Transcription
Applications of Dialectical BehaviorTherapy to the Treatment ofTrauma-Related ProblemsAmy W. Wagner, Ph.D.VA Portland Health Care System, Portland DBT Inst.1
My IntentProvide brief overview of DBT Discuss ways in which DBT is relevant to individualswith problems related to traumatic events Practice case formulation and treatment planning forindividuals with complex presentations Introduce a new approach that integrates DBT withProlonged Exposure 2
Existing Treatments for PTSD andRelated Problems Have LimitationsDespite strong empirical support for trauma-processing therapies(e.g., Prolonged Exposure, Cognitive Processing Therapy), their reachis fairly low Many people with BPD or other complex presentations are typicallyexcluded from research on trauma-processing therapies PE and CPT are based on specific set of problems and caseformulation that may not fit many individuals with histories oftrauma Few well-established treatments exist for the array of problemsseen in individuals with histories of repeated traumatic experiences(e.g., “Complex PTSD”) 3
What’s a clinician to do?4From Resick et al. (2012), JTS
DBT is designed for the multi-problemedclient with severe emotion dysregulation. Targetsa wide-range of problems (that overlap withPTSD and most conceptualizations of “complexPTSD”) Basedon empirically-supported principles andinterventions Basedon individualized case formulations Largeand growing empirical support5
DBT Has Strong Research Base DBT has now been evaluated in 30 randomizedcontrolled trials across 19 independent sites in 8 differentcountries with 12 distinct patient populations Adaptations exist for substance use disorders, eatingdisorders, behavior problems in adolescents, incarceratedindividuals with antisocial personality disorder, victims ofdomestic violence, severe shame, and others DBT appears effective for problems related to emotiondysregulation6
Application #1:DBT as stabilization for individualswith complex trauma historiesand/or PTSD(Stage I DBT)7
DBT Stages and TargetsTARGETStage I:Severe Behavioral DyscontrolGOALStability and Behavioral ControlStage II: Quiet DesperationNormative Emotional Experiencing& Expression (Fruzzetti)Stage III: Problems in LivingOrdinary Happiness and UnhappinessStage IV: IncompletenessCapacity for Sustained Joy8
Stage 1 Primary Targets Decrease Life-threatening behaviors Therapy-interfering behaviors Quality-of-life interfering behaviors Increase behavioral skills Mindfulness Interpersonal Effectiveness Emotion Regulation Distress Tolerance Self-Management9
Stage 1 Secondary Targetsself invalidationunrelenting crisisapparent competenceactive passivityinhibited grievingemotional vulnerability10
Treatment of Trauma-Related Problemsin Stage I: StageI targets treated directly (per standard DBT) StageII targets with a “here and now” approachDBT skills to manage DBT skills to engage in trauma-focused treatment Contingency management and stimulus control 11
DBT is a principal-based treatment (thatincludes protocols) 3 main theories guide DBTBehavioral theoryBiosocial theoryDialectical theory Allowsfor ideographic case formulation andtreatment 12Interventions include standard behavioral interventions, DBTskills, acceptance-based strategies, dialectical strategies
Fundamental IrreverenceReciprocalCommunicationConsultation tothe patient13EnvironmentalIntervention
DBT is a behavioral therapy thatincludes validation and dialecticalstrategies and assumes basic deficits inemotion regulation abilities.14
Case Formulation is Key in DBT“a set of hypotheses about the causes, precipitants, andmaintaining influences of a person’s difficulties thathelps you to translate general treatment protocolsinto an individualized treatment plan”15Koerner, K. (2011). Doing Dialectical Behavior Therapy: A Practical Guide.
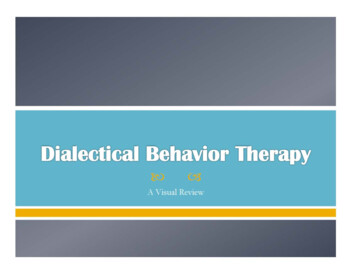
Chain analyses lead to behavioralanalyses which inform case formulation.“What made you moresusceptible? Why this day/time?”What exactly is theproblem behavior(detailed)?“What set this off?When did it start?”“What did you do,feel, think, whathappened next?”17“What happened after?”Koerner, K. (2015)
Look for patterns of controllingvariables.VULNERABILITY ENCES
Sources of Hypotheses aboutControlling Variables Disorder specific mechanisms from literature (e.g.,anxiety sensitivity in panic) Biosocial theory (e.g., emotional dysregulation, dysfunctionalbehavior as problem-solving) Behavioral principles (e.g., skills deficits, conditioning, etc.)Secondary targetsDialectics19Koerner, K. (2011). Doing Dialectical Behavior Therapy: A Practical Guide.
Interventions in DBT target controllingvariables.Does the person have the skill?No:20TEACH SKILLSKoerner, K. (2015).
DBT SkillsBehaviors to IncreaseBehaviors to DecreaseMindfulnessIdentity confusionEmptinessCognitive dysregulation(Dissociative behavior)InterpersonalEffectivenessInterpersonal chaosFears of abandonmentEmotion RegulationLabile affectExcessive anger (shame, fear )Emotional avoidanceDistress ToleranceImpulsivitySuicidal threatsNon-suicidal self-injury
Interventions in DBT target controllingvariables.Does the person have the skill?Yes:What’s getting in the way? Emotions: exposurebased procedures, cue-control Contingencies: contingency management procedures Cognitions: cognitive interventions, wise mind, dialecticalreasoning22Koerner, K. (2015).
Stage I DBT is Effective! But Now What? Studies show reductions in the Stage 1behaviors (self-harm, suicide attempts,psychiatric hospitalizations, substanceuse, eating disordered behavior, andmore).Our clients are still in hell: depression, anxiety,substance use, dissociative behavior, anger, PTSDsymptoms, poor relationships, eating disorderedbehavior, etc.23
Application #2:DBT as treatment for problemsrelated to prolonged and severetrauma and invalidation(Stage II of DBT)24
There is no agreed-upon, defined, or wellevaluated Stage II DBT.25
Neat Work Being Done with Stage II DBT: Martin Bohus, MD—Central Institute of Mental Health,Mannheim, Germany Alan Fruzzetti, Ph.D., University of Nevada, Reno Melanie Harned, Ph.D., University of Washington, Seattle26
As DBT therapists, we know what we need toknow to move forward with Stage II treatment“You had the power all along my dear.”27
As in Stage I, Stage II DBT is principlebased and ideographic.Case formulation is key!28
Case formulation is just as central inStage II DBT Includeshierarchy of targets (based on client goals,severity of problem, functional relationships betweenproblems) Guidedby behavioral, biosocial, and dialecticaltheories Interventionspull from DBT skills, behavioralinterventions, acceptance-based strategies, dialecticalstrategies29
Know What You’re Treating:Targets for Stage IITARGETGOALQuiet DesperationNormative Emotional Experiencing &Expressionintrusive experiencesmindfulness of current experienceavoidance of emotions*capacity for emotional experiencingavoidance of situations/experiencesengagement in meaningful activityemotion dysregulationcapacity for emotional -validation/acceptance*behaviors that function as emotional avoidance30
Behaviors that can function as emotionalavoidance (and also increase suffering): Non-suicidal self-injurySubstance useDissociative behaviorEating disordered behaviorSecondary emotionsJudgmentsIntentional suppressionRestriction of life activitiesFacial expressions/body postureTherapy interfering behavior31
When to Start: Considerations for readiness Client Factors No higher target behavior presentFoundation in behavioral skills (especially ability to tolerate, regulateemotions)Connection to therapistRelative stability in livingVulnerabilities to emotions addressedCommitment to Stage IITherapist/Clinic Factors 32Solid case formulation developedKnowledge/skill in key principles/interventionsSufficient resources to provide adequate treatmentConnection to clientConsult group
Where to Start?1.2.3.4.5.33Develop thorough list of current problems anddiagnosesSelect those that can be conceptualized as related toemotion dysregulation/difficulties with emotionalexperiencingSelect those that are creating the most sufferingcurrently and are consistent with client goalsDevelop thorough and specific behavioral definitions ofkey problemsConsider potential functional relationships betweenproblems (e.g., does the presence of one behaviorincrease the likelihood of another?)
Where to Start?6.7.8.9.10.34Develop a self-monitoring plan (diary card) for currentbehaviors and past high risk behaviorsConduct behavioral analyses of target behavior(s)Consider key interventions requiredConsider your resourcesStay open, flexible to new information!
As in Stage I, Stage II DBT is principlebased and ideographic Guided by behavioral theory Based on bio-social theory Behavioral analyses remain centralBehavioral theory guides assessmentBehavioral interventions based on assessmentAssumes transaction between individual and environment (indevelopment and maintenance of problems)Attention to role of invalidation (in development and maintenance ofproblems)Skills deficits remain a focusAssumes dialectical world view 35Maintains balance of acceptance and changeMindfulness skills strengthened, applied to emotionsPromotes dialectical thinking
Let’s put this into action!36
Case Example “Rhonda” is a 32 year old, divorced female White Army veteran who meetscriteria for BPD, PTSD, and alcohol dependence (in remission for 2months). She has a long-standing history of self-harm behavior, includingcutting and burning, but has not engaged in any self-harm for 3 months. Shehas been in Stage I DBT for the past 6 months.She has a history of sexual and physical abuse perpetrated by her fatherand was sexually assaulted in the military.She has two young children and is currently in a custody battle with her exhusband.She reports frequent memories of her sexual assault from the military andsexual abuse as a child. At times this leads to dissociative behavior,including “spacing out” and losing time for up to an hour. She is veryisolated—not working and only leaving her home to shop or take herchildren to school.37
Stage II Targets for Rhonda intrusive memories sexual assault in the militarychildhood sexual abuse dissociative behavior isolated not workingrarely leaves homeadditional PTSD- and BPD-related problems?38
What else do you need toknow? What’s missing?How would you get it?39
Stage II for Rhonda: Considerations Behavioral descriptions of each problemCurrent precipitants, maintaining factorsPossible relationships between problemsMost problematic for RhondaPriorities for RhondaStaff/clinic resources40
Zeroing In on Interventions: Use diagnostic and self-report measures Self-monitoring: consider how you would modify adiary card to keep track of targets/goals Behavioral analyses remain central Behavioral, biosocial, and dialectical theories guideassessment41
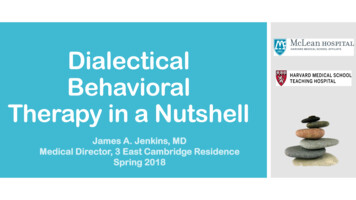
Look for patterns of controllingvariables.VULNERABILITY ENCES
Possible Interventions for Rhonda: DBT-PE Protocol (Harned et al.) Individualized treatment based on assessment of targetbehaviors43
Let’s do a quick self-check: What are the four primary maintaining factors we arelooking for in our chain analyses (hint: they correspond tolearning theory/types of learning)?What are the four primary categories of interventions?44
Key links and interventions from behavioraltheory:Maintaining FactorsInterventionsskills deficits skills trainingcues in the environmentcontingenciescognitive factors remove cue or exposurecontingency managementcognitive interventions45
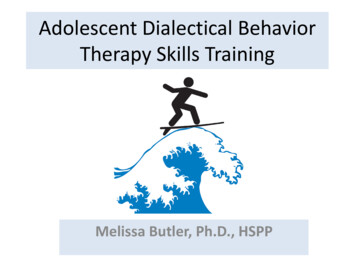
“Rhonda”VULNERABILITYPerceived therapistas upset”I’m screwed up”Began discussing conflictwith partner, anger46High shameBecame unresponsivein sessionReduction of shame
“Rhonda”VULNERABILITYPerceived therapistas upset”I’m screwed up”Began discussing conflictwith partner, anger47High shameBecame unresponsivein sessionReduction of shame
“Rhonda”VULNERABILITYPerceived therapistas upset”I’m screwed up”Began discussing conflictwith partner, anger48High shameBecame unresponsivein sessionReduction of shame
“Rhonda”VULNERABILITYPerceived therapistas upset”I’m screwed up”Began discussing conflictwith partner, anger49High shameBecame unresponsivein sessionReduction of shame
“Rhonda”VULNERABILITYPerceived therapistas upset”I’m screwed up”Began discussing conflictwith partner, anger50High shameBecame unresponsivein sessionReduction of shame
“Rhonda”VULNERABILITYPerceived therapistas upset”I’m screwed up”Began discussing conflictwith partner, anger51High shameBecame unresponsivein sessionReduction of shame
Possible Interventions for Rhonda Let’s assume key links in chain represent common links todysfunctional behavior outside of session too. Need for DBT skills?Self-invalidation?Presence of cues, precipitants?Contingencies?Discuss possible interventions.52
Frequent interventions in Stage II: Exposure Self-validation Mindfulness of emotions Distress tolerance/willingness53
Steps in “Informal” Exposure: Orient to the intervention Present cue Block avoidance (including secondary emotions) Opposite action (do it all the way) Allow for corrective information54
Teaching Self-Validation: Increase awareness of self-invalidationTherapist accurately validates the valid, does not validatethe invalid—and is explicit about thisTherapist titrates use of validation, pulls for more selfvalidationDirect teaching of level 4 and level 5 validationKeep the focus on the primary emotion (Fruzzetti)55
Mindfulness in Stage II: Practice can be longer in duration, more frequent, lessguidedIncrease focus on mindfulness of emotionsFor individuals with histories of trauma continue focus onawareness of physical sensations.Maintain focus on non-judgmental awarenessGenerate, share practices you like!56
Distress Tolerance in Stage II Emphasis on increasing willingness (specifically willingnessto have painful emotions) Discuss research directlyLook for “I can’t” beliefsEngender a “bring it on” attitude (or at least “hold gently”);“willingness with your head and your heart”Mindfulness of physical discomfort as practiceEmphasis on radical acceptance (of current and pastexperiences)57
Modes of Treatment Base this on your case formulation Consider your resources Maintain a consult group!58
Application #3:Treatment of PTSD amongindividuals with severe emotiondysregulation(DBT-PE Protocol for PTSD;Harned, Linehan, et al.)59
Melanie Harned, Ph.D.: DBT-PE For treatment of PTSD among individuals with BPD/severeemotion dysregulation PTSD viewed as quality of life interfering behavior Based on PE for PTSD (Foa et al.) Clients remain in standard DBT and have additional 90”weekly sessions of PE60
Readiness criteria for DBT-PE protocol Notat imminent risk for suicide No life threatening behavior for 2 months Ability to control life threatening behaviors when inthe presence of cues for those behaviors No serious therapy interfering behavior PTSD is highest priority target Ability and willingness to experience intenseemotions without escaping61
Unique Features of DBT-PE Protocol Emphasis on commitment to no life threatening behaviors andworking on behaviors that could interfere with exposureUtilization of Post-Exposure Skills PlanCommon Reactions to Trauma include behaviors related toBPDImaginal exposure also targets experiences of “traumaticinvalidation”In vivo hierarchy includes behaviors that evoke unjustifiedshameExposure Recording Form includes pre and post urges tocommit suicide, self-injure, quit therapy, use substances, statedissociation, levels of specific emotions and radical acceptance62
Unique Features of DBT-PE Protocol Includes more strategies for managing over-engagement anddissociationDBT skills used to “up-regulate” emotions for underengagementContinued use of DBT strategies (validation, dialectical, etc.)More direct cognitive interventions63
Open Trial of DBT PE Protocol (N 13)(Harned, Korslund, Foa, Linehan, 2012) Significant reductions in PTSD Majority no longer met criteria for PTSD No evidence of worsening of suicidal or self-injuriousbehavior, PTSD, treatment drop-out, or use of crisisresources Highly acceptable to clients64
Randomized Controlled Trial, DBT (9)vs.DBT-PE (17); (Harned, Korslund, & Linehan, 2015) Treatment expectancies, satisfaction, and completion didnot differ between conditionsThose receiving DBT-PE had greater reductions in PTSDand doubled remission rates (80% v. 40%)Those who completed DBT-PE were 2.4 times less likelyto attempt suicide and 1.5 times less likely to self-injureDBT-PE lead to greater improvements on all secondaryoutcomes measured: dissociation, trauma-related guiltcognitions, shame, anxiety, depression, and globalfunctioningEffect sizes for all measures were strong for DBT-PE65
Next Steps: Obtain formal training in exposureConsider training in additional (compatible) approaches thataddress the targets and approach in Stage II Have a team meeting Compassion Focused TherapyEmotion Focused TherapyFunctional Analytic PsychotherapyAcceptance and Commitment TherapyMindfulnessTreatment needs in your clinicResources available/neededPlan how you will startEvaluate the impact of what you do!!66
References:Harned, M. S., Korslund, K. E., Foa, E. B. & Linehan, M. M. (2012). Treating PTSD insuicidal and self-injuring women with borderline personality disorder:Development and preliminary evaluation of a Dialectical Behavior TherapyProlonged Exposure Protocol. Behaviour Research and Therapy, 50, 381-386.Harned, M. S., Korslund, K. E., & Linehan, M. M. (2014). A pilot randomizedcontrolled trial of Dialectical Behavior Therapy with and without the DialecticalBehavior Therapy Prolonged Exposure protocol for suicidal and self-injuringwomen with borderline personality disorder and PTSD. Behaviour Research andTherapy, 55, 7-17.Koerner, K. (2011). Doing Dialectical Behavior Therapy: A Practical Guide. New York:Guilford.Linehan, M. (2014). DBT Skills Training Manual, Second Edition. New York: Guilford.Linehan, M. (2014). DBT Skills Training Handouts and Worksheets, Second Edition. NewYork: Guilford.Rizvi, S. L. & Ritschel, L. A. (2014). Mastering the art of chain analysis in dialecticalbehavior therapy. Cognitive and Behavioral Practice, 21, 335-349Wagner, A. W., Rizvi, S. L. & Harned, M. S. (2007). Applications of DialecticalBehavior Therapy to the treatment of complex trauma-related problems: Whenone case formulation does not fit all. Journal of Traumatic Stress, 20, 391-400.67
Stage II DBT Includes hierarchy of targets (based on client goals, severity of problem, functional relationships between problems) Guided by behavioral, biosocial, and dialectical theories Interventions pull from DBT skills, behavioral intervention