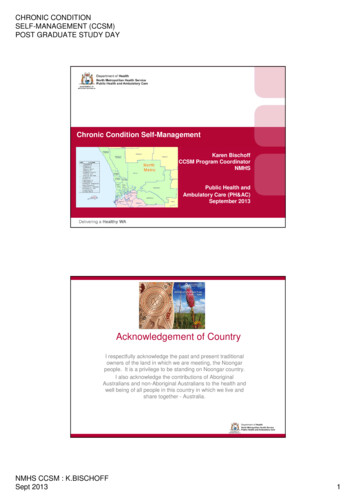
4REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20181.2DEFINING HEART DISEASEAlso known as coronary heart disease or ischemic heart disease (IHD), heart disease is acondition in which the heart muscle is damaged or does not function properly. Plaque(composed of fat, cholesterol, calcium and other substances) builds up on the inner walls ofcoronary arteries and, over time, it can harden or rupture. When plaque hardens, coronaryarteries get narrower and it reduces the flow of blood to the heart muscle which may causechest pain or discomfort, called angina. When plaque ruptures, a blood clot can form in acoronary artery and block blood flow to the heart, causing an acute myocardial infarction(AMI), also known as heart attack. Similarly, a stroke may occur when blood flow to the brainis interrupted or reduced. It happens when a brain blood vessel ruptures or when it is blocked.Heart disease can also lead to heart failure and other types of heart disease, such as cardiacarrhythmias (abnormal heart rhythm).5 Heart failure occurs when the pumping action of theheart cannot provide enough blood to the rest of the body. It results in an accumulation offluid in the body, particularly in the lungs or legs.6 The most common cause of heart failureis damage to the heart muscle as a result of acute myocardial infarction.1.3STAGES IN THE DEVELOPMENT OF HEART DISEASEHeart disease develops over decades. A number of events occur before it progresses toend-stage heart failure. Behavioural risk factors such as unhealthy diet, physical inactivity,smoking, alcohol use and a number of medical risk conditions (e.g. hypertension, diabetes,obesity and high cholesterol) increase a person’s risk of developing heart disease later in life.Without early detection, lifestyle modification and/or treatment, these risk factors maycontribute to heart failure or death as depicted in Figure A below.FIGURE A. Events leading to heart disease progressionAt risk for heart diseaseand heart failure butwithout structural heartdisease† or symptoms ofheart failureStructural heart diseasebut no symptoms ofheart failureStructural heart diseasewith symptoms of heartfailurePeople with:People with:People with: hypertensiondiabetesobesitysmokinghigh cholesterolStructuralheart disease ischemic heartdisease acute myocardialinfarction arrhythmiaDevelopment ofsymptoms ofheart failure known structuralheart disease shortness of breathand fatigue; reducedexercise tolerance end-stage heartdiseaseFigure adapted from Jessup M. et al7 and Dzau VJ et al.8†Structural heart disease refers to a defect or abnormality in the heart’s valves, heart muscle or blood vessels that can be presentat birth (congenital) or acquired later in life.
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20181.4PURPOSE OF THIS REPORTThis is the first report from the Public Health Agency of Canada (PHAC) to includeadministrative health data from the Canadian Chronic Disease Surveillance System (CCDSS)for the national surveillance of heart disease in Canada. It aims to provide a national pictureof the status of heart disease in Canada, in addition to highlighting trends spanning over adecade (2000–2001 to 2012–2013). Using data from the CCDSS, estimates for IHD, as wellas AMI [a subset of IHD] and heart failure are described in this report. The CCDSS is acollaborative network of provincial and territorial chronic disease surveillance systems, ledby PHAC. Technical and methodological notes about the CCDSS as well as definitions usedto identify heart disease cases can be found in Appendices A–D. The data from the CCDSSon IHD, AMI and heart failure, as well as many other chronic conditions can be accessedonline through PHAC’s Public Health Infobase (https://infobase.phac-aspc.gc.ca).5
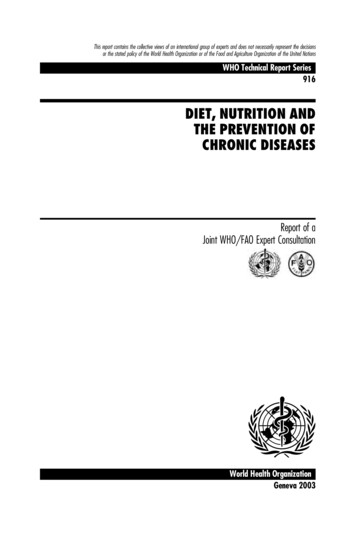
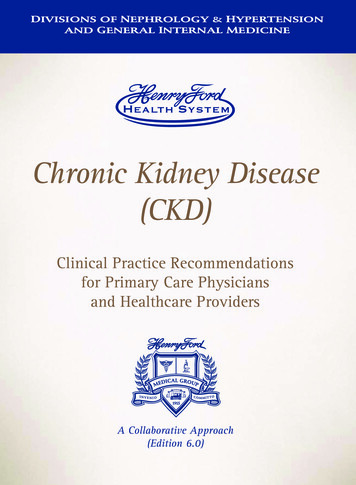
6REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20182.KEY FINDINGS2.1IMPROVED CARDIOVASCULAR HEALTHBased on Canadian Chronic Disease Surveillance System (CCDSS) data from 2000–2001 to2012–2013, a few common trends were observed for ischemic heart disease (IHD), acutemyocardial infarction (AMI) [a subset of IHD] and heart failure. These trends are consistent withthose reported in the Public Health Agency of Canada’s Tracking Heart Disease and Stroke inCanada report from 2009, which indicated that death rates for heart disease have decreaseddramatically from 1969 to 2004.62.1.1Prevalencei The age-standardized prevalence of diagnosed IHD, among individuals aged 20 years andolder, increased from 7.1% to 8.1% between 2000–2001 and 2004–2005 and then stabilizes(Figure 1A). The average annual percent change (AAPC) in prevalence is less than one percentfrom 2000–2001 to 2012–2013. In contrast, the percentage of people with a history of AMIiiincreased from 1.2% in 2000–2001 to 2.0% in 2012–2013, representing an AAPC of 3.7%(Figure 1A). The number of people living with IHD continues to increase over time, from about 1.5 millionin 2000–2001 to 2.4 million in 2012–2013, including about 578,000 with a history of AMI in2012–2013 (Figure 1A). The age-standardized prevalence of heart failure, among individuals aged 40 years and older,remains stable at about 3.5% (Figure 1B). Similar to IHD, the AAPC in heart failure prevalenceis less than one percent from 2000–2001 to 2012–2013. Over the 13-year period, the numberof people living with diagnosed heart failure increased from about 467,700 to 669,600.The number of Canadian adults aged 20 years and older with a history ofheart attack (a subset of heart disease) increased from approximately251,000 to 578,000 between 2000–2001 and 2012–2013.The proportion of Canadians with a history of heart attack increased by67% over the same time period. This increase likely reflects that more andmore Canadians are surviving heart attacks.iCounts and crude prevalence and incidence estimates by sex, age group, year, and province/territory can be accessed onlinethrough the Public Health Infobase: https://infobase.phac-aspc.gc.ca.iiIndividuals aged 20 years and older with a hospital admission including a diagnostic code of AMI or recorded history of AMIwere included. More details are available in Appendix B, Table 1.
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20187FIGURE 1A. Prevalence (%† and number) of diagnosed ischemic heart disease (IHD) andoccurrence (%† and number) of acute myocardial infarction (AMI) among Canadians aged20 years and older, Canada*, 2000–2001 to .81.91.91.91.92.001,526,340 1,644,800 1,747,830 1,839,400 1,920,150 1,996,040 2,065,270 2,125,500 2,182,720 2,234,980 2,288,290 2,336,430 FISCAL YEARIHD PrevalenceAMI Occurrence (IHD subset)†Number of people with IHDNumber of people who had AMI (IHD subset)Age-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.NUMBER OF PEOPLEPREVALENCE OR OCCURRENCE (%)7
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018FIGURE 1B. Age-standardized† prevalence of diagnosed heart failure and number ofpeople with heart failure, among Canadians aged 40 years and older, Canada*, 2000–2001to ,320655,760669,6200FISCAL YEARPrevalence†Number of peopleAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.2.1.2Incidence (new cases) The age-standardized incidence rate of IHD decreased from 12.3 per 1,000 in 2000–2001to 6.8 per 1,000 in 2012–2013, with an AAPC of -4.6%. The age-standardized occurrencerate of a first AMI also declined, from 3.0 per 1,000 in 2000–2001 to 2.2 per 1,000 in2012–2013, with an AAPC of -1.8% (Figure 2A). The number of people newly diagnosedwith IHD declined from about 221,800to 158,700 between 2000–2001 and2012–2013. However, the number ofpeople having a first AMI remainedrelatively stable at about 62,000 peopleannually (Figure 2A). The age-standardized incidence rate ofheart failure declined from 8.1 per 1,000to 5.3 per 1,000 between 2000–2001 and2012–2013, with an AAPC of -3.1%. Overthe same period, the number of peoplenewly diagnosed with heart failure fellfrom about 102,800 to 92,900 individuals(Figure 2B).IHDê 45%AMI(a subset of IHD)ê 17%Heart Failure%ê 35Heart disease incidence ratesdeclined in Canada between2000–2001 and 2012–2013NUMBER OF PEOPLE3PREVALENCE (%)8
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20189FIGURE 2A. Incidence (rates† and number) of diagnosed ischemic heart disease (IHD) andoccurrence (rates† and number) of first acute myocardial infarction (AMI) among Canadiansaged 20 years and older, Canada*, 2000–2001 to ,03061,12061,34063,1900FISCAL YEAR†IHD incidence rateNumber of people with newly diagnosed IHDOccurrence first AMI (IHD subset)Number of people with new AMI (IHD subset)Age-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.NUMBER OF PEOPLEINCIDENCE OR OCCURRENCE RATE (per 1,000)12
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018FIGURE 2B. Age-standardized† incidence rates of diagnosed heart failure and number ofpeople with heart failure, among Canadians aged 40 years and older, Canada*, 2000–2001to L YEARIncidence rate†Number of peopleAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.NUMBER OF PEOPLEINCIDENCE RATE (per 1,000)10
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 20182.1.3All-Cause Mortality Rates The age-standardized all-cause mortality rate among people living withIHD and those with a history of AMI decreased substantially between2000–2001 and 2012–2013, from 22.5 to 17.1 per 1,000 and from 42.2 to27.5 per 1,000, respectively, with corresponding AAPCs of -1.3% and -2.9%(Figure 3A). On the other hand, the absolute number of deaths has increased over time, from about86,300 deaths in 2000–2001 to 112,200 deaths in 2012–2013 in those with diagnosed IHD,including a rise in the number of deaths among those with a history of AMI, from about25,600 deaths to 41,500 deaths (Figure 3A). Overall, all‑cause deaths among those witha history of AMI represented over one third of all deaths in those with IHD. The age-standardized all-cause mortality rate among people living with heart failuredeclined from 78.4 to 57.8 per 1,000 between 2000–2001 and 2012–2013, with an AAPCof -2.5%. The number of people with heart failure who died of any cause increased from67,300 in 2000–2001 to 80,100 in 2012–2013 (Figure 3B).Between 2000–2001 and 2012–2013%ê 24 decreasein the all-cause mortality rate among Canadiansliving with IHD%35decreaseêin the all-cause mortality rate among Canadianswho had an AMI (a subset of IHD)%ê 26 decreasein the all-cause mortality rate among Canadiansliving with heart failure11
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018FIGURE 3A. Age-standardized† all-cause mortality rates and number of deaths amongCanadians aged 20 years and older with diagnosed ischemic heart disease (IHD) and thosewho had an acute myocardial infarction (AMI), Canada*, 2000–2001 to 00FISCAL YEARIHD all-cause mortality rateAMI all-cause mortality rate (IHD subset)†IHD—Number of deathsAMI (IHD subset)—Number of deathsAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.NUMBER OF DEATHSALL-CAUSE MORTALITY RATE (per 1,000)12
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 8075,64078,16077,52080,0500FISCAL YEARAll-cause mortality rate†Number of deathsAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.NUMBER OF DEATHSALL-CAUSE MORTALITY RATE (per 1,000)FIGURE 3B. Age-standardized† all-cause mortality rates and number of deaths amongCanadians aged 40 years and older with diagnosed heart failure, Canada*, 2000–2001to 2012–2013
14REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018CANADIAN ADULTS WITH HEART DISEASE HAVE HIGHER MORTALITY RATES COMPAREDTO THOSE WITHOUT HEART DISEASE Compared to those without IHD, AMI or heart failure, individuals with the diseaseof interest are more likely to die of any cause in a given year. Age-standardized all-cause mortality rates were almost three times higher, on average,among Canadian adults with diagnosed IHD compared to those without in a givenyear (Figure 4A). Compared to those without a prior history of AMI, those with a history of AMI were aboutfour times more likely to die of any cause in 2012–2013 (Figure 4B). The gap betweenthose with and without a history of AMI has reduced over time, since the rate ratio wasas high as 4.7 in the early 2000s. In a given year, Canadians aged 40 years and older with diagnosed heart failure were,on average, six times more likely to die of any cause than those without heart failure(Figure 4C).Heart Failure6XAMI(subset of IHD)4XIHD3XIn any given year, Canadians withheart disease are more likely todie of any cause than thosewithout heart disease
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2.72.82.82.72.82.80FISCAL YEARWith IHD†Without IHDRate ratioAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.RATE RATIO (WITH VS. WITHOUT IHD)ALL-CAUSE MORTALITY RATE (per 1,000)FIGURE 4A. Age-standardized† all-cause mortality rates and rate ratios among Canadians aged20 years and older with and without ischemic heart disease (IHD), Canada*, 2000–2001 to2012–2013
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018FIGURE 4B. Age-standardized† all-cause mortality rates and rate ratios among Canadiansaged 20 years and older with and without acute myocardial infarction (AMI), Canada*,2000–2001 to 2012–2013505454043530325202RATE RATIO (WITH VS. WITHOUT AMI)ALL-CAUSE MORTALITY RATE (per 3.73.83.73.80FISCAL YEARWith AMI (IHD subset)†Without AMIRate ratioAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.
REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018FIGURE 4C. Age-standardized† all-cause mortality rates and rate ratios among Canadiansaged 40 years and older with and without heart failure, Canada*, 2000–2001 to 2012–201310909808ALL-CAUSE MORTALITY RATE (per 1,000)7606505404303202100RATE RATIO (WITH VS. WITHOUT HEART 36.26.26.26.26.20FISCAL YEARWith heart failure†Without heart failureRate ratioAge-standardized to the 2011 Canadian population.* Data from Yukon were not available.NOTES: The 95% confidence interval shows an estimated range of values which is likely to include the true value 19 times out of 20.SOURCE: Public Health Agency of Canada, using Canadian Chronic Disease Surveillance System data files contributed byprovinces and territories, May 2016.17
18REPORT FROM THE CANADIAN CHRONIC DISEASE SURVEILLANCE SYSTEM:HEART DISEASE IN CANADA, 2018MULTIPLE FACTORS EXPLAIN IMPROVED CARDIOVASCULAR HEALTHBetween 2000–2001 and 2012–2013, age-standardized incidence (occurrence in the caseof AMI) and all-cause mortality rates have declined greatly among those with IHD and heartfailure and those having had an AMI.Using a validated mortality model, Ford E. et al. quantified the respective contribution of majorrisk factors and medical treatments to the decline in mortality from coronary heart diseasebetween 1980 and 2000, among American adults aged 25 to 84 years old. About 47% of thisdecline in mortality was attributed to treatments, including medications or rehabilitation, afteran AMI. Approximately 44% of the decline was also attributed to changes in risk factors, namelydecreases in total cholesterol, systolic blood pressure and smoking.9 Similar studies conductedin Western countries found that trends in risk factors explained 44% to 76% of the declinewhereas treatments explained 23% to 47%.10Use of aspirin, antihypertensive medications and cholesterol-lowering medications (such asstatins) reduce the risk of developing heart disease.11,12 In addition, the effectiveness of cardiacdrugs to relieve symptoms and prevent recurrent AMI and premature death has been welldocumented.13–15 Improvements in cardiac care and use of surgical treatments, mainly coronaryartery bypass surgery, has also been shown to reduce all-cause mortality rates and ischemicheart disease events.16In the INTERHEART study, it was found that nine risk factors (smoking, high cholesterol,hypertensio
Heart disease appears about 10 years later in women than in men. In addition, age-standardized prevalence and incidence rates of diagnosed ischemic heart disease and heart failure as well as the occurrence of acute myocardial infarction were higher among men than women over the 13-year period. Similarly, age-standardized