Transcription
Dizziness: Approach to Evaluationand ManagementHERBERT L. MUNCIE, MD, Louisiana State University School of Medicine, New Orleans, LouisianaSUSAN M. SIRMANS, PharmD, University of Louisiana at Monroe School of Pharmacy, Monroe, LouisianaERNEST JAMES, MD, Louisiana State University School of Medicine, New Orleans, LouisianaDizziness is a common yet imprecise symptom. It was traditionally divided into four categories based on the patient’shistory: vertigo, presyncope, disequilibrium, and light-headedness. However, the distinction between these symptoms is of limited clinical usefulness. Patients have difficulty describing the quality of their symptoms but can moreconsistently identify the timing and triggers. Episodic vertigo triggered by head motion may be due to benign paroxysmal positional vertigo. Vertigo with unilateral hearing loss suggests Meniere disease. Episodic vertigo not associatedwith any trigger may be a symptom of vestibular neuritis. Evaluation focuses on determining whether the etiology isperipheral or central. Peripheral etiologies are usually benign. Central etiologies often require urgent treatment. TheHINTS (head-impulse, nystagmus, test of skew) examination can help distinguish peripheral from central etiologies.The physical examination includes orthostatic blood pressure measurement, a full cardiac and neurologic examination, assessment for nystagmus, and the Dix-Hallpike maneuver. Laboratory testing and imaging are not required andare usually not helpful. Benign paroxysmal positional vertigo can be treated with a canalith repositioning procedure(e.g., Epley maneuver). Treatment of Meniere disease includes salt restriction and diuretics. Symptoms of vestibular neuritis are relieved with vestibular suppressant medications and vestibular rehabilitation. (Am Fam Physician.2017;95(3):154-162. Copyright 2017 American Academy of Family Physicians.)CME This clinical contentconforms to AAFP criteriafor continuing medicaleducation (CME). SeeCME Quiz Questions onpage 149.Author disclosure: No relevant financial affiliations. Patient information:A handout on this topic,written by the authors ofthis article, is availableat ziness is a common yet im precise symptom often en coun tered by family physicians.Primary care physicians see atleast one-half of the patients who presentwith dizziness.1 The differential diagnosis isbroad, with each of the common etiologiesaccounting for no more than 10% of cases2(Table 11,3). Because the symptoms are vague,physicians must distinguish benign from se rious causes that require urgent evaluationand treatment.Dizziness was traditionally classifiedinto four categories based on the patient’sdescription: (1) vertigo, (2) presyncope, (3)disequilibrium, and (4) light-headedness.4However, current approaches do not includepresyncope and do not use the vague termlight-headedness.5 Patients often have dif ficulty describing their symptoms and maygive conflicting accounts at different times.3Symptom quality does not reliably predictthe cause of dizziness.6 Physicians are cau tioned against overreliance on a descriptiveapproach to guide the diagnostic evalua tion.7 Alternatively, attention to the timingand triggers of dizziness is preferred over thesymptom type because patients more consis tently report this information.3,7General ApproachQuestions regarding the timing (onset,duration, and evolution of dizziness) andtriggers (actions, movements, or situations)that provoke dizziness can categorize thedizziness as more likely to be peripheral orcentral in etiology. Findings from the physi cal examination can help confirm a probablediagnosis. A diagnostic algorithm can helpdetermine whether the etiology is peripheralor central (Figure 1).TITRATE THE EVALUATIONTiTrATE is a novel diagnostic approach todetermining the probable etiology of diz ziness or vertigo.2 The approach uses theTiming of the symptom, the Triggers thatprovoke the symptom, And a TargetedExamination. The responses place the diz ziness into one of three clinical scenarios:episodic triggered, spontaneous episodic, orcontinuous afpVolume95,Physicians.NumberFor3 theFebruary1, 2017Downloadedfrom theAmericanFamily Physician website at www.aafp.org/afp.Copyright 2017 American Academyof Familyprivate, noncom mercial use of one individual user of the website. All other rights reserved. Contact copyrights@aafp.org for copyright questions and/or permission requests.
DizzinessSORT: KEY RECOMMENDATIONS FOR PRACTICEClinical recommendationEvidenceratingReferencesVertigo associated with unilateral hearing loss should raise suspicion for Meniere disease.C41The physical examination in patients with dizziness should include orthostatic blood pressure measurement,nystagmus assessment, and the Dix-Hallpike maneuver for triggered vertigo.C16The HINTS (head-impulse, nystagmus, test of skew) examination can help differentiate a peripheral cause ofvestibular neuritis from a central cause.C20Laboratory testing and imaging are not recommended when no neurologic abnormality is found on examination.C1Benign paroxysmal positional vertigo is treated with a canalith repositioning procedure (e.g., Epley maneuver).A30Vestibular neuritis symptoms may be relieved with medication and vestibular rehabilitation.C20Meniere disease may improve with a low-salt diet and diuretic use.B41A consistent, good-quality patient-oriented evidence; B inconsistent or limited-quality patient-oriented evidence; C consensus, disease-orientedevidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to http://www.aafp.org/afpsort.Table 1. Differential Diagnosis of Dizziness and Vertigo:Common CausesCause (most toleast frequent)Clinical descriptionPeripheral causesBenign paroxysmalpositional vertigoTransient triggered episodes of vertigo caused bydislodged canaliths in the semicircular canalsVestibular neuritisSpontaneous episodes of vertigo caused byinflammation of the vestibular nerve orlabyrinthine organs, usually from a viral infectionMeniere diseaseSpontaneous episodes of vertigo associatedwith unilateral hearing loss caused by excessendolymphatic fluid pressure in the inner earOtosclerosisSpontaneous episodes of vertigo caused byabnormal bone growth in the middle ear andassociated with conductive hearing lossCentral causesVestibular migraineSpontaneous episodes of vertigo associated withmigraine headachesCerebrovascular diseaseContinuous spontaneous episodes of vertigocaused by arterial occlusion or insufficiency,especially affecting the vertebrobasilar systemCerebellopontine angleand posterior fossameningiomasContinuous spontaneous episodes of dizzinesscaused by vestibular schwannoma (i.e., acousticneuroma), infratentorial ependymoma, brainstemglioma, medulloblastoma, or neurofibromatosisOther causesPsychiatricInitially episodic, then often continuous episodes ofdizziness without another cause and associatedwith psychiatric condition (e.g., anxiety,depression, bipolar disorder)Medication inducedContinuous episodes of dizziness without anothercause and associated with a possible medicationadverse effectCardiovascular/metabolicAcute episodic symptoms that are not associatedwith any triggersOrthostaticAcute episodic symptoms associated with a changein position from supine or sitting to standingInformation from references 1 and 3.February 1, 2017 Volume 95, Number 3www.aafp.org/afp With episodic triggered symptoms, patientshave brief episodes of intermittent dizzinesslasting seconds to hours. Common triggersare head motion on change of body position(e.g., rolling over in bed). Episodic triggeredsymptoms are consistent with a diagnosis ofbenign paroxysmal positional vertigo (BPPV).With spontaneous episodic symptoms (notrigger), patients have episodes of dizzinesslasting seconds to days. Because these epi sodes have no trigger, the patient’s historyestablishes the diagnosis. Common diagnos tic considerations for spontaneous episodicsymptoms include Meniere disease, vestibu lar migraine, and psychiatric diagnoses suchas anxiety disorders. Symptoms associatedwith lying down are more likely vestibular.With continuous vestibular symptoms,patients have persistent dizziness lastingdays to weeks. The symptoms may be due totraumatic or toxic exposure. Classic vestibu lar symptoms include continuous dizzinessor vertigo associated with nausea, vomiting,nystagmus, gait instability, and head-motionintolerance. In the absence of trauma orexposures, these findings are most consistentwith vestibular neuritis or central etiologies.However, central causes can also occur withpatterns triggered by movement.HISTORY: TIMING, TRIGGERS,AND MEDICATIONSPatients who describe a sensation of selfmotion when they are not moving or a sensa tion of distorted self-motion during normalhead movement may have vertigo.5 Vertigois the result of asymmetry within the ves tibular system or a disorder of the peripherallabyrinth or its central connections.8,9 TheAmerican Family Physician 155
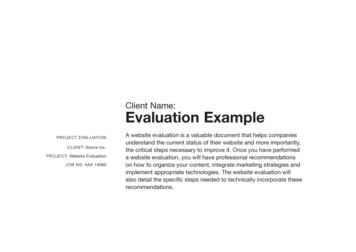
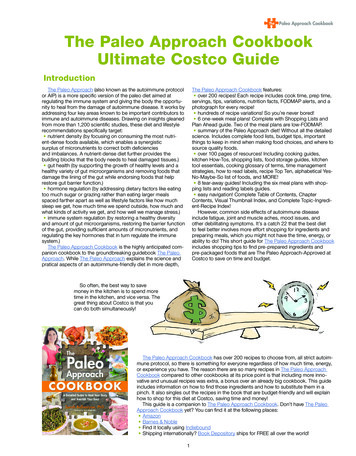
DizzinessAssessment of DizzinessPatient presents with dizziness or vertigoIs the timing episodic or continuous?EpisodicContinuousIs it triggered or spontaneous?Is it associated with traumaor toxins, or spontaneous?Triggered*SpontaneousTrauma or toxinSpontaneousDix-Hallpike maneuverHearing lossPositiveBenign paroxysmalpositional vertigoNegativeAssess dachePsychiatricsymptomsVestibularmigrainePanic attack,psychiatricconditionHINTS examinationBarotraumaMedicationsSaccade present,unidirectionalhorizontal nystagmus,normal test of skewNo saccade, nystagmusdominantly vertical,torsional or gazeevoked bidirectional,abnormal test of skewPeripheral etiologyCentral etiology†Vestibular neuritisStroke or transientischemic attack*—Exacerbation of symptoms with movement does not aid in determining whether the etiology is peripheral vs. central.†—Central causes can also occur with patterns triggered by movement.Figure 1. Algorithm for the diagnostic evaluation of dizziness. (HINTS head-impulse, nystagmus, test of skew.)distinction between vertigo and dizziness is of limitedclinical usefulness.2If vertigo is described, physicians should ask abouthearing loss, which could suggest Meniere disease.10Diagnostic criteria for Meniere disease include episodicvertigo (at least two episodes lasting at least 20 minutes)associated with documented low- to medium-frequencysensorineural hearing loss by audiometric testing in theaffected ear and tinnitus or aural fullness in the affectedear.10 The auditory symptoms are initially unilateral.Physicians should determine whether the vertigo istriggered by a specific position or change in position.BPPV is triggered with sudden changes in position, suchas a quick turn of the head on awakening or tipping thehead back in the shower. Dizziness from orthostatichypotension occurs with movement to the upright posi tion. Clinicians may erroneously assume that dizzinessthat worsens with movement is associated with a benigncondition in patients with persistent dizziness.11 However,156 American Family Physicianexacerbation of symptoms with movement is common tomost causes of persistent dizziness and does not aid indetermining whether the etiology is peripheral vs. central(benign vs. dangerous).7WHAT IS NEW ON THIS TOPIC: EVALUATIONOF DIZZINESSTiTrATE is a novel diagnostic approach to determine theprobable etiology of dizziness or vertigo. It uses the Timing ofthe symptom, the Triggers that provoke the symptom, And aTargeted Examination. The patient’s response determines theclassification of dizziness as episodic triggered, spontaneousepisodic, or continuous vestibular.In a study of older patients in a primary care setting,medications were implicated in 23% of cases of dizziness.The HINTS (head-impulse, nystagmus, test of skew) examinationcan help differentiate a peripheral cause of vestibular neuritisfrom a central cause.www.aafp.org/afpVolume 95, Number 3 February 1, 2017
DizzinessMedications were implicated in 23% of cases ofdizziness in older adults in a primary care setting12(Table 21,13,14). The use of five or more medications isassociated with an increased risk of dizziness.15 Olderpatients are particularly susceptible to medicationadverse effects because of age-related pharmacokineticand pharmacodynamic changes.13PHYSICAL EXAMINATIONFindings from the physical examination—including acardiac and neurologic assessment, with attention to thehead, eye, ear, nose, and throat examination—are usu ally normal in patients presenting with dizziness.Blood pressure should be measured while the patientis standing and in the supine position.16 Orthostatichypotension is present when the systolic blood pres sure decreases 20 mm Hg, the diastolic blood pressuredecreases 10 mm Hg, or the pulse increases 30 beats perminute after going from supine to standing for one min ute.17 A full neurologic examination should be performedin patients with orthostatic dizziness but no hypotensionor BPPV.The patient’s gait should be observed and a Rombergtest performed. Patients with an unsteady gait should beassessed for peripheral neuropathy.18 A positive Rombergtest suggests an abnormality with proprioception recep tors or their pathway.The use of the HINTS (head-impulse, nystagmus, testof skew) examination can help distinguish a possiblestroke (central cause) from acute vestibular syndrome(peripheral cause).19 A video demonstrating this exami nation is available at /partner id/797802/uiconf id/27472092/entry id/0 b9t6s0wh/embed/auto.Head-Impulse. While the patient is sitting, the head isthrust 10 degrees to the right and then to the left whilethe patient’s eyes remain fixed on the examiner’s nose.If a saccade (rapid movement of both eyes) occurs, theetiology is likely peripheral.20 No eye movement stronglysuggests a central etiology.19Nystagmus. The patient should follow the examiner’sfinger as it moves slowly left to right. Spontaneous unidi rectional horizontal nystagmus that worsens when gazingin the direction of the nystagmus suggests a peripheralcause (vestibular neuritis).7 Spontaneous nystagmus thatis dominantly vertical or torsional, or that changes direc tion with the gaze (gaze-evoked bidirectional) suggests acentral etiology. Central pathology nystagmus changesdirection less than half the time6 and can be suppressedwith fixation.21 A video-oculography device is avail able to quantitatively measure eye movement.22 FrenzelFebruary 1, 2017 Volume 95, Number 3goggles used to detect involuntary eye movements havebeen helpful with nystagmus assessment.23Test of Skew. Test of skew is assessed by asking thepatient to look straight ahead, then cover and uncovereach eye. Vertical deviation of the covered eye afteruncovering is an abnormal result. Although this is a lesssensitive test for central pathology, an abnormal result isfairly specific for brainstem involvement.Table 2. Medications Associated with DizzinessMedicationCausal mechanismAlcoholCardiac effects:hypotension, posturalhypo tension, torsadesde pointes, otherarrhythmiasAntiarrhythmics, class 1aAntidementia agentsAntiepilepticsAntihistamines (sedating)AntihypertensivesAnti-infectives: anti-influenzaagents, antifungals, quinolonesAntiparkinsonian agentsAttention-deficit/hyperactivitydisorder agentsDigitalis terase type 5 inhibitorsSkeletal muscle relaxantsSodium–glucose cotransporter-2inhibitorsUrinary anticholinergicsSkeletal muscle relaxantsUrinary and l anti cholinergiceffectsCerebellar toxicityBenzodiazepinesLithiumAntidiabetic agentsHypoglycemiaBeta adrenergic blockersAminoglycosidesOtotoxicityAntirheumatic agentsAnticoagulantsAntithyroid agentsBleeding complications(anti coagulants), bonemarrow suppression(anti thyroid agents)Information from references 1, 13, and 14.www.aafp.org/afp American Family Physician 157
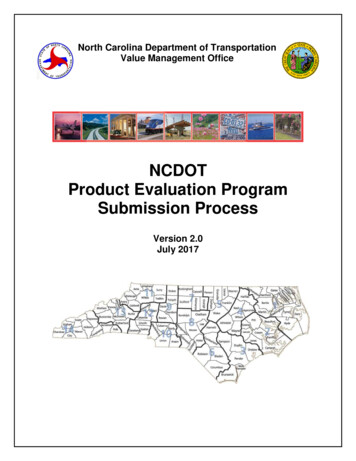
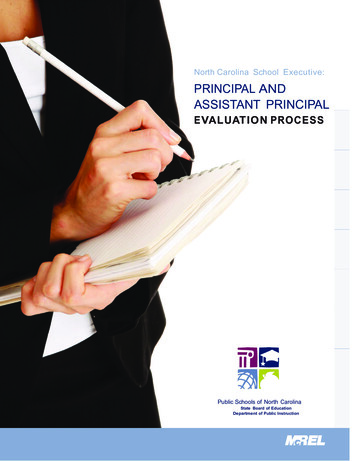
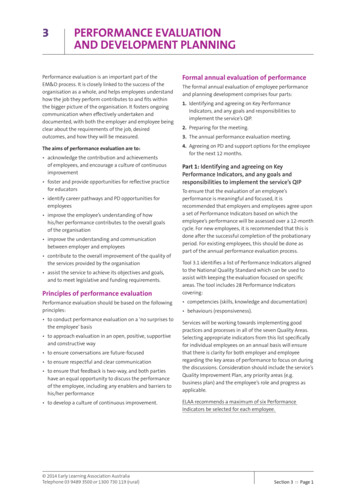
DizzinessAILLUSTRATIONS BY MARCIA HARTSOCK45 BFigure 2. Dix-Hallpike maneuver (used to diagnose benign paroxysmal positional vertigo). This test consists of a seriesof two maneuvers: (A) With the patient sitting on the examination table, facing forward, eyes open, the physicianturns the patient’s head 45 degrees to the right. (B) The physician supports the patient’s head as the patient lies backquickly from a sitting to supine position, ending with the head hanging 20 degrees off the end of the examinationtable. The patient remains in this position for 30 seconds. Then the patient returns to the upright position and isobserved for 30 seconds. Next, the maneuver is repeated with the patient’s head turned to the left. A positive test isindicated if any of these maneuvers trigger vertigo with or without nystagmus. A video of the procedure is availableat http://www.youtube.com/watch?v vRpwf2mI3SU.Reprinted with permission from Swartz R, Longwell P. Treatment of vertigo. Am Fam Physician. 2005;71(6):1117.BPPV is diagnosed with the Dix-Hallpike maneuver(Figure 2).24 Transient upbeat-torsional nystagmus dur ing the maneuver is diagnostic of BPPV if the timing andtrigger are consistent with BPPV. Nystagmus may notdevelop immediately, and a sense of vertigo may occurand last for one minute. A negative result does not ruleout BPPV if the timing and triggers are consistent withBPPV.25 Nystagmus with the maneuver may be due to acentral etiology, especially if the timing and trigger arenot consistent with BPPV.LABORATORY TESTING AND IMAGINGMost patients presenting with dizziness do not requirelaboratory testing. Patients with chronic medical condi tions (e.g., diabetes mellitus, hypertension) may requireblood glucose and electrolyte measurements. Patientswith symptoms suggestive of cardiac disease shouldundergo electrocardiography, Holter monitoring, andpossibly carotid Doppler testing. However, in a summaryanalysis of multiple studies that included 4,538 patients,only 26 (0.6%) had a laboratory result that explainedtheir dizziness.16Routine imaging is not indicated.1 However, anyabnormal neurologic finding, including asymmetric orunilateral hearing loss, requires computed tomographyor magnetic resonance imaging to evaluate for cerebro vascular disease. Hearing loss with vertigo and normalneuroimaging suggests Meniere disease.Peripheral EtiologiesPeripheral causes of dizziness arise from abnormalitiesin the peripheral vestibular system, which is comprised158 American Family Physicianof the semicircular canals, the saccule, the utricle, andthe vestibular nerve. Common peripheral causes of diz ziness/vertigo include BPPV, vestibular neuritis (i.e., ves tibular neuronitis), and Meniere disease.26BENIGN PAROXYSMAL POSITIONAL VERTIGOBPPV occurs when loose otoconia, known as canaliths,become dislodged and enter the semicircular canals, usu ally the posterior canal.27 BPPV can occur at any age, butis most common between 50 and 70 years.28 No obviouscause is found in 50% to 70% of older patients, but headtrauma is a possibility in younger persons.29Treatment of BPPV consists of a canalith repositioningprocedure such as the Epley maneuver, which repositionsthe canalith from the semicircular canal into the vestibule30(Figure 324). The success rate is approximately 70% on thefirst attempt, and nearly 100% on successive maneuvers.29Home treatment with Brandt-Daroff exercises (http://www.youtube.com/watch?v voZXtTUdQ00) can also besuccessful. If there is no improvement with repeated reposi tioning maneuvers, or if atypical or ongoing nystagmus withnausea is present, another cause should be considered.27Pharmacologic treatment has no role in the treatmentof BPPV. Vestibular suppressant medications should beavoided because they interfere with central compensa tion and may increase the risk of falls.20,31VESTIBULAR NEURITISVestibular neuritis, the second most common cause ofvertigo, is thought to be of viral origin. It most commonlyaffects persons 30 to 50 years of age. Men and women areaffected equally.www.aafp.org/afpVolume 95, Number 3 February 1, 2017
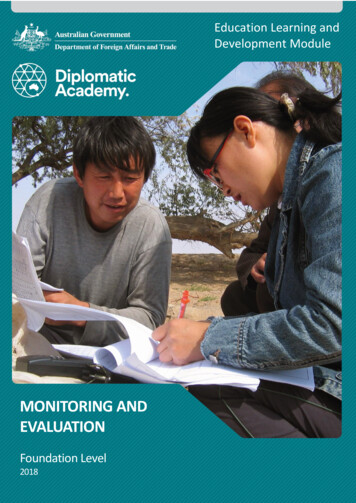
Dizziness45 90 ADBEFigure 3. Epley maneuver. (A) The patient sits on the examination table, with eyes open and head turned 45 degreesto the right. (B) The physician supports the patient’s headas the patient lies back quickly from a sitting to supineposition, ending with the head hanging 20 degrees offthe end of the examination table. (C) The physician turnsthe patient’s head 90 degrees to the left side. The patientremains in this position for 30 seconds. (D) The physicianturns the patient’s head an additional 90 degrees to theleft while the patient rotates his or her body 90 degreesin the same direction. The patient remains in this positionfor 30 seconds. (E) The patient sits up on the left side ofthe examination table. The procedure may be repeatedon either side until the patient experiences relief of symptoms. A video of the procedure is available at http://www.youtube.com/watch?v ZqokxZRbJfw&NR 1.ILLUSTRATIONS BY MARCIA HARTSOCK90 Reprinted with permission from Swartz R, Longwell P. Treatment of vertigo.Am Fam Physician. 2005;71(6):1119.CVestibular neuritis is diagnosed on the basis of theclinical history and physical examination.32 It can causesevere rotatory vertigo with nausea and apparent move ment of objects in the visual field (oscillopsia), horizon tally rotating spontaneous nystagmus to the nonaffectedside, or an abnormal gait with a tendency to fall to theaffected side. Hearing is not impaired in this condi tion. The Dix-Hallpike maneuver is not useful becausepatients with vestibular neuritis do not have episodicpositionally triggered symptoms.February 1, 2017 Volume 95, Number 3As vestibular compensation occurs, the patient’s vertigoresolves slowly over a few days.33 In 50% of patients,the underlying nerve damage may take two months toresolve.34 However, a sensation of disequilibrium maypersist for months because of unilateral impairment ofvestibular function. Vertigo may recur, indicating interfer ence with compensation. If the attacks do not become suc cessively shorter, another diagnosis should be considered.Reassurance, explanation, and advice are essential, incombination with symptomatic treatment for the firstwww.aafp.org/afp American Family Physician 159
DizzinessTable 3. Vestibular Suppressant MedicationsMedicationDosageAdverse effectsCost*Metoclopramide(Reglan)5 to 10 mg orally every6 hours, or 5 to 10 mgslowly IV every 6 hoursAkathesia, atrioventricular block, bradycardia, bronchospasm,dizziness, drowsiness, dystonic reaction, gynecomastia,nausea, tardive dyskinesiaTablets: 2 ( 25)Prochlorperazine5 to 10 mg orally or IMevery 6 to 8 hoursAgitation, dizziness, drowsiness, dystonic reaction, extra pyramidal symptoms, photosensitivity, tardive dyskinesiaTablets: 2Dimenhydrinate50 mg orally every 6 hoursAnorexia, blurred vision, dizziness, drowsiness, nausea 3Meclizine(Antivert)12.5 to 50 mg orally every4 to 8 hoursBlurred vision, drowsiness, fatigue, headache, vomiting 1 to 4 ( 8 to 47)Promethazine25 mg every 6 hours orally,IM, or rectally every 4 to12 hoursAgitation, bradycardia, confusion, constipation, drowsiness,dizziness, dystonia, extrapyramidal symptoms, gynecomastia,photosensitivity, urinary retentionTablets: 2Diazepam(Valium)2 to 10 mg orally or IVevery 4 to 8 hoursAmnesia, drowsiness, slurred speech, vertigoTablets: 1 ( 30 to 168)Lorazepam(Ativan)1 to 2 mg orally every4 hoursAmnesia, dizziness, drowsiness, slurred speech, vertigo 1 ( 320 to 500)AntiemeticsAntihistaminesSuppository: 3BenzodiazepinesIM intramuscularly; IV intravenously.*—Estimated retail price for a three-day course based on information obtained at http://www.goodrx.com (accessed October 7, 2016). Generic pricelisted first; brand name in parentheses.Information from references 20 and 24.few days.33 The prognosis is excellent, but developmentof BPPV after an attack of vestibular neuritis may occurin 15% of patients.35Vestibular neuritis is treated with medications and ves tibular rehabilitation20 (Table 320,24). Antiemetics andantinausea medications should be used for no more thanthree days because of their effects in blocking centralcompensation. Vertigo and associated nausea or vomit ing can be treated with a combination of antihistamine,antiemetic, or benzodiazepine. Although systemic cor ticosteroids have been recommended as a treatment forvestibular neuritis, there is insufficient evidence for theirroutine use.36 Antiviral medications are ineffective.37MENIERE DISEASEMeniere disease causes vertigo and unilateral hearingloss. Although it can develop at any age, it is more com mon between 20 and 60 years.38 The vertigo associatedwith Meniere disease is often severe enough to necessitatebed rest and can cause nausea, vomiting, and loss of bal ance. Other symptoms include sudden slips or falls, andheadache with hearing loss worsened during an attack.39The underlying pathology is excess endolymphaticfluid pressure leading to inner ear dysfunction; how ever, the exact cause is unknown.40 Patients manifest aunidirectional, horizontal-torsional nystagmus duringvertigo episodes.First-line treatment of Meniere disease involves life style changes, including limiting dietary salt intake to160 American Family Physicianless than 2,000 mg per day, reducing caffeine intake,and limiting alcohol to one drink per day. Daily thiazidediuretic therapy can be added if vertigo is not controlledwith lifestyle changes.41Transtympanic injections of glucocorticoids42 andgentamicin43 can improve vertigo. Although transtym panic glucocorticoids may improve hearing, transtym panic gentamicin is associated with hearing loss andshould be reserved for patients who already have signifi cant hearing loss.20Vestibular suppressant medications may be used foracute attacks.20 Prochlorperazine, promethazine, anddiazepam (Valium) have been effective. Surgery is anoption for patients with refractory symptoms.41 Ves tibular exercises may be helpful for patients with uni lateral peripheral vestibular dysfunction.44 Vestibularrehabilitation may be needed for persistent tinnitus orhearing loss.Central EtiologiesThe vestibular nuclei, cerebellum, brainstem, spinalcord, and vestibular cortex make up the central vestibu lar system. Central abnormalities cause approximately25% of dizziness experienced by patients.45 Commoncentral etiologies include vestibular migraine and verte brobasilar ischemia. Patients with central pathology maypresent with disequilibrium and ataxia rather than truevertigo. However, vertigo can be a presenting symptomof an impending cerebrovascular event.46,47www.aafp.org/afpVolume 95, Number 3 February 1, 2017
DizzinessPotentially deadly central causes of acute vestibularsyndrome may mimic a more benign peripheral disor der, and a stroke may present with no focal neurologicsigns. Computed tomography does not have adequatesensitivity to distinguish stroke from benign causes ofacute vestibular syndrome. The HINTS examinationis highly sensitive and specific in identifying stroke inpatients with acute vestibular syndrome, and it is supe rior to diffusion-weighted magnetic resonance imagingin ruling out stroke.6This article updates a previous article by Post and Dickerson.1VESTIBULAR MIGRAINESUSAN M. SIRMANS, PharmD, is an associate professor in the Departmentof Clinical Sciences at the University of Louisiana at Monroe School ofPharmacy.Episodic vertigo in a patient with a history of migraineheadaches suggests vestibular migraine.48 Vestibularmigraine is one of the most common causes of episodicvertigo among children.49 Among adults, it is three timesmore common among women and more often occursbetween 20 and 50 years of age.50 A family history of ves tibular migraine is a risk factor.The diagnostic criteria for vestibular migraine includeat least five episodes of vestibular symptoms of moder ate or severe intensity lasting five minutes to 72 hours;current or previous history of migraine headache; oneor more migraine features, and at least 50% with ves tibular symptoms; and no other cause of vestibularsymptoms.51Initial management focuses on identifying and avoid ing migraine triggers. Stress relief is recommended, andadequate sleep and exercise are encouraged. Vestibularsuppressant medications are helpful.20 Because of a lackof well-designed randomized clinical trials, preven tion recommendations are based on expert opinion.52Preventive medications include anticonvulsants, betaadrenergic blockers, calcium channel blockers, tricyclicantidepressants, butterbur extract, and magnesium.The goal is a 50% reduction in attacks.20 It is not clearwhether migraine abortive therapy is effective in treat ing vertigo.20VERTEBROBASILAR ISCHEMIAThe blood supply to the brainstem, cerebellum, andinner ear is derived from the vertebrobasilar system. Anymajor branch occlusion can cause vertigo. Diagnosisusually relies on a history of brainstem symptoms, suchas diplopia, dysarthria, weakness, or clumsiness of thelimbs. Vertigo is the initial symptom in 48% of patients,although fewer than one-half will have an associatedneurologic finding.53 Treatment includes antiplatelettherapy and reduction of risk factors for cerebrovasculardisease. Warfarin (Coumadin) has been used in cases ofsignificant vertebral or basilar artery stenosis.54February 1, 2017 Volume 95, Number 3Data Sources: A PubMed and Ovid search was completed in ClinicalQueries using the key words dizziness, vertigo, disequilibrium, andpresyncope. Additional search terms included Meniere disease, Epleymaneuver, and vestibular neuritis. The Cochrane Library and EssentialEvidence Plus were searched using the key words vertigo and dizziness.Last search date: October 2015.The AuthorsHERBERT L. MUNCIE, MD, is a professor in the Department of Famil
Feb 01, 2017 · nystagmus assessment, and the Dix-Hallpike maneuver for triggered vertigo. C 16 The HINTS (head-impulse, nystagmus, test of skew)