Transcription
The Anatomy ofLocal Anesthesia:The MaxillaUniversity of Detroit Mercy DentalSchoolFebruary 13, 2013Ronald P Morris, DDS
We have to startsomewhere. Let’s startwithPulpal Anesthesia ofMaxilla
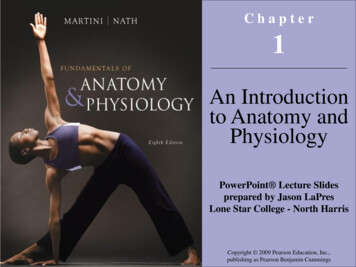
Infraorbital nerveMaxillary division oftrigeminal nerve. Its majorbranch is infraorbital (on thefloor of the orbit).
Netter 2nd 1
Maxillary Pulpal Innervation From the groove and canal,branches come down thewall of the maxillary sinus,to innervate the upper teeth.These are the nerves that weare concerned with, in pulpalanesthesia of the maxillaryteeth.
Branches of Infraorbital Nerve During its coursethrough the floor ofthe orbit, theinfraorbital nerve,gives off branches.We give themthese names:– middle superioralveolar nerve(MSA)– anteriorsuperioralveolar nerve(ASA)InfraorbitalNerveASAMSA
Posterior Superior AlveolarNerve (PSA)Posteriorsuperioralveolar nerveis a littledifferent.ASAPSAMSA
Superior Alveolar Plexus All three nervebranches(ASA, MSA,PSA) form adental plexus(a meshworkof nerves)which, in turn,innervate thepulps of themaxillaryteeth.ASAPSADentalPlexusMSA
To get goodanesthesia, theobject is to getanestheticsolution incontact with thenervesomewherebetween the sitewe’reanesthetizing,and the brain.
Infiltration oftooth # 7 willanesthetize otherstructures in thevicinity: # 8, andpossibly # 6.Note:unfortunately,this labialinfiltrationinjection will notanesthetize thepalatal tissue
Infiltrating Tooth # 7
1.RETRACT LIKE A DENTIST2.GIVE YOURSELF GOODVISIBILITY3.CREATE A SPACE FORYOUR ANESTHETIC
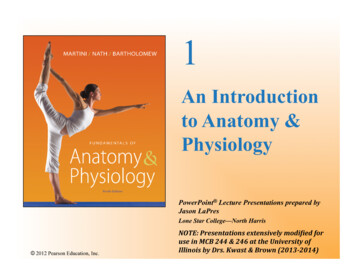
Infraorbital Nerve Block If the operator injectssome anestheticsolution such that itenters the infraorbitalforamen. Theanesthetic will travel upthe infraorbital canal farenough to reach theASA before it branchesfrom the nerve
We can.ASAPSAPath ofAnestheticMSA
Note the location of infraorbitalforamen
Easiest way to infraorbitalforamen: follow the long axisof the first premolar tooth.Penetrate the mucosa and gohalf the length of a shortneedle.
If the infraorbital nerve isanesthetized, its two mainbranches will also beanesthetized.ASAMSA
Fehr 2nd 232
Anesthetizing the PSAAnatomical ReferencesPSA Nerve Block: The posteriorsuperior alveolar(PSA) nerveenters thebackside of themaxillarytuberosity. Thespot where itenters appearsas a rough areaon a skull.
Area affected by PSA BlockFehr 2nd 225
How is This BlockAccomplished? The maxillary tuberosity is easily palpated. The anesthetic needle is inserteddiagonally, (upward, inward & backward),allowing the needle tip to approach theposterior surface of the maxillarytuberosity.
“Roof” of vestibule“Posterior Wall” ofvestibuleThe operatormust swingthe barrel ofthe syringefartherlaterally thanshe wants to.Injection siteis the“corner”where the“roof” of thevestibulemeets the“posteriorwall” of thevestibule.
Be sure topoint theneedle farenoughposteriorly to“get aroundthe corner”behind themaxillarytuberosity.
Palatal Soft Tissue The palate isinnervated by nervesentering at both theback of the palate,and the front of thepalate. There is a great dealof overlap betweenthe two sources ofinnervation.NasopalatineNerveGreater PalatineNerveNote that overlap of these two sourcesoccurs in the canine region.
McM H&N 3rd 257
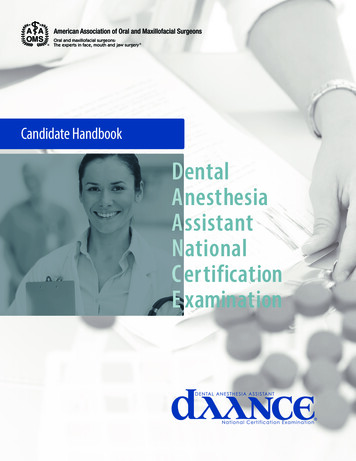
Note the distribution of the Greater Palatine Nerve
This injection is placedwhere the “roof” of thepalate meets the “wall”of the palate, at the levelof the second or thirdmolar.Palpation will reveal a“soft spot” in this area,which is the injectionsite.Greater palatinenerve injection
Injection site forgreater palatinenerve block:Where the “roof” ofthe palate meets the“wall” of the palate,just lingual to themaxillary secondmolar tooth.roofwall
Even in infiltrating, it’sbest to inject into thecorner between thewall and roof of thepalate.The corner
The nasopalatine nerve blockMcM H&N 3rd 257
The Anterior Middle SuperiorAlveolar (AMSA) Injection A new, single-site palatal injection Anesthetizes from second premolar tocentral incisor, palatal and pulpal No collateral numbness to patient’s lip andface Excellent for operative procedures whereposition of smile line is important.
Injection is made palatal tomaxillary first premolar, wherethe “roof” of the palate meetsthe “wall”.
Note the porosity of the palatalbone in that areaRohen 4th 50
AMSA injection will give palatal softtissue anesthesia, and pulpalanesthesia to premolars and anteriorteeth. It will not anesthetize buccal or labialsoft tissue. This can be advantageous when thenatural “lip line” is important.
Maxillary Division Block
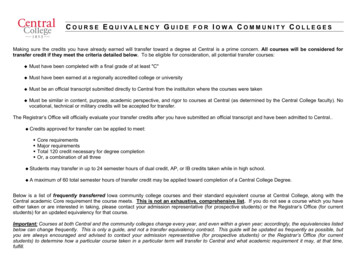
Greater palatineforamenRohen 4th 50
Greater palatine foramen leads to pterygopalatinefossa, with maxillary nerve insideNetter 2nd 2
Pterygopalatinefossa,containingmaxillary nerve,which bringssensoryinnervation tostructuresabove the planeof occlusion ofthe teeth
Maxillary Division Block What would be the effect if we injectedlocal anesthetic into the pterygopalatinefossa? All the structures served by maxillarynerve on that side would be anesthetized.
Netter H&N 593
Netter H&N 592
The Anatomy of Local Anesthesia: The Maxilla University of Detroit Mercy Dental School February 13, 2013 Ronald P Morris, DDS. We have to start somewhere. Let’s start with Pulpal Anesthesia of Maxilla. Maxillary division of t