Transcription
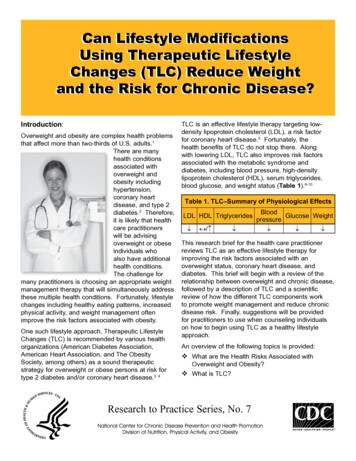
Can Lifestyle ModificationsUsing Therapeutic LifestyleChanges (TLC) Reduce Weightand the Risk for Chronic Disease?Introduction:Overweight and obesity are complex health problemsthat affect more than two-thirds of U.S. adults.1There are manyhealth conditionsassociated withoverweight andobesity includinghypertension,coronary heartdisease, and type 2diabetes.2 Therefore,it is likely that healthcare practitionerswill be advisingoverweight or obeseindividuals whoalso have additionalhealth conditions.The challenge formany practitioners is choosing an appropriate weightmanagement therapy that will simultaneously addressthese multiple health conditions. Fortunately, lifestylechanges including healthy eating patterns, increasedphysical activity, and weight management oftenimprove the risk factors associated with obesity.One such lifestyle approach, Therapeutic LifestyleChanges (TLC) is recommended by various healthorganizations (American Diabetes Association,American Heart Association, and The ObesitySociety, among others) as a sound therapeuticstrategy for overweight or obese persons at risk fortype 2 diabetes and/or coronary heart disease.3, 4TLC is an effective lifestyle therapy targeting lowdensity lipoprotein cholesterol (LDL), a risk factorfor coronary heart disease.5 Fortunately, thehealth benefits of TLC do not stop there. Alongwith lowering LDL, TLC also improves risk factorsassociated with the metabolic syndrome anddiabetes, including blood pressure, high-densitylipoprotein cholesterol (HDL), serum triglycerides,blood glucose, and weight status (Table 1).6-10Table 1. TLC–Summary of Physiological EffectsLDL HDL Triglycerides / BloodGlucose Weightpressure This research brief for the health care practitionerreviews TLC as an effective lifestyle therapy forimproving the risk factors associated with anoverweight status, coronary heart disease, anddiabetes. This brief will begin with a review of therelationship between overweight and chronic disease,followed by a description of TLC and a scientificreview of how the different TLC components workto promote weight management and reduce chronicdisease risk. Finally, suggestions will be providedfor practitioners to use when counseling individualson how to begin using TLC as a healthy lifestyleapproach.An overview of the following topics is provided: What are the Health Risks Associated withOverweight and Obesity? What is TLC?Research to Practice Series, No. 7
How Does the Current U.S. Dietary Fat and Cholesterol Consumption Compare to TLCRecommendations?Why Does TLC Recommend Reducing Intakes ofSaturated Fat, Trans Fat, and Cholesterol whileIncreasing Consumption of Monounsaturated andPolyunsaturated Fats?What Other Dietary Options Can Help ReduceCoronary Heart Disease Risk?What are the Benefits of Increased PhysicalActivity and Weight Management?Research to Practice: Suggestions forIncorporating TLC into a Healthy Lifestyle.What are the Health Risks Associatedwith Overweight and Obesity?Overweight (BMI 25–29.9 kg/m2) and obesity (BMI 30 kg/m2) are independent risk factors for severalchronic disease conditions including coronary heartdisease, hypertension, elevated cholesterol, anddiabetes.11-13 The prevalence of these conditionsincreases as BMI increases. Based on NHANES IIIdata, hypertension, total cholesterol, and low HDLare positively associated with BMI (Figure 1).14 Therisk for developing diabetes also increases withincreasing weight.15 Compared to a healthy weightperson, an overweight individual is 3 times morelikely to develop diabetes within 10 years.16 Thisrisk rises dramatically to 23 times the risk at thehigher BMI levels (BMI 35 kg/m2).16 Individuals withdiabetes are also at an increased risk of developingcoronary heart disease.5 Coronary heart diseasecomprises more than 50% of all cardiovasculardisease-related events in U.S. adults and is theleading cause of diabetes-related death.17Coronary Heart Disease RiskPrevalence (%)Body Mass Index and Coronary Heart Disease Risk Factors4540353025The metabolic syndrome—a clusteringof multiple risk factors associated withoverweight and obesityIt is now known thatwhen certain chronicdisease risk factorsco-occur (abdominalobesity, low HDL,elevated fastingglucose, and elevatedtriglycerides), thereis an increased riskfor cardiovasculardisease anddiabetes. Themetabolic syndromeis a defined clusterof three or morethese chronic diseaserisk factors (Table 2) that are often accompanied byinsulin resistance.5Metabolic syndrome increases the risk for coronaryheart disease and diabetes 2- to 6-fold and 3.5fold, respectively.19-21 Based on NHANES III data,an estimated one-fourth of U.S. adults have themetabolic syndrome.22 Furthermore, based on theNational Cholesterol Education Program (NCEP)criteria listed in Table 2 an estimated 86% of adultsage 50 and older with type 2 diabetes have themetabolic syndrome.23The beneficial health effects of weight loss20151050Of concern is the tendency for diabetes and coronaryheart disease risk factors to co-occur in thosewho are overweight or obese, thus complicatingtreatment options. An estimated 64% and 72% ofoverweight and obese Americans, respectively, havehypertension, elevated cholesterol, or both.14 A studyexamining more than 1.9 million members of a largemanaged care program found hypertension, elevatedtotal cholesterol, and/or diabetes to commonlyco-occur in more than 40% of those diagnosed withone of these conditions.18 25.025.0– 27.027.1– 29.9 30.0Body Mass index (kg/m2)Elevated Blood PressureReduced HDLElevated CholesterolFigure 1. BMI and prevalence of coronary heart disease risk14FigureAdapted1. BMI fromand prevalencecoronaryheart diseasefactors.Brown et al.,of2000.14risk factors. Adapted from Brown et al., 2000.A 10- to 20-pound weight loss often improvesblood pressure, blood cholesterol, and triglyceridelevels.24-27 Weight loss is also an effective therapyfor reducing the risk of diabetes. A subanalysis of aDiabetes Prevention Program cohort comprised ofadults with impaired glucose tolerance receiving anintensive lifestyle intervention, found a 16% reductionin risk for developing diabetes for every kilogram2
Table 2. NCEP Criteria for Metabolic Syndrome*Risk FactorAbdominal obesityMenWomenTriglyceridesHDL cholesterolMenWomenBlood PressureFasting glucoseBox 1. TLC Components:Defining LevelWaist Circumference 40 in 35 in Diet– Reduced intakes of saturated fats,trans fats, and cholesterol.– Dietary options for maximizing LDLreduction and reducing coronaryheart disease risk (plantstanols/sterols, increased solublefiber, and fish). Weight management 150 mg/dL 40 mg/dL 50 mg/dL 130/85 mmHg 100 mg/dLAdapted from National Cholesterol Education Program5(NCEP), ATP III Final Report.*A diagnosis of metabolic syndrome is made when 3 or moreof the risk factors are present.of weight loss, independent of diet and physicalactivity.28 Weight loss has a similar effect on the riskfor developing hypertension. In another observationalstudy, a Framingham Study cohort composed ofoverweight, middle-aged adults without hypertension,found that a moderate weight loss of 15 poundsor more reduced the long-term risk of developinghypertension by 28%.29 Furthermore, in a clinicalstudy of individuals with metabolic syndrome, weightreduction was shown to reduce elevated triglycerides,systolic and diastolic blood pressure, serum glucose,and total cholesterol.30What is TLC?TLC is the lifestyle component of the Third Reportof the NCEP Adult Treatment Panel (ATP) IIIguidelines5 that focuses on diet, weight management,and increased physical activity (Box 1). The ATPIII guidelines specifically target LDL because ofits strong, positive correlation with coronary heartdisease risk.5 Although drugtherapy may also be used,ATP III places a majoremphasis on TLC asan essential therapyfor persons at riskfor coronary heartdisease.5 Thecumulative effectof the TLC dietcomponents listed inBox 1 can reduce LDLby 25-30% comparedto a typical U.S.diet similar to theeffect of drug therapy.5 Increased regular physical activityIn addition to lowering LDL, a TLC-like eating planhas also been shown to positively affect bloodpressure and serum triglyceride levels with little orno effect on HDL levels.6 These effects are furtherenhanced by weight reduction and increased physicalactivity in overweight individuals (Table 1).5, 31 Thisis especially important for those with diabetes and/orthe metabolic syndrome.TLC is a comprehensive lifestyle approach thatincludes specific dietary recommendations (TLCdiet), weight management, and increased physicalactivity. The TLC diet component emphasizesreducing dietary cholesterol ( 200 mg/day), saturatedfats ( 7% of total calories), and trans fats (lowerintake) (Table 3). Total fat comprises 25–35%Table 3. Dietary Recommendations for TLC DietComponentTotal fatSaturated fatPolyunsaturated fatMonounsaturatedfatTrans fatCarbohydrate**Dietary fiberProteinCholesterolSodiumDietary optionsPlant sterols/stanolsSoluble fiberFish (fatty fish)TLC Diet25-35% of total calories* 7% total caloriesUp to 10% of total caloriesUp to 20% of total caloriesLower intake50-60% of total calories20-30 grams per day15-25% of total calories 200 mg/day 2,300 mg/dayAdd up to 2 grams per dayIncrease 5-10 grams per dayInclude in weekly eating plan*ATP III allows an increase of total fat to 35% of total caloriesand a reduction of carbohydrate to 50% in persons withmetabolic syndrome and/or at risk for type 2 diabetes.** Carbohydrate should derive predominantly from foods rich incomplex carbohydrates including grains (especially wholegrains) and fruits and vegetables.3
of total calories, with up to 20% coming frommonounsaturated fats and 10% from polyunsaturatedfats. Finally, optional nutrient considerations formaximizing LDL reduction and reducing coronaryheart disease risk include complementing the dietwith stanols/sterols (2 g/day) and viscous (soluble)fibers (5–10 g/day), and including fish (especially oilyfish such as salmon, tuna, and mackerel) as part ofone’s overall eating plan.The following sections describe each of the TLCcomponents (TLC diet, weight management, andincreased physical activity) in detail and how eachaffects the risk factors associated with coronary heartdisease, type 2 diabetes, and metabolic syndrome.How Do the Current U.S. Dietary Fat andCholesterol Intakes Compare to TLCRecommendations?Fats play diverse roles in the body. Not only do fatsinsulate the body against the elements, but they alsoserve as an energy source for the body. In addition,fats are a crucial component of the cell membranesthat surround each of the billions of cells in the body.Because of the important roles dietary fats play inmaintaining health, it is important to consume boththe proper amount and types of fat. Fats are themost concentrated source of energy (calories) inthe diet, providing nine calories per gram comparedto four calories per gram for either protein orcarbohydrates. As previously mentioned, TLCrecommends that dietary fats make up 25–35% of aperson’s total daily calories. 5 The minimum valueprotects against energy and nutrient deficiencies,elevated triglyceride levels, and lower HDL-C levelswhile the upper limit helps curb saturated fat intakeand excess energy consumption.32 According to a2004 report of theContinuing Surveyof Food Intakesof Individuals(CSFII), the latestestimated medianintake of totaldietary fats in theUnited States isapproximately 33percent of totalcalories.33 Whilethis number iswithin the TLCrecommendationsfor total fat intake,TLC’s secondcriterion for fatintake types of fats is not being met. As shownin (Table 4), Americans are consuming more thanthe recommended amounts of saturated fat andcholesterol.34More about trans fats and dietary cholesterolTrans fats have received much attention lately due totheir negative effect on coronary heart disease risk.36Most trans fats in the United States diet are producedduring the partial hydrogenation of vegetable oils.32Hydrogenation is a food manufacturing processthat turns liquid vegetable oils into the more solidmargarines. This process also makes the fatsmore stable and less likely to turn rancid, which isan especially favorable characteristic for fats usedin deep fat frying. Hydrogenation adds hydrogenatoms to a fat molecule. The more hydrogenatoms that are added to a fat molecule, the more“hydrogenated” and solid the fat becomes. Transfats are produced when the fat molecule is notcompletely hydrogenated, or in other words “partiallyhydrogenated.” Of note, although a small amount ofnaturally occurring trans fats are also found in dairyproducts and meats, these trans fats do not appearto negatively affect cholesterol levels to the samedegree as those derived from partially-hydrogenatedvegetable oils.36Cholesterol is a “fat-like” substance that also playsan integral role in cell membrane structure. Inaddition, cholesterol is required for the productionof bile acids (used in fat digestion) and steroidhormones (e.g., estrogen and testosterone). Thebody is able to produce all of the cholesterol itneeds on a daily basis.5 Therefore, unlike the dailyrequirement for dietary fats, cholesterol does notneed to be acquired through the diet. The current4
U.S. consumption for cholesterol (257 mg/day)is slightly higher than the maximal level of TLCguidelines (Table 4).Why Does TLC Recommend ReducingIntakes of Saturated Fat, Trans Fat, andCholesterol while Increasing Consumption ofMonounsaturated and Polyunsaturated Fats?Saturated Fats. Saturated fat intake is believed tobe the primary dietary factor known to raise LDL.5It has been estimated that for every 1% increasein total calories from saturated fats, there is anassociated 2% increase in LDL.5 Conversely, LDL islowered by 2% for every 1% decrease in total caloriesfrom saturated fats. A recent weight loss study ofobese adults found that a TLC-like diet deriving lessthan 7% of total calories from saturated fats reducedLDL levels an average of 8%.7Trans Fats. In addition to lowering saturated fatintake, TLC also recommends trans fat intake bekept low. Trans fats raise LDL, although not to thesame degree as saturated fats.37 Trans fats alsolower HDL cholesterol when used instead of naturallyoccurring oils such as olive or canola oil.38, 39 Thisdual effect on cholesterol levels actually raises thetotal cholesterol to HDL ratio, which can increasethe risk for coronary heart disease.36, 40, 41 Otherthan their impact on cholesterol levels, trans fatsare also believed to increase other coronary heartdisease risk factors, including elevated triglyceridelevels and alterations to the inside lining of the bloodvessels (endothelial dysfunction).39, 42 Due to thesenegative effects on coronary heart disease risk, TLCrecommends that intakes of trans fats be kept low.Monounsaturated Fatty Acids andPolyunsaturated Fatty Acids. Replacing saturatedfats and trans fats with either monounsaturatedfats or polyunsaturated fats has been shown tolower LDL.43 Data from the 20 Years Follow-upof the Nurses’ Health Study found that a higherpolyunsaturated fat intake (approximately 7% versus5% of total calories) in women is associated witha decreased risk of coronary heart disease.44 Inan earlier examination of the Nurses’ Health StudyTable 4. Common Food Sources for Dietary Fats and CholesterolDietary FatEstimated MeanDailyConsumption34, 35Levels (U.S.)TLCRecommendationsSaturated fats11% total calories 7% total caloriesAnimal-based foods, including whole-fat dairy products(milk, cream, butter, cheese), fatty meats such as beef andpork. Some vegetable-based foods such as coconut,palm, and palm kernel oils also contain relatively highlevels of saturated fats.Trans fats6 grams/dayLower intakeFoods containing or prepared with partially hydrogenatedvegetable oils, including stick margarine, pastries, friedfoods, french fries, and pastries. Naturally occurring transfats are also found in milk, butter, and meats.Monounsaturatedfats12% total caloriesUp to 20% totalcaloriesPolyunsaturatedfats6% total caloriesUp to 10% totalcaloriesFood SourcesOils including olive, canola, and peanut oil.The two primary types of polyunsaturated fats are omega6 and omega-3 fats. Omega-6 fats are found in nuts,seeds, and vegetables oils such as sunflower, canola,safflower, corn, and soybean oils.Plant sources of omega-3 fats ( -linolenic) include canolaoil, soybean oil flaxseed, and English walnuts.Eicosapentaenoic acid (EPA) and docosahexaenoic acid(DHA) are omega-3 fats found in the oily fish such assalmon, tuna, and mackerel. The leaner fish such as cod,haddock, and catfish contain less EPA and DHA.Cholesterol257 mg/day 200 mg/dayFoods of animal origin. Highest amounts are found in liverand egg yolks. Moderate amounts are found in full-fatdairy products, some seafood (shrimp and lobster), andfish (salmon and sardines)5
group, monounsaturated fats were also shown tobe inversely associated with the risk for coronaryheart disease.45 Thus, based on the heart-protectiveeffects of monounsaturated and polyunsaturatedfats, TLC recommends that most of the total dailydietary fat (25–35% of total calories) be comprisedof monounsaturated fat and polyunsaturated fat withintakes ranging up to 20% and 10% of total calories,respectively. See Table 4 for examples of foodscontaining these healthy fats.Other positive health effects of monounsaturated andpolyunsaturated fats occur when these fats replacea portion of one’s dietary carbohydrate intake. Highintakes of carbohydrates ( 60% of calories) inoverweight/obese individuals can potentially elevateblood glucose and triglyceride levels and lower HDLcholesterol.5 Diets that replace a portion of thecarbohydrates with monounsaturated fats and/orpolyunsaturated fats can decrease serum triglyceridelevels with little or no decrease in HDL levels.10 Arecent study looking at the effect of various dietcompositions on coronary heart disease risk foundthat a partial substitution of dietary carbohydrateswith either protein (half from plant sources) orunsaturated fats (primarily monounsaturated)improved blood pressure, LDL, HDL, and triglyceridelevels and reduced the risk of coronary heartdisease.6 This is an important consideration for thosewith insulin resistance or diabetes that have elevatedtriglycerides and low HDL levels.5 For this reason,TLC recommends increasing total fat (primarilycomposed of monounsaturated and polyunsaturatedfats) percentage up to 35% of total calories whilereducing carbohydrate intake to approximately 50%and protein to 15% of total calories for individualswith the metabolic syndrome and/or at risk fordiabetes.5Dietary Cholesterol. On average, a 100 mgincrease in dietary cholesterol increases total serumcholesterol levels by 2.2 mg/dL46 Interestingly, whileegg consumption accounts for more than one-thirdof cholesterol consumption in the United States,prospective data from the Nurses’ Health Study andthe Health Professionals Study found no significantimpact on frequency of egg consumption oncoronary heart disease risk, except among diabeticwomen.47 A more recent meta-analysis found thatdietary cholesterol raises the total cholesterol to HDLcholesterol ratio—negatively affecting the cholesterolprofile.48 Therefore, due to the potential for dietarycholesterol to raise LDL, the TLC diet recommendsconsuming less than 200 mg/day of cholesterol.What Other Dietary Options Can HelpReduce Coronary Heart Disease Risk?Plant Stanols/Sterols.Plant stanols and sterols(stanols/sterols) aretypically derived fromsoybean and tall pine-treeoils. Processed stanols/sterols are easily dissolvedin oils and margarine andare currently available ina wide variety of foods,drinks, margarines, andsoft gel capsules. Onceconsumed, the stanols/sterols are digested andsubsequently changed to a compound that blockscholesterol absorption, which in turn can reduceLDL cholesterol.49 Maximum dietary effects occur atplant stanol/sterol intakes of approximately 2 g/day.5To sustain LDL reductions, stanol/sterol-containingproducts need to be consumed on daily basis.Soluble Fiber. The two primary types of complexcarbohydrates include fiber and starch. Starch isfound in the seed of corn, wheat, rice, oats, andlegumes. The body is able to digest starch and useit for energy. Unlike starch, only a small amount ofdietary fiber can be digested and used for energy.This is because humans lack the enzyme required todigest fiber. Although not a primary energy source forthe body, fiber plays an important role in maintainingthe health of the digestive system and is typicallyclassified by its ability to absorb water: Soluble fiber absorbs water (soluble in water) andturns into a gel-like substance in the intestinesthat helps block cholesterol and fats from beingabsorbed through the intestinal wall into the bloodsystem. Soluble fiber can be found in foods suchas apples, oats, kidney beans, and barley. Insoluble fiber does not absorb water (insolublein water) and essentially moves through theintestines undissolved. For this reason, insolublefiber is also referred to as “roughage.” Insolublefiber helps maintain the function of the digestivesystem by promoting the proper movement offood through the intestines. This form of dietaryfiber is primarily found in whole grains such aswhole wheat and popcorn and vegetables such ascauliflower, broccoli, and green beans.Soluble forms of dietary fiber can reduce LDL,whereas insoluble fibers have not been shown to6
significantly reduce LDL levels.5 A meta-analysis oftrials related to soluble fibers found consuming 2-10g/day produced a small, yet significant reductionin LDL.50 Therefore, to further optimize the LDLlowering effects of the TLC diet, TLC recommendsincluding fiber-rich foods that add at least 5-10 gramsof soluble fibers to the daily fiber intake (e.g., apples,bananas, oatmeal, legumes, and barley).Fish Consumption. Omega-3 fats are a specifictype of polyunsaturated fat known to reduce the riskfor sudden death and death from coronary heartdisease.51, 52 Although omega-3 fats are foundin plants (α-linolenic acid) and fish (Table 4), theomega-3 fats found in fish, eicosapentaenoic acid(EPA) and docosahexaenoic acid (DHA), appear tobe more effective in reducing coronary heart diseaserisk.52 The beneficial effects of fish consumptionhave been observed at levels of one to two ouncesper day, with further reductions in coronary heartdisease risk occurring in a dose-dependent mannerup to about 5 servings per week.53 Therefore, TLCguidelines support the American Heart Association’srecommendations37 that at least two 4-ounce servingsof fish (especially oily fish such as salmon, tuna, andmackerel) be consumed each week.Dietary Salt. Based on NHANES data,approximately 65 million U.S. adults have highblood pressure, an independent risk factor forcardiovascular disease.54 Although there arenumerous factors that can elevate blood pressure,increases in dietary salt (sodium chloride) intakeare associated with increased blood pressure.55Conversely, a reduced salt intake can lowerblood pressure and prevent hypertension. Therehave been many studies that have looked at theeffects of dietary salt restriction in reducing bloodpressure in individuals with high blood pressure.56,57These studies have consistently shown modestblood pressure reductions associated with saltrestricted diets. Similar studies assessing peoplewith high-normal blood pressure (prehypertension)also showed a reduction in blood pressure withreduced salt intake.58, 59 A recent observationalfollow-up study from the Trials of HypertensionPrevention (TOHP) found that a 25% to 35%reduction in dietary salt intake reduced the riskof cardiovascular disease (defined as myocardialinfarction, stroke, revascularization, or cardiovasculardeath) by 25% compared to those with no sodiumreduction.60 Based on these cumulative findings, TLCrecommends limiting sodium intake to less than 2,300mg per day.5What are the Benefits of IncreasedPhysical Activity and WeightManagement?Because an overweight status and physical inactivityare highly correlated with the metabolic syndrome;weight reduction and increased physical activity usingTLC are recommended for those who are overweightor obese and at risk for type 2 diabetes and/orcoronary heart disease.3-5 Lifestyle interventionsare effective therapies in promoting weight loss andimproving coronary heart disease and diabetes riskfactors.31, 61-65 Specifically, TLC-like interventions havebeen shown to promote weight loss while improvingcoronary heart disease and diabetes risk factors.7, 9, 10Reduced-Calorie TLC Diet for Weight LossAchieving energy balance (calories consumed calories expended) is key to maintaining a healthyweight. Weight loss occurs when calories expendedexceed calories consumed. Optimally, this isachieved by reducing caloric intake while increasingdaily physical activity levels.An important consideration of any reduced-caloriediet plan is whether it provides the appropriatebalance of nutrients at the lower calorie levels. Forexample, a particular diet may provide the properbalance of carbohydrates, protein, fats, and othernutrients at a 2,000 calorie level, but not provideadequate amounts of fat, protein, and/or othernutrients when the daily calories are reduced to 1,200calories.Overall, the TLC diet is low in saturated fats, dietarycholesterol, and sodium, while emphasizing adequatelevels of monounsaturated and polyunsaturated fats.These nutrient levels remain constant at the reducedcalorie levels, making it a high quality/balanceddiet for weight reduction.66 In addition, along with7
providing the recommended amounts and types ofdietary fats, a reduced-calorie TLC diet plan alsomaintains a healthy balance between carbohydrate,protein, and total fat intake.66Increasing Physical ActivityWeight reductionthat incorporatesincreased physicalactivity has beneficialeffects on severalmetabolic risk factorsincluding insulinresistance, bloodpressure, serumtriglycerides, LDL,and HDL levels.5,67-70In a recentweight loss studyof overweight andobese women withmetabolic syndrome,the addition ofphysical activity toa reduced-caloriediet improved metabolic syndrome risk factorsapproximately 3.5-fold as compared to diet alone.71SummaryBecause of the high prevalence of overweight/obesityand associated chronic disease risk in the UnitedStates, it is likely that health care practitioners willbe required to treat overweight or obese individualswith multiple chronic disease risk factors. TLC isan effective lifestyle therapy in the treatment of bothelevated LDL cholesterol levels and hypertension.Because it also promotes weight loss while improvingcoronary heart disease risk factors associatedwith the metabolic syndrome, TLC can also be animportant therapeutic strategy in the prevention oftype 2 diabetes.Research to Practice: Suggestionsfor Incorporating TLC into aHealthy Lifestyle “To reduce the risk of chronic disease inadulthood: Engage in at least 30 minutes ofmoderate-intensity physical activity, above usualactivity, at work or home on most days of theweek. For most people, greater health benefits can beobtained by engaging in physical activity of morevigorous intensity or longer duration. To help manage body weight and preventgradual, unhealthy body weight gain in adulthood:Engage in approximately 60 minutes ofmoderate- to vigorous-intensity activity on mostdays of the week while not exceeding caloricintake requirements.This researchreview has detailedhow a healthy dietand increasedphysical activityusing a TLC-likeapproach canhelp with weightmanagement whiledecreasing the riskfor chronic disease.Even though theprimary focusof the TLC “dietplan” is reducingdietary cholesteroland replacingsaturated andtrans fats with themore heart-healthyfats, the TLC dietalso features a sound eating plan that includesmany lower energy density foods including fruits,vegetables, whole grains, lean meats, poultry,seafood, legumes, and low-fat dairy products.Furthermore, TLC helps balance calories consumedwith calories expended (energy balance) bycombining increased daily physical activity levels withan appropriate calorie level for weight management.66 To sustain weight loss in adulthood: Participatein at least 60 to 90 minutes of daily moderateintensity physical activity while not exceedingcaloric intake requirements. Some people mayneed to consult with a healthcare provider beforeparticipating in this level of activity.”The remaining sections are written specifically forthe client/patient. Practitioners can use the followingtips to help get their clients started on the road to ahealthier lifestyle with TLC. When adopting a TLClike approach, the client may need to seek the adviceof a registered dietitian or other health professional.Thus, because of its positive effects on coronaryheart disease, diabetes, and metabolic syndromerisk factors, TLC suggests physical activity levelsbased on the 2005 Dietary Guidelines for Americansrecommendations:5, 32, 728
Begin with Determining Calorie NeedsWhen it comes to maintaining your current weight,the key is achieving energy balance balancing thenumber of calories you consume with the amount ofcalories your body requires to support its daily energyneeds. In contrast, if you want to lose weight, itmeans taking in less calories than your body needson a daily basis (energy deficit). The first step forany healthy eating plan is to determine a daily calorielevel based on whether you want to maintain or loseweight.For weight loss, the National Heart, Lung, andBlood Institute (NHLBI)11 recommends decreasinga person’s intake approximately 500–1,000 caloriesper day, which will result in an approximate 1 to 2pound weight loss per week and an average 8%weight loss after 6 months.4 A simplified approachfor determining an appropriate calorie level for weightloss in individuals who are overweight is basedon a person’s initial
density lipoprotein cholesterol (LDL), a risk factor for coronary heart disease. 5. Fortunately, the health benefits of TLC do not stop there. Along with lowering LDL, TLC also improves risk factors associated with the metabolic syndrome and diabetes, including blood pressure, high-density lipoprotein