Transcription
Mentally Ill and HomelessNeeds, Gaps, and Project SuggestionsEXHIBIT I MentalHealth;Document consists of 18 pages.Entire document provided.1Due to size limitations, pages provided. A copy of thecomplete document is available through the Research Library(775/684-6827) or e-mail library@lcb.state.nv.us).Meeting Date 10/9/03
Mentally Ill & Homeless Lack Housing Difficult to locate, identify and treat Are not connected to resources provided bythe community that can help themIn addition to All the other challenges of coping with thesymptoms of their mental illness
Some Local Statistics Each year, approximately 10% of the2,000 homeless individuals attending theStand Down for the Homeless have beendiagnosed with a mental illness An average of 14% of them have attemptedsuicide, and another 25% had thought aboutsuicide 1 in 5 report struggling with Depression
More Local Statistics The 1999 UNLV Homeless DemographicSurvey found that– Most homeless people (54.2%) do notregularly “hang out” or travel with anotherperson during the day– 1 in 5 homeless individuals approached for theinterview were too incoherent to continue– In the end, 502 homeless individuals wereinterviewed and their data is presented here
More Local Statistics The 1999 UNLV Homeless DemographicSurvey also found that– 16.9% of the 502 who were coherent enoughto be interviewed had been diagnosed with amental disability– 20.8% said they had received a “dualdiagnosis”– Yet, only 65% are receiving SSI benefits.
Mentally Ill and HomelessPossible Projects
Crisis Response Team
Crisis Response Teams Respond with on-site intervention,assessment and connection to housing andservices – particularly state mental healthservices A central telephone number, provided tobusinesses and residents in high-saturationareas, to dispatch a team within 15 minutes Transportation provided – either byautomobile, taxi, or ambulance, asappropriate
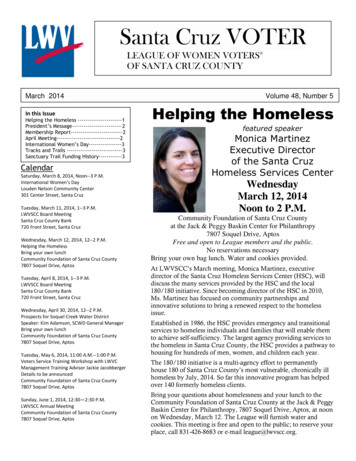
Crisis Response TeamBest Practice: Pine Street Inn’sNBOR program inBoston,Massachusetts 17% of chronic homelessmoved into EmergencyShelter system 16% moved on totransitional settings 10% enrolled in formaltreatment programs 31% successfully livingin permanent housing65% of the 1,022 persons served did not maintain contact; figures above reflect outcomes of the 35% that did maintain contact
Crisis Response TeamBest Practice:Lessons Learned: Pine Street Inn’sNBOR program inBoston,Massachusetts Need on-street nursing(Nurse Practitioner) Nursing liaisons in theshelters Case managementLiaisons at the shelters Taxi vouchers for thosewho could travel on own Hire formerly homeless
SSI Outreach Team
SSI Outreach Team Outreach to “bushes”, but also respond toreferrals from other agencies Pair each client with an advocate to assistwith the complicated application process The advocate is primarily responsible for“managing the paper” Best if can arrange with SSA to offer“presumptive” benefits for up to 6 monthsfor those most visibly disabled
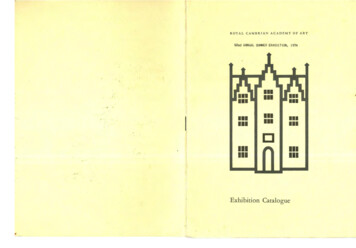
SSI Outreach TeamBest Practice: SSI OutreachProjectBaltimore,Maryland Staffed by a ProjectDirector, 2 Counselors,and 1 Admin Assist Annual Budget ofapproximately 200,000 Serves a minimum of100 homeless personseach year Clients benefit fromlinkages to other countyservices
SSI Outreach TeamBest Practice:Lessons Learned: SSI OutreachProjectBaltimore,Maryland Target severely mentallyill people living on thestreets Require Team to seeeach client within threedays of a phone call,with preference for“home” visits
SSI Outreach TeamBest Practice:Lessons Learned: SSI OutreachProjectBaltimore,Maryland Project Director should belicensed clinical socialworker qualified to preparethe Disability Report forSSA Arrange for “presumptive”eligibility benefits– In 6 years, only 2 of the 450clients “presumed eligible”were denied SSI
Housing First
Housing First Move chronic homeless persons directlyfrom the streets into private market housing Pair each client with an AssertiveCommunity Treatment (ACT) Team todeliver services to the client at least twiceeach month in her/his home Use TBRA or Section 8 to pay for rent Adherence to sobriety rules is not acondition to maintaining housing
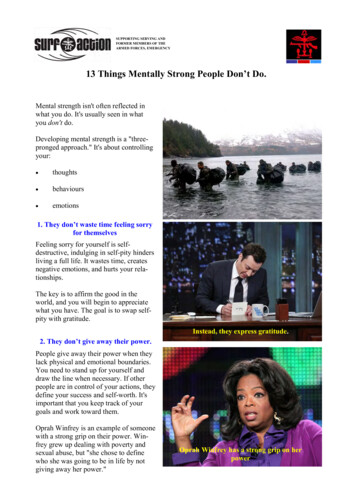
Housing First Serves over 400 peopleannually, at a cost of Pathways to Housingapproximately 20,000 per yrNew York, NY Staffing pattern:Best Practice:––––––4 Housing Counselors5 Team Leaders2 Psychiatrists2 Nurses1 Vocational SpecialistService Coordinators, each witha particular expertise
Housing FirstBest Practice: Pathways to HousingNew York, NY Each ACT Team seesapproximately 70clients ACT Team isresponsible for meetingthe basic needs,enhance the quality oflife, increase socialskills, and increaseemploymentopportunities
Housing FirstBest Practice: Pathways to HousingNew York, NYLessons Learned: Have 2 transitionalapartments for use byclients who haven’t yetfound an apartment of theirown Have HQS Inspectioncapabilities on staff Only Requirements: meettwice each month withACT Team and enroll in aMoney Managementprogram
Housing Resources Tenant-Based RentalAssistance (TBRA)–––––Section 8 vouchersHOMEHOPWASHPS C Partner with nonprofitHousing Developers Build your ownhousing– HOME and LIHTF– Section 811– SHP, S C andSection 8 SRO– Section 515– YouthBuild– CDBG– LoansPlease see hand-out for more details
Creating Homes Initiative
Creating Homes Initiative Capitalize on available housing funds andopportunities to develop and expandpermanent housing options and services forpersons with mental illness Obtain a base incentive amount ( 2million) from the State budget to act asleverage for other sources
Funds Available for CHI Dept. of Mental Healthand DevelopmentalDisabilities HUD Continuum ofCare programs HUD HOME funds HUD Section 811 HUD Section 8Vouchers for Personswith Disabilities HUD Section 8 HUD CDBG Federal Home LoanBank Nevada Low IncomeHousing Tax Credits Local Foundations Fannie Mae Kresge Foundation Robert Wood JohnsonFoundation
Creating Homes Initiative Request that the State’s Housing Division targetits housing development resources for housing forthe mentally ill Create and execute local strategies to expand themenu of needed permanent housing andsupportive service options for each community Have a CHI Task Force or Steering Committeereview, rank and recommend housing proposalsto the Housing Division for funding
Creating Homes Initiative Direct new resources to increasing housingoptions Category changes of current programs orbuildings to permanent housing Utilize non-traditional buildings (churches,downtown hotels, etc.) as permanenthousing options for persons with mentalillness
Creating Homes InitiativeBest Practice: Tennessee Dept ofMental Health andDevelopmentalDisabilitiesCommission Receives annualallocation of 2.5 millionand has leveraged over 29 million in newfederal, other state, andlocal funds to producepermanent housing:supervised and partiallysupervised grouphousing, private/publicmarket rental housing andhomeownership
Creating Homes InitiativeBest Practice: Tennessee Dept ofMental Health andDevelopmentalDisabilitiesCommission Hired 7 RegionalHousing Facilitatorsto work with locallybased CHI TaskForces Goal: 2,005 housingunits by 2005 Accomplishment:1,937 by June 2002
Other Needed Services
Other Needed Services Safe Haven drop-in center for homeless mentallyill–––––No compliance with rules or medication requiredOpen-door policyOvernight accommodations, day sleeping okayNo limits on length of stayFacility design and program goal must be to reducethe intimidating barriers homeless people with severemental illnesses encounter with the care system
Other Needed Services Maintain an ideal number of Licensed ClinicalPsychologists to reduce wait time for diagnosis Significant increases in Nevada’s Intensive CaseManagement services Increased Crisis Observation beds Build a forensic services facility in SouthernNevada — and fully staff it Significant increases in all the other programs ofstate mental health
Other Needed Services Alcohol and Drug Abuse Treatment specializedfor those with co-occurring mental illness Residential treatment settings for clients prone toviolence Medication management and education –including “depot medications” that allow for oneinjection of time-released medication Specialized service for clients with the diagnosisof borderline personality disorder
Other Needed Services More Representative Payee services –particularly specialized for this population Alternatives to acute hospitalization – beavailable to preadmission consultation tocommunity and hospital providers who areconsidering an acute hospital admission Specialized service for clients with thediagnosis of borderline personality disorder
Other Needed Services Continuity of Care – the ongoing relationshipsbetween the client and the psychiatrist and casemanager are particularly important. Increased focus on clients’ family members,friends and other community resources (shelterproviders) as part of treatment. Programs shoulduse the term “partner” rather than “manage” tobuild the trust
Mentally Ill & Homeless Lack Housing Difficult to locate, identify and treat Are not connected to resources provided bythe community that can help themIn addition to All the other challenges of coping with thesymptoms of their mental illness
“presumptive” benefits for up to 6 months for those most visibly disabled . SSI Outreach Team Best Practice: SSI Outreach Project Baltimore, Maryland Staffed by a Project Director, 2 Counselors, and 1 Admin Assist . of border