Transcription
www.baccn.org.ukBACCNStandards for NurseStaffing in Critical CareBritish Association ofCritical Care NursesCritical Care NetworksNational Nurse LeadsRoyal College of NursingCritical Care & In-flight Forum
ContentsIndex of tables4Produced by104Acknowledgements5Executive SummaryTable 1: National Codes: Departmentof Health Critical Care InformationAdvisory Group January 20066Standards for Nurse Staffingin Critical Care Units11Table 2: Definition of A Critical Care Nurse147Introduction8BackgroundTable 3: Systematic Literature Reviewsinto Organisational Factors andCritical Care Patient Outcomes.9Definition of critical care1611Definition of critical care nurseTable 4: Proposed Quality MetricMeasures of Nursing Care Relatingto Outcomes in Critical Care1612Review of the literature1915Developing nurses staffing standardsand policy related to quality outcomesTable 5: Disconnection fromVentilation and Competence1916Reduction in the incidence ofhealthcare associated infections(HCAI) and staffing levelsTable 6: Disconnection from MechanicalVentilation and Vigilance22Table 8: Outline curriculum for critical care22Artificial ventilation is associatedwith increased critical carecosts and adverse eventsTable 7: Educational principles/recommendations23Table 9: Educational principles for critical care26Table 10: Current FundingSystems for Critical Care28Table 11: Key Points Relevant to theCritical Care Minimum Data Set (CCMDS)1718Protocol based care improves outcomes18Team working and improved communicationis associated with risk avoidance19Legal issues relevant to staffing in critical care20Health care assistants and assistantpractitioners in critical care20Administrative support staff in critical care20Severity scoring systems andnursing workload21Association of UK university hospitals(AUKUH) acuity/dependency tool21Education for critical care nurses26Building critical care facilities26Commissioning and fundingof critical care services28Same sex accommodation incritical care settings29Technology and critical care : baccn@baccn.orgT: 0844 800 8843
Produced byAcknowledgementsKate Bray: Professional Advisor BACCN NationalBoard, Benchmark Communications14 Blandford SquareNewcastle upon Tyne, NE1 4HZ UKbaccn@baccn.orgWorld Federation of Critical CareNurses: http://en.wfccn.org/European Federation of Critical Care NursingAssociations: http://www.efccna.org/Ian Wren: (BACCN) Acute Care ClinicalProgramme Manager, PlymouthHospitals NHS Trust Plymouth, UKPublished in September 2009Copyright of these Staffing Standards is jointly ownedby the British Association of Critical Care Nurses, TheCritical Care Networks National Nurse Leads, andthe Royal College of Nursing Critical Care Forum.Andrea Baldwin: Senior Nurse/Chair Critical CareNetworks National Nurse Leads Group (CC3N)Service Improvement Lead Nurse: Lancashireand South Cumbria Critical Care NetworkUna St Ledger: BACCN Northern IrelandCommittee Member / Chair Education SubGroup, Critical Care Network Northern Ireland(CCaNNI) / Nursing Development Lead, CriticalCare, Belfast Health &Social Care Trust, UKVanessa Gibson: Professional Advisor BACCNNational Board Senior Lecturer Critical CareNorthumbria University Newcastle UKSheila Goodman: RCN Critical Care & In-FlightForum Steering Committee Member, SisterCritical Care Services West Suffolk HospitalDominic Walsh: RCN Critical Care & InFlight Forum Steering Committee Member,Charge Nurse Royal Free Hospital.For further information contact via E a.baldwin@lthtr.nhs.uk www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
Executive SummaryThe inception of intensive care and subsequentlycritical care (DOH 2002) started in 1952 inDenmark using techniques from the operatingtheatre whereby positive pressure ventilationwas used to support patients with respiratoryfailure. As the specialty developed within theUnited Kingdom (UK), the original ‘gold standard’for nurse staffing in intensive care units wasset at a ratio of one nurse for each patient in1967. which reflected the intensive supportand nursing care such patients required.In recent years this standard has been challengedfor a variety of reasons that include the highcost of staffing associated with critical illnessmanagement, and the suggestion that nursing staffin critical care units need to work more flexibly.The critical care environment has changedconsiderably since the 1960’s and the specialityof critical care has, as a consequence grown. Thishas been in response to advances in technology,surgical and medical techniques and procedures,and also managing an increasing older patientpopulation with complex diagnoses and comorbidities. This has lead to changes in staffingand the nursing team in a critical care unit cannow typically comprise of registered nurses,advanced critical care practitioners, critical careoutreach nurses, and practice developmentnurses, who are supported by assistant criticalcare practitioners and health care assistants.critical care and as such has been highlighted inthis document. These include infection control,size and geographical layout, and number ofbeds in a unit, case mix, safety in relation toventilated patients, mixed sex accommodationneeds, and the individual experience of eachnurse. Critical care nurses, unit managers, andcommissioners, need to take account of allthese variables related to an individual unit,in addition to the skill mix, experience andcompetence of nursing staff available.With appropriate administrative and technologicalsupport, critical care nurses need to embracethe necessary data collection processes nowrequired within this specialty. They also needto be proactive in adopting, contributing to,and developing team focused evidence basedprotocols, in order to improve outcomes forpatients and their families. The future challengefor critical care nurses is to develop and measurethe contribution of quality metrics, which reflectthe effectiveness, and safety of nursing inputfor critical care patients. In doing so they willcontribute to the body of evidence to support andinform relevant nurse-patient ratios in critical care.Tracy Pilcher, Chair, British Associationof Critical Care NursesAndrea Baldwin, Chair, Critical CareNetworks National Nurse leadsRachel Binks, Chair, Royal college ofNursing Critical Care & In-flight ForumThe UK professional critical care nursingorganisations have in the past developed guidancefor critical care staffing, in order to assist nurses inmaking informed decisions with relation to staffingunits; and this inaugural document representsthe first occasion when all three UK ProfessionalCritical Care Nursing associations have workedtogether to produce Standards for Nurse Staffingin Critical Care. These standards have evolved fromprevious work and are endorsed by the BACCN,CC3N, and the RCN Critical Care & In flight Forum.These standards reflects the emerging bodyof evidence, that supports the higher ratio ofnursing staff required to deliver safe and effective www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
Standards for Nurse Staffing in Critical Care Units Determined By:The British Associationof Critical Care NursesThe Critical Care NetworksNational Nurse Leads1.Every patient in a Critical Care Unitmust have immediate access to aregistered nurse with a post registrationqualification in this specific speciality2.Ventilated patients should have aminimum of one nurse to one patient3.The nurse patient ratio within any Critical CareUnit should not go below 1 nurse to 2 patients4.The level of care needs required byeach patient should equate to the skillsand knowledge of the registered nursedelivering and/or supervising that care5.1.Critical Care Units should employ flexibleworking patterns as determined by unitsize, activity, case mix and the fluctuatinglevels of care for each patient, to ensurepatient safety and care delivery6.A supernumerary clinical co-ordinator, whois a senior critical care qualified nurse willbe required for larger and geographicallydiverse units of more than 6 beds. Theclinical co-ordinator’s role is to ensureeffective, safe and appropriate care isdelivered each shift, by managing andsupporting staff and patients, and actingas a communicator and liaison betweenthe rest of the multi-disciplinary team.7.Royal College of NursingCritical Care & In-flight Forum8.On-going education for all nursing staffworking in critical care is of principalimportance to ensure knowledgeableand competent staff care for patients.Clinical Educator posts should beutilised to support this practice.9.Health Care Assistants (HCAs) have a key rolein assisting registered nurses in deliveringdirect patient care and in maintaining patientsafety. These roles should be developed tomeet the demands of patients and of theunit. However, the registered nurse remainsresponsible for the assessment, planning,delivery and evaluation of patient care.10. The Assistant Practitioners (APs) role inCritical Care can provide direct patient careunder the indirect supervision of a registerednurse, who will remain responsible for theassessment, planning and evaluation ofpatient care. The effectiveness of the role ofAssistant Practitioners in Critical Care Unitsrequires further evaluation and research.11. Administrative staff should be employed toensure registered nurses are free to give directpatient care, and to support the critical careunits and staff with essential data collection.12. Critical Care nurses should be proactivein the development of multi-professionalteam working to optimise quality patientcare and ensure a quality service.The layout of beds and use of side wardsin a Critical Care Unit must be takeninto account when setting staffinglevels to ensure safe patient care. www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
IntroductionThe British Association of Critical Care Nurses(BACCN), Critical Care Networks National NurseLeads (CC3N) and the Royal College of Nursing(RCN) Critical Care & In-flight Forum have workedtogether to produce contemporary standardsfor nurse staffing in critical care. The standardsare a review of past recommendations and takeinto account changes in practice, and reflect thechallenges ahead. They have been developed inorder to support healthcare organisations who arecommitted to providing safe critical care services,to the most acutely ill patients in their care.These standards have been developed as areference for nursing staff in critical care, managersand commissioners associated with critical care,in order to provide and support safe patient care,focused upon quality, and the desired patientoutcomes. The standards should help inform theworkforce development programme necessary forthe continued evolution of critical care services.The following information is presented as evidenceto support the standards determined by theBACCN, CC3N, and the RCN Critical Care & In-flightForum. These standards have been developedfor critical care nurses in the United Kingdom.It is acknowledged that in Wales, Scotland andNorthern Ireland there may be differing healthpolicy specific to these areas, however theprinciples are transferable to all critical care units. www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
Background(Audit Commission 1999). The Audit Commissionand the strategic framework documents whichfollowed (DoH 2000, DoH 2001, DoH 2005) assertthat nurse staffing for critical care patients neededto be developed more flexibly, with a move awayfrom the rigid one to one nurse patient ratiotraditionally used in intensive care. Nurses’ payaccounts for up to 28 per cent of acute trusts’total expenditure and is the biggest single itemof hospital expenditure (Audit Commission2009). This recent work by the Audit Commissiondemonstrated that in general wards costs stillvaried profoundly across the UK, and mirrored thefindings found by the Audit Commission Reportinto Critical Care in 1999 where it was reportedthat the nurse staffing costs varied widely. Atthe extreme some unit’s costs were twice thatof a similar sized unit (Audit Commission 1999).Such a variance in nurse staffing costs haverequired critical care nurses to be able to evaluateand justify decisions related to the high nursepatient staffing ratios in critical care units.The inception of intensive care and consequentlycritical care (DOH 2000) started in 1952 inDenmark using techniques from the operatingtheatre whereby positive pressure ventilation isused to support patients with respiratory failure.Prior to this patients with respiratory failure weresupported using negative pressure ventilationusing ‘iron lungs’ with limited success. (IntensiveCare Society 2003). The speciality of critical carehas since grown in response to advances intechnology, and improved surgical and medicaltechniques and procedures. Life expectancy hasincreased, and health care providers are nowcaring for an increasingly ageing population,often with complex underlying conditions. Withinthe UK, the notion of centralising patients whorequired ventilation and increased observationin specialised units emerged in the early 1960’s.In 1967 the gold standard for nurse staffing inintensive care units was set at a ratio of one nursefor each patient (British Medical Association1967). Subsequent documents reinforced thisstandard, suggesting that a ratio of one nurse perbed equated to 7.0 nurses per bed to ensure allbeds could be open (Association of Anaesthetists1988, Intensive Care Society 1997, RCN 2003) Ascritical care medicine progressed intermediatehigh dependency units (HDU’s) developed andthe ratio of nurses per patient was establishedat two patients to one nurse (DoH 1996) .The critical care nursing professional organisationshave previously developed guidance forcritical care staffing, in order to assist nursesin making informed decisions in relation tostaffing units (BACCN 2001, BACCN 2005, RCN2003). This standard evolves from previouswork, and is endorsed by the BACCN, CC3N,and the RCN Critical Care & In-flight Forum.Critical Care is considered a low volume, high costspeciality caring for the sickest patients in an acutehospital. In response to the growing pressure forcritical care beds the Audit Commission examinedthe service in England and Wales, culminating inthe most comprehensive examination of criticalcare since its inception (Audit Commission1999). This report demonstrated the differencein nurse staffing numbers, grade and skill mixacross units, and reported significant variation innumbers of nurses employed and the subsequentcosts associated with this. Staff acknowledgedthat at times a ventilated sedated patient in anintensive care unit may require less registerednursing input than the agitated and confusedself-ventilating patient in a high dependency unit www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
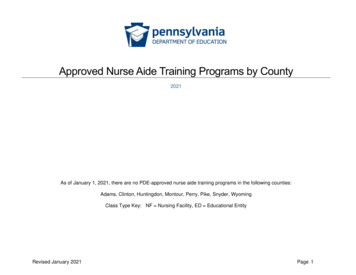
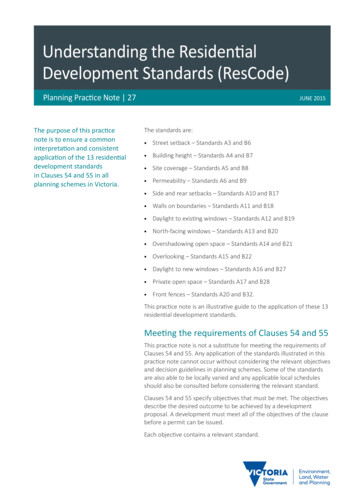
Definition of critical careThe philosophy of critical care (DoH 2000, ICS 2009)embraces a hospital wide perspective, with a focusupon levels of care from level 0 to 3 that is requiredby patients based upon their severity of illness,and regardless of their location . This seamlessapproach encompasses the needs of patients atrisk of critical illness, and also patients recoveringfrom critical illness (DoH 2000). Accordingly thesepatients may be managed in a variety of facilitiessuch as a general ward, an HDU or an intensivecare unit (ICU) depending upon where their needscan be best met, with the support of the multiprofessional team (DoH 2000, RCN, 2003, ICS 2009).For the purpose of this standard the term‘critical care’ will refer to the actual facilities ordiscrete units within a hospital where adultcritical care services are provided. A CriticalCare Unit (CCU) is an umbrella term for an HDUor an ICU, or indeed a unit combining boththese services. Patients requiring level 2 careare usually managed in an HDU whilst thesickest patients requiring level 3 care, are caredfor in an ICU (Mackenzie 2004, ICS 2009).ICU manages patients with potentially reversibleconditions who can benefit from more detailedobservation and invasive treatment thancan safely be provided on general wards orhigh dependency areas. ICU is appropriatefor patients requiring advanced respiratorysupport alone or support of two or morefailing organ systems. ICU offers facilities forthe diagnosis, prevention and treatment ofmultiple organ failure (DOH 1996, ICS 2009).Critical Care Units may be general, mixedspeciality or speciality units (Audit Commission1999). For the purpose of these standards thelevels defined for adult critical care relate to theIntensive Care Society Standards and Guidelinesfor Levels of Critical Care for Adult Patients.The Critical Care Stakeholders Forum, and theDepartment of Health through the CriticalCare Information Advisory Group (CCIAG) alsosupport the standards (ICS 2009). The Codesassigned by CCIAG for the different types ofcritical care specialities are shown in Table 1.HDU provides an intermediate level of carebetween that which is available on a generalward and that on an ICU. Detailed monitoringand intervention is provided to patients withor at risk of developing single organ failure,with the exception of those needing advancedrespiratory support. HDU is also appropriate forpatients who will benefit from extended postoperative care, following major or complicatedsurgery. It can also serve as a ‘step down unit’ forpatients who no longer require intensive carebut who are not yet well enough to be returnedto a general ward (DoH 1996, ICS 2009). www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
National Codes: Department of Health Critical Care Information Advisory Group January 2006Table 101General Intensive Care Unit; adult intensive care, including wards labelled assurgical or medical ICU, but excluding the specialised units identified below.General Intensive Care Units may provide a mixture of HDU and ICU level care02Cardiothoracic Intensive Care Unit; this includes those unitslabelled as separate cardiac or thoracic units03Liver Intensive Care Unit04Neurological Intensive Care Unit05High Dependency Unit09Cardiac Care Unit; otherwise referred to as a Coronary Care Unit10Combined High Dependency and Coronary Care Unit; the beds andstaff for the two units are geographically in the same area11Combined Coronary and Intensive Care Unit; the beds and stafffor the two units are geographically in the same area12Combined High Dependency and Intensive Care Unit; the beds andstaff for the two units are geographically in the same area13Post Operative Recovery Unit; this includes a theatre recovery area14Spinal Injury Intensive Care Unit; this is a unit designated forcritical care rather than a spinal injury ward15Burns Critical Care Unit; this includes all special care burns facilitiesother than short term post-operative care areas16Renal Unit; this includes an in-patient kidney dialysis unit, butexcludes general nephrology or urology wards10www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
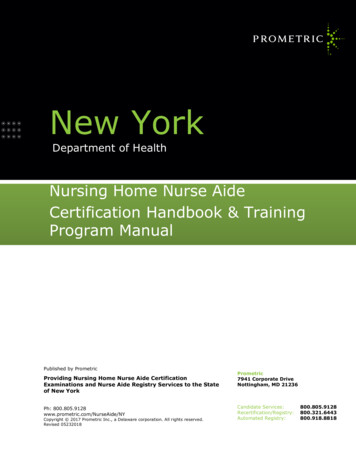
Definition of critical care nurseTable 2The World Federation of Critical Care Nursesprovides a universal definition, which is applicableto critical care in the UK. (Table 2). The skills andknowledge of a critical care nurse are appliedacross the domains of early recognition andintervention, risk management, recovery andrehabilitation in the care of critically ill patients(Ontario Critical Care Nurse Training Standards2005). When survival is not possible the nursesupports the patient and family through theprocess of dying and early bereavement (DoH,2001). A proficient critical care nurse utilises:advanced problem solving, decision makingand communication skills to provide proactive,safe and effective care when undertakingcontinuous complex monitoring and assessment,administering, co-ordinating and evaluatinghigh-intensity therapies, responding promptly tosudden changes in a patient’s condition and inproviding information and emotional support topatients and relatives (ACCCN 2002, RCN 2003).Definition of A Critical Care NurseWorld Federation of Critical Care Nurses (2005)A critical care nurse is a registered practitionerwho enhances the delivery of comprehensivepatient centred care, for acutely ill patientswho require complex interventions in a highlytechnical environment; bringing to the patientcare team a unique combination of knowledgeand skills. The roles of critical care nurses areessential to the multidisciplinary team who areneeded to provide their expertise when caringfor patients and their relatives (WFCCN 2005).Critical care nurses make a significant contributionto the development of the evidence base forcritical care nursing practice. Thus enhancing thequality and experience of patient care, throughinvolvement in professional activities such as, thedevelopment of self and others, data collection,audit, service improvement and research anddevelopment initiatives (DoH 2000; DoH 2001).Critical Care nursing is a dynamic speciality,which positively and proactively respondsto meet the ever changing, complex andchallenging demands of the critically illpopulation and the overall healthcare system.This has resulted in the development of adiverse range of nursing roles, such as thebedside staff nurse, nurse manager, advancedpractitioner, nurse educator, nurse researcher,critical care outreach nurse and consultantnurse. These roles also present opportunitiesfor the development and career progressionof critical care nurses (DoH 2001, DoH 2008).11www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
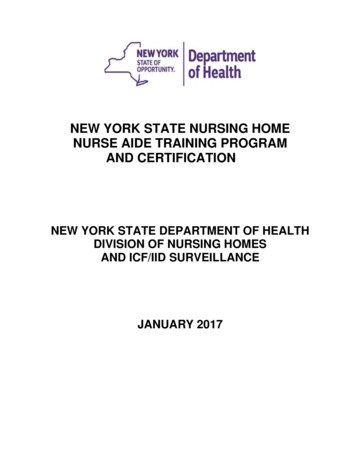
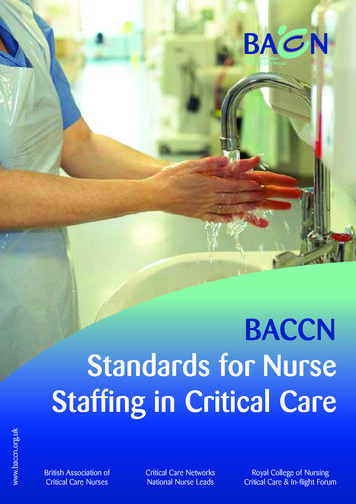
Review of the literatureMethodologyIn order to systematically gather evidenceand facilitate the development of the standardstatement, a number of bibliographic databaseswere searched. To further focus the scope ofthe search, parameters were also identifiedand included restricting papers to the Englishlanguage, human subjects, and papers publishedsince 2003. This was intentional to build upon thelast comprehensive and significant review of theliterature related to staffing in critical care 1990– 2003 (Coombs and Lattimer 2007). Databasessearched were Medline, CINAHL, Cochranedatabase, OVID, Blackwell Scientific, Kings Fund,Department of Health, and the National ResearchRegister. The following search terms were used: Critical care nursing Nursing Nurse staffing Skill mix Adverse events Health care assistants and critical care Length of stay Critical care Intensive care Technology Infection controlThe terms were also combined to further extendthe range of the search. Databases of notable peerreviewed journals were also searched for scientificand non-scientific papers relating to critical careand nursing. To encompass all other aspects ofevidence and information related to nurse staffingin critical care searches were also carried out viathe internet, RCN legal teams, and the NationalPatient Safety Agency (NPSA). Information fromthe expert group of contemporary knowledgeand information related to policy and recentinnovations in critical care were also included.factors, contributed positively or negatively topatient outcomes in critical care settings. Fromthis, approximately 250 abstracts or full textarticles were reviewed. Further review of thesearticles yielded six quality reviews of studiesrelated to staffing in critical care, which could helpin developing staffing standards (Table 3). Theliterature search was not confined to the UnitedKingdom; however international evidence must beinterpreted with caution, in relation to critical carein the NHS and the UK. Critical Care units in the UKfunction differently to other countries, for examplemedical staff and support staff such as respiratorytechnicians are often greater in number in othercountries than in UK units. (Wunsch and Anguset al 2008, BACCN 2005). It is recognised thatnursing roles in critical care in the UK are distinctfrom other countries, as nurses have increasedresponsibility for the management of patientcare and organisation of the unit (RCN 1997).Developing an understanding of the uniquecontribution that nurses make to patient outcomeswithin critical care has been the source of manystudies. However to date, there appears onlylimited definitive work linking nursing alone, topositive or negative patient outcomes withincritical care. Where evidence does exist, thereappears difficulty in extrapolating the resultsto a general population of critical care patientsand environments. The literature on occasionsgives conflicting views regarding some outcomemeasures. Such conclusions are also supportedwithin several notable systematic reviews thathave sought to explore causal links betweenorganisational factors including nursing, andpatient outcomes in critical care (Table 3).West et al (2009) in the most recent review ofresearch evidence related to nurse staffingin critical care, emphasise the need forfurther research and offers the followinghypothesis to be tested in future research:For the literature search approximately 3000entries were reviewed, dating from 1st January2003 to present date. Within the search, entrieswere screened for relevance to critical care andnursing, and in particular for outcomes suggestingthat the nursing contribution to organisational“overwork and staff shortages will interferewith task performance, including surveillance,monitoring, early detection of adverse eventsand preventative measures e.g., hand washing,pulmonary hygiene, early ambulation”.12www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
West et al (2009) also found that study designincluding sample size and single versus multi unitreviews, as well as the statistical methodologyused, leads to difficulty in interpreting some ofthe findings when studying adverse outcomesin critical care. Other review authors commentupon the predominance of observational studiesand a lack of robust clinical trials focussing uponestablishing causal relationships. More recentresearch related to critical care suggests that nursestaffing needs to be based on patient acuity ratherthan an absolute number of patients (Kiekkas et al2008). It also demonstrates that a greater numberof registered nurses is associated with improvedpatient safety and efficiency (Thungjaroenkulet al 2008). Pronovost et al (2002) suggest thatpractical and ethical considerations may be aninsurmountable barrier to conducting clinical trialsinto identifying optimum organisational factors;this may include nursing and nursing skill mix.13www.baccn.org.ukE: baccn@baccn.orgT: 0844 800 8843
14200920072006200520022001West E et alCoombs andLattimerNumataY et alCarayonP andGurses MP*PronovostPJ et alCarmelS, andRowan KOrganisation of intensivecare (including nursing).Relationship betweenphysician staffing andpatient outcomes in ICU.Identification of humanfactors within nursing activity,which impact upon patientsafety and quality of care.Staffing levels andhospital mortalityLiterature review of Safety,effectiveness and of organisingcare for critically ill patients:Identification of empirical evidencelinking nursing resources topatient outcomes. Frameworkto guide further researchFocusOrganisational factors may impact uponmortality after case mix adjustmentIncreased numbers of intensivists inthe ICU led to significant reductions inICU, and hospital mortality and LOS.2763Some causation possible in relationto unit, job, patient, and situation.No clear association identifiedbetween hospital mortalityand low nursing numbersLimited evidence for the safety, effectivenessand cost effectiveness for differing modelsof organising care for the critically ill.Some evidence exists linking patientoutcomes, safety and ICU staffing. Howevergeneralisation remains problematical andwould benefit from further research.Conclusion2295815Number ofarticles infinal review.* Whilst the results from this review were focussed upon medical staffing, it is felt important to include as an example of areview into organisational factors that did show a positive correlation between outcome and staffing.DateAuthor(s)Table 3Systematic Literature Reviews into Organisational Factors and Critical Care Patient Outcomes.Research into the effects ofmultidisciplinary staffingmodels on patient outcomesshould be a high priority.Four aspects of nursing activityrelated to patient safety identified;the unit, job, patient and situationwould benefit from further research.Variable confounding factors.Hospital mortality may lacksensitivity in detecting negativeoutcomes associated withlow staffing numbers.Some correlation between nursestaffing levels in intensive care andincidence of adverse events. Literatureadopts a uni professional bias, moreresearch is required on multi disciplinaryteam working, the organisation of care,and long term outcomes of care.Studies vary in quality, which mayaffect interpretation of results.Comments by author(s)
Developing nurses staffing standardsand policy related to quality outcomesto the consequences of nursing and organisationalfactors. Adverse outcomes have been describedpreviously as including a ‘failure to rescue’ (Silberet al. 1992). Utilising this theme Ball and McElligot(2003) sought to move away from evaluatingpatient outcomes related to just nursing numbers.This study examined the difference nurses madeto the recovery of critical care patients, and thenurses’ ability to prevent patient deterioration.The literature review was attempting to identifyany positive or negative outcomes associatedwith the nursing resource alone. In relation topatient outcomes, there are different viewpointsthat measure negative and positive outcomes.For example, patients may see dignity, survivaland no infections as key quality outcomes,among others. However nurses may perceiveoutcomes such as pressure ulcer acquisition,less adverse incidents (minor to major) andattention to the fundamentals of care as alsoimportant. Managers may
May 05, 2009 · The UK professional critical care nursing organisations have in the past developed guidance for critical care staffing, in order to assist nurses in making informed decisions with relation to staffing units; and this inaugural document represents the first occasion when all three UK Professional