Transcription
Spirometry Testing inOccupational HealthProgramsBest Practices forHealthcare ProfessionalsOSHA 3637-03 2013
Occupational Safety and Health Act of 1970“To assure safe and healthful working conditionsfor working men and women; by authorizing enforcementof the standards developed under the Act; by assistingand encouraging the States in their efforts to assuresafe and healthful working conditions; by providing forresearch, information, education, and training in the field ofoccupational safety and health.”Material contained in this publication is in the publicdomain and may be reproduced, fully or partially, withoutpermission. Source credit is requested but not required.This information will be made available to sensoryimpaired individuals upon request.Voice phone: (202) 693-1999;teletypewriter (TTY) number: 1-877-889-5627.This publication provides a general overview of a particularstandards-related topic. This publication does not alter ordetermine compliance responsibilities which are set forthin OSHA standards, and the Occupational Safety and HealthAct. Moreover, because interpretations and enforcementpolicy may change over time, for additional guidance onOSHA compliance requirements, the reader should consultcurrent administrative interpretations and decisions by theOccupational Safety and Health Review Commission andthe courts.OSHA would like to thank the American College ofOccupational and Environmental Medicine (ACOEM) andM.C. Townsend Associates, LLC for their assistance inpreparing this document.Cover photo courtesy of Vitalograph. This image is for informationalpurposes only and does not represent an official OSHA endorsement ofthe products shown or their manufacturer.
Spirometry Testing inOccupational HealthProgramsBest Practices for Healthcare ProfessionalsOccupational Safety and Health AdministrationU.S. Department of LaborOSHA 3637-03 2013
TABLE OF CONTENTS1.0 INTRODUCTION.11.1 SPIROMETRY OVERVIEW.22.0 ACCURATELY MEASURING WORKER LUNG FUNCTION.32.1 PERSONNEL INVOLVED IN SPIROMETRY TESTING.32.2 EQUIPMENT .52.3 CONDUCTING SPIROMETRY TESTS.163.0 INTERPRETING TEST RESULTS.283.1 COMPARING WORKER RESULTS WITH THE NORMAL RANGE(REFERENCE VALUES).283.2 EVALUATING RESULTS OVER TIME.324.0 QUALITY ASSURANCE (QA) REVIEWS.355.0 SPIROMETRY PROCEDURE MANUAL.366.0 RECORDKEEPING.377.0 REFERENCES.38APPENDIX A: NATIONAL HEALTH AND NUTRITION EXAMINATION SURVEY III(NHANES III) REFERENCE VALUES.40APPENDIX B: CHECKLIST FOR SPIROMETRY PROCEDURE MANUAL.54OSHA REGIONAL OFFICES.56HOW TO CONTACT OSHA.57ivO CC U PAT I O N A L S A F E T Y A N D H E A LT H A D M I N I S T R AT I O N
1.0 INTRODUCTIONSpirometry, the most common type of pulmonaryfunction test (PFT), is used to evaluate workerrespiratory health in medical surveillanceprograms and to screen workers for their abilityto perform certain tasks. Spirometry results canplay a central role in decisions about worker jobassignments and personal protective equipment,and in the assessment of exposure-related healtheffects. OSHA standards for asbestos, cadmium,coke oven emissions, and cotton dust requirespirometry testing as part of medical surveillance(see 29 CFR 1910.1001, 1910.1027, 1910.1029, and1910.1043). OSHA standards for formaldehyde andbenzene require pulmonary function testing whenrespiratory protection is used at work (see 29 CFR1910.1048 and 1910.1028).Whether spirometry is conducted to complywith an OSHA regulation or as part of anotherworkplace-mandated program, its value iscompromised when testing is conductedincorrectly, equipment is inaccurate, or resultsare misinterpreted. Technically flawed teststoo often lead to inaccurate interpretations ofworker respiratory health, falsely labeling normalsubjects as “impaired” or impaired subjects as“normal.” Such flawed test results are not onlyuseless but also convey false information whichcould be harmful to workers (1). Too often, thosewho conduct the tests or interpret the results areunaware of the impact of technical pitfalls and ofcurrent spirometry testing recommendations.Because spirometry has become so important inoccupational health practice, OSHA developedthis guidance document to summarize what itregards as the elements of a good occupationalhealth spirometry program. Recommendationsare based on current guidelines from theAmerican Thoracic Society/European RespiratorySociety (ATS/ERS), the American College ofOccupational and Environmental Medicine(ACOEM), and the National Institute forOccupational Safety and Health (NIOSH) (2–8).OSHA’s goal is to provide an update for themedical community on what are the requiredcomponents for valid tests and strategiesfor interpreting results, so that occupationalspirometry tests are useable and of high technicalquality.This document provides a brief overview of theelements of spirometry, followed by specificrecommendations on: (1) accurate measurementof worker lung function (training of personnel,equipment considerations, and spirometry testprocedures); (2) appropriate interpretation ofvalid tests (comparing worker results with normalreference values and evaluating worker resultsover time); (3) Quality Assurance (QA) reviews;and (4) recordkeeping. This document is organizedto permit all readers, regardless of their level ofspirometry experience, to refer immediately tospecific sections of interest.PURPOSE OF THIS GUIDEThis guidance document is intended formedical personnel who oversee worker healthprograms, conduct spirometry tests, and/or interpret spirometry results. The goal ofthe document is to help ensure the collectionof accurate, valid spirometry results thatare interpreted correctly. Such spirometryassessments can be used to make wellinformed decisions about worker respiratoryhealth (including the need for medicalreferrals), and to conduct programs forprevention and early intervention.S P I R O M E T RY T ES T I N G I N O CC U PAT I O N A L H E A LT H P R O G R A M S1
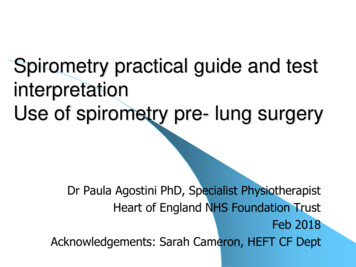
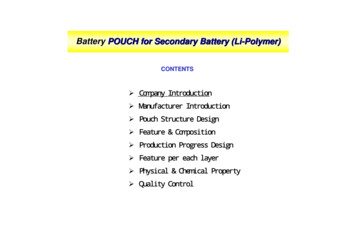
1.1 SPIROMETRY OVERVIEWMeasurements from a worker’s valid spirometrytest are compared with a normal range (i.e.,reference values) and/or with that worker’sbaseline test results to determine whether themeasured volume and flow rate are significantlysmaller or slower than expected. As describedbelow, both the spirometry test itself and thecomparison of results with the normal rangeand/or baseline values should be performedcarefully to guarantee an accurate interpretationof a worker’s respiratory health. This documentfocuses first on accurately measuring worker lungfunction and second on appropriately interpretingtest results. Recommendations are also maderegarding QA review programs and recordkeeping.Some respiratory diseases slow the speed ofexpired air; others reduce the volume of air thatcan be inspired and then exhaled. To detect theseimpairments, spirometry measures the maximalvolume and speed of air that is forcibly exhaledafter taking a maximal inspiration. Forced VitalCapacity (FVC) is defined as total exhaled volumeafter full inspiration. Speed of expired air isdetermined by dividing the volume of air exhaledin the first second, i.e., the Forced ExpiratoryVolume in One Second (FEV1), by the total FVC togive the FEV1/FVC ratio. The time course of theexpiration is recorded as a volume-time curve, andchanges in expiratory flow rate are shown as aflow-volume curve (Figure 1).65FEV1410Flow (L/s)Volume (L)12FVC3210864FVC2012345678910001Time (s)23456Volume (L)Figure 1. Volume-time curve (left) and flow-volume curve (right).Reproduced with permission from ACOEM (5).2O CC U PAT I O N A L S A F E T Y A N D H E A LT H A D M I N I S T R AT I O N
2.0 ACCURATELY MEASURING WORKER LUNG FUNCTIONThree factors work together to produce accurate,meaningful test results: (1) the technician shouldbe well-trained, supervised, and skilled to coachthe worker to record optimal test results; (2)the spirometer should be accurate; and (3) theworker should perform with maximal effort andcooperation. Failure of any one of these factors(e.g., the technician has poor coaching skills,equipment is inaccurate, or a worker does notperform maximal efforts) is likely to produceinaccurate results and lead to an incorrectassessment of respiratory health.to do their job properly, and follow the clinic’sspirometry program guidelines. In some cases,the PLCHP may also conduct spirometry tests. ThePLHCP should be able to: (a) evaluate the technicalquality and validity of spirometry results beforedetermining whether they indicate normal orimpaired respiratory function; (b) communicate themeaning of the test results to the worker who wastested; and (c) evaluate test results for groups ofworkers at a workplace to determine if patterns ofabnormal lung function might indicate a hazardousworkplace exposure.2.1 PERSONNEL INVOLVED INSPIROMETRY TESTING(2) Technicians. Spirometry technicians play acritical role in obtaining accurate and preciseresults. They often have primary responsibilityfor maintaining the spirometer and checking itsaccuracy, preparing and coaching workers duringtesting, and determining whether tests are valid.Motivation to effectively test each worker and theability to recognize and correct testing errors areessential qualities in a technician.Medical personnel who conduct spirometrytests and/or interpret the results should beable to identify technically flawed curves anddistinguish valid from invalid tests. Commonlyused spirometers generate printouts and reports,regardless of whether results are accurate. Simplyreading a spirometer’s interpretation is insufficientand can lead to serious misclassification ofrespiratory health if tests are invalid. Training,knowledge, and understanding of spirometrypitfalls are essential for all medical personnelinvolved in occupational spirometry testingprograms.OSHA states: “The most important qualityof a pulmonary function technician is themotivation to do the very best test on everyemployee. The technician must also be ableto judge the degree of effort and cooperationof the subject. The test results obtained by atechnician who lacks these skills are not onlyuseless, but also convey false informationwhich could be harmful to the employee.” (1)Occupational spirometry tests are performed byhealthcare personnel with varied backgroundsand credentials, ranging from physicians tomedical assistants. Generally, the two types ofpersonnel involved in spirometry testing and theirresponsibilities can be described as follows:2.1.1 TRAINING(1) Physician or Other Licensed Health CareProfessional (PLHCP). In this document, the termPLHCP includes physicians, physician assistants,nurse practitioners, and in some workplaces,registered nurses. PLHCPs often oversee theoccupational spirometry program, supervisetechnicians, clinically interpret spirometryscreening test results, and evaluate groupedspirometry data for medical surveillance purposes.The PLHCP may be responsible for ensuringthat technicians are well-trained and maintaintheir levels of competency, have the resourcesSince clinical training programs do not emphasizerecognition and troubleshooting of spirometrytechnical errors, the National Institute forOccupational Safety and Health (NIOSH) approvescourses that emphasize how to conduct accuratespirometry tests. The 2–3 day courses cover thefundamentals of spirometry and provide handson instruction in small groups with experiencedinstructors. Students must demonstrate theirability to properly prepare for and administer aspirometry test, verify equipment calibration,and recognize unacceptable maneuvers. NIOSH-S P I R O M E T RY T ES T I N G I N O CC U PAT I O N A L H E A LT H P R O G R A M S3
approved spirometry refresher courses are alsoapproved for those experienced with spirometry;both types of courses are listed on the NIOSHweb page at g.html.Some OSHA standards (e.g., asbestos, benzene)require training for spirometry technicianswho are not licensed physicians, and thecotton dust standard specifies that technicianswho are not licensed physicians complete aNIOSH-approved course (see 29 CFR 1910.1001,1910.1028, and 1910.1043). In addition to theseregulatory requirements, OSHA recommendsthat all technicians and other persons conductingoccupational spirometry tests obtain certificationby completing a NIOSH-approved course andmaintain that certification by periodically takingrefresher courses.Since occupational spirometry technicians oftenperform spirometry tests as only one of manyclinical responsibilities, supervisors and directorsof spirometry programs should also understandthe elements of valid tests and be able to recognizeflawed results. Such oversight permits problems tobe corrected quickly and tests to be repeated whenneeded. So that PLHCPs can perform this oversightfunction, OSHA recommends that supervisorsand/or interpreters of test results also complete aNIOSH-approved spirometry course or equivalenttraining that emphasizes recognition and troubleshooting of technical errors and the interpretationof spirometry results.4Certificates of successful course completionare issued to individual technicians who havesuccessfully completed a NIOSH-approvedcourse. Institutions or medical practices cannotbe “NIOSH-approved” for spirometry testingand the courses are not designed to trainmedical personnel who subsequently train theirstaff, unlike some other medical skill trainingcourses. Since each technician who will conductoccupational spirometry tests should completea NIOSH-approved course, OSHA recommendsthat program directors identify a limited numberof technicians to perform spirometry tests andhave them trained, rather than allowing untrainedemployees to perform the tests. As the designatedtechnicians become more skillful at performingspirometry tests with increasing experience,the program’s overall test quality generally willimprove.OSHA recommends that all personsconducting occupational spirometry testingsuccessfully complete an initial NIOSHapproved spirometry course and maintain thatcertification over time. Some OSHA standardsspecifically require that health personnelwho are not licensed physicians complete aspirometry training course if they test workerscovered under those standards.O CC U PAT I O N A L S A F E T Y A N D H E A LT H A D M I N I S T R AT I O N
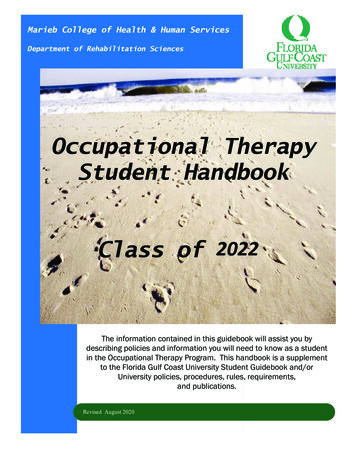
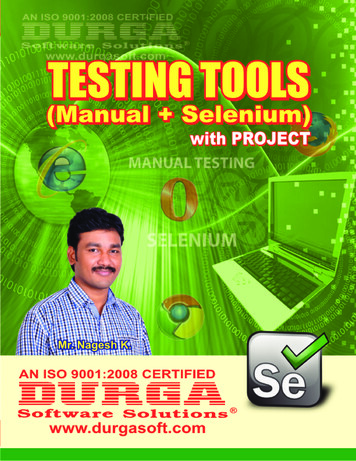
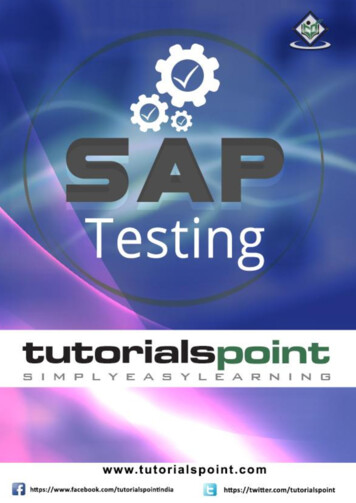
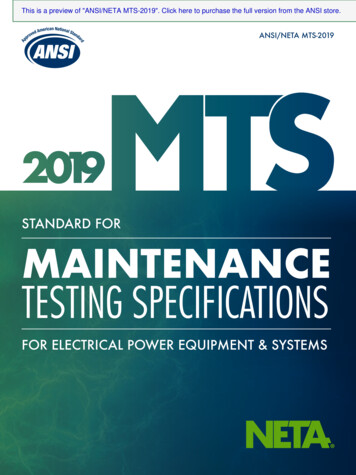
2.2 EQUIPMENT2.2.1 SELECTING A SPIROMETERTypes of spirometers. Spirometry tests areperformed on volume- and flow-type spirometers(Figures 2 and 3). Volume-type spirometersaccumulate air (Figure 2) and directly measurethe worker’s volume of exhaled air. In contrast,flow-type spirometers (Figure 3) measure thespeed of exhaled air and integrate those speedsto obtain volumes of exhaled air. Both types ofspirometers can display the volume-time andflow-volume curves shown in Figure 1, and bothshould meet the spirometer recommendationsdiscussed below and summarized in the text boxon OSHA’s recommendations for newly-purchasedspirometers.Figure 2. Example of a volume spirometer with real-time display.Image courtesy of Morgan Scientific, Inc. These images are for informational purposes only and donot represent an official OSHA endorsement of the product shown or their manufacturer.Figure 3. Example of a flow spirometersensor with mouthpiece, filter, andreal-time display.Image courtesy of Vitalograph. Thisimage is for informational purposesonly and does not represent an officialOSHA endorsement of the productsshown or their manufacturer.S P I R O M E T RY T ES T I N G I N O CC U PAT I O N A L H E A LT H P R O G R A M S5
Accuracy and Precision. To be useful inGraphical Displays. Spirometers used foroccupational health programs, spirometry testresults should be accurate, i.e., free from errors.For example, if 3 liters (L) of air are put into aspirometer, the result should be recorded as 3 L.The results should also be precise, or repeatable,e.g., if 3 L of air are put into a spirometer severaltimes, it should be recorded repeatedly as 3 L.Results that are accurate and precise can becompared across different settings and fromone time to another (8). Minimum standardsfor spirometer accuracy, precision, range ofmeasurements, and other operating characteristicshave been specified by the ATS/ERS (3) and theInternational Organization for Standardization (9).occupational testing should have real-timedisplays, showing curves while the test isbeing performed, that are large enough to beviewed easily. By observing real-time displaysof both flow-volume and volume-time curves,the technician can judge the worker’s effort andprovide optimal coaching. Since the flow-volumedisplay emphasizes the beginning of expiration,it helps technicians detect problems early in themaneuver. In contrast, the volume-time displayclearly shows the end of the maneuver and helpstechnicians coach workers to record completeexpirations. Spirometers should also includeboth flow-volume and volume-time curves intheir reports of test results to assist PLHCPsin interpreting test results. Reports includingadequately sized flow-volume and volume-timegraphs will help PLHCPs clearly see problems inthe early or late stages of the maneuver.Validation Testing. Independent testinglaboratories and some manufacturers performvalidation testing to evaluate a prototypespirometer’s accuracy and precision underlaboratory conditions. Validation testing byindependent laboratories is preferred but is notalways possible. Before purchasing a spirometer,OSHA recommends that users obtain writtenverification from the manufacturer that a prototypeof that spirometer was tested and met at least theATS/ERS minimum specifications for accuracy andprecision.However, when the spirometer will be used toevaluate changes in lung function over time, it isalso recommended that medical personnel select aspirometer that is even more accurate and precisethan the minimum standards (see section 3.2 onEvaluating Results Over Time).6However, medical personnel should note thatmanufacturer claims that a spirometer meets ATS/ERS accuracy and precision recommendationsmay not mean that the display and graph sizes areadequate, since these aspects are not evaluatedduring validation testing. The recommendedminimum sizes for real-time spirometer displaysand spirometry report graphs are shown in Figures4a and 4b.O CC U PAT I O N A L S A F E T Y A N D H E A LT H A D M I N I S T R AT I O N
FlowFlowFlow(L/s)(L/s)(L/s)VolumeVolumeVolume(L) 754643532421310200100011 22 33 44 55 66 77 88VolumeVolume (L)(L)1 2 3 4 5 6 7 8Volume (L)11 22 33 44 55 66 77 88 99 1010 1111 1212 1313 1414 1515TimeTime (s)(s)1 2 3 4 5 6 7 8 9 10 11 12 13 14 15Time (s)5 VolumeVolume ScaleScale 5 mm/Lmm/L FlowScale 2.5mm/L/s2.5 mm/L/sFlow Scale 5 VolumeTimeScalemm/sScale5 mm/LTime Scale 5 mm/s *CompliesFlow Scale 2.5mm/L/s*ComplieswithANSIISOwith ANSIISO 2567225672 aspectaspect ratioratio requirements.requirements.5 mm/s Time Scale *Complies with ANSI ISO 25672 aspect ratio requirements.Figure 4a – ATS/ERS recommended minimum size for real-time spirometer displaysduring testing.*Reproduced with permission from ACOEM (5).S P I R O M E T RY T ES T I N G I N O CC U PAT I O N A L H E A LT H P R O G R A M S7
Flow (L/s)87VolumeVolume(L) (L)766554Volume 01008043322110000121110987654321010234567878Volume (L)81721623545678Volume34 (L)56Volume (L)7843210012345691011 12 13 14 15Time (s)1234567891011 12 13 14 15123456 Time7 8(s) 91011 12 13 14 15Time (s)10 mm/L Volume Scale 5 mm/L/s Flow Scale 10 mm/s Time Scale *Complies with ANSI ISO 25672 aspect ratio requirements.10 mm/L Volume Scale 5 mm/L/s Flow Scale 10Scale mm/L10 VolumeTime Scale mm/sFigure 4b – ATS/ERSrecommendedsize for spirometry test report graphic displays.*5ANSI Flow Scale mm/L/s*ComplieswithISO 25672 aspect ratio requirements.Reproduced with permission from ACOEM (5).10 mm/s Time Scale *Complies with ANSI ISO 25672 aspect ratio requirements.8O CC U PAT I O N A L S A F E T Y A N D H E A LT H A D M I N I S T R AT I O N
Data and Curve Storage and Recall. Otherimportant spirometer aspects relate to informationsaved from a test session, flexibility of spirometersoftware in permitting editing of earlier effortswithin a test, and choice of output to be includedOSHA recommends that newlypurchased spirometers have thefollowing features:1.2.3.4.5.6.7.8.9.10.11.12.13.Accuracy and precision meet minimumATS/ERS standards in all cases, andexceed the standards if used to evaluatechanges over time in an individual’s lungfunction;Capacity to save and recall all curves andresults from up to 8 maneuvers;Ability to electronically save curves andresults for simplified future recall andreview of test quality and results;Capability to edit and delete previouserroneous curves within a test session;Displays as large as those shown in Figure4a of both flow-volume and volume-timecurves as the test is being performed topermit technicians to fully evaluate testquality before deciding whether to save aneffort;Automatic calculation and saving ofquality control aids, to help with, but notreplace, visual evaluation of test quality bywell-informed personnel;Display of all data and curves as large asthose shown in Figure 4b in the report;Interpretation of largest FVC and FEV1,even if they occur on different curves;Identification of the reference values (e.g.,Hankinson 1999) used in the report;Display of both the predicted values andlower limits of normal (LLN), discussedbelow, in the report;Display of the FVC and FEV1 repeatabilityin the report;A dedicated “calibration check” routine,discussed below, on the spirometer menu;andDisplay of last calibration check date oneach report.in reports of test results. Poor performance on anyof these features can significantly impact the easewith which personnel can conduct occupationalspirometry tests and interpret their results.2.2.2 CHECKING SPIROMETER CALIBRATIONWhen the spirometer is in use, techniciansshould verify its accuracy by frequently checkingits calibration and performing maintenanceprocedures at regular intervals. An inaccuratespirometer can produce falsely reduced orelevated worker test results. Such inaccuracies arenot always obvious on visual inspection of the testcurves. Frequent calibration checks allow for earlyidentification of equipment problems, avoidingweeks or months of reporting incorrect values.Calibration checks should be performed in theenvironment in which workers will be tested, andshould be conducted: At least daily when workers are to be tested;Whenever the equipment is changed orrelocated; andBefore the first test and at least every 4 hourson days when large numbers of tests areconducted; this will prevent an undetectedproblem from invalidating large numbers oftest results.For many models of spirometers, the calibrationis checked but cannot be adjusted by the user.If these spirometers become inaccurate andrepeatedly fail their calibration checks, andthere are no obvious mechanical causes for theinaccuracy, they must be recalibrated by themanufacturer. However, other spirometer modelsare recalibrated regularly by the technician,who must carefully follow the manufacturer’sinstructions. After recalibrating such spirometers,technicians should then perform the calibrationchecks described below. Technicians shoulduse spirometer software programs designed forcalibration checks whenever possible.S P I R O M E T RY T ES T I N G I N O CC U PAT I O N A L H E A LT H P R O G R A M S9
Failure to pass all spirometer checks indicatesthat workers should not be tested until thecause of failure is identified and corrected,and the spirometer passes all of its calibrationchecks.Checks of volume spirometers differ from checksof flow-type spirometers since the goal of thechecks is to reveal specific problems unique toeach type of equipment.Volume-type spirometer calibration checks: Thefirst daily check for a volume spirometer is todetermine whether it is airtight. Leaks can developin the hose, the spirometer itself, or connectionsand seals when spirometers are disassembledfor cleaning or when hoses are changed betweenworkers being tested. Small but problematicleaks cannot be detected by inspection alone, sotesting for leaks should be conducted daily andwhen hoses are changed. To test for leaks, injectabout 3 L of air into the spirometer and apply asmall positive pressure (as recommended by themanufacturer) for one minute while the spirometeroutlet (i.e., end of the breathing hose) is blocked.A volume loss of more than 0.03 L/min., i.e., 30milliliters/minute (ml/min.), indicates a leak thatshould be corrected before testing workers.After verifying that there are no leaks, thespirometer’s accuracy is checked by injecting3.00 L of air from a calibration syringe. If thespirometer’s recorded volume is within 3.5% ofthe injected 3 L, or 2.90–3.10 L, the spirometer isacceptably accurate.Volume linearity should be checked quarterly.Volume linearity evaluates whether the spirometeris accurate, not just from 0–3 L, as tested daily,but also across its entire volume range. Accuracyin volume linearity is important when workerswith large lung volumes are tested. To test forvolume linearity, air is manually drawn into thespirometer and its volume is recorded. Then, a 3-Lvolume of air is injected with a calibration syringeto determine whether the spirometer’s recordedvolume increases by 3 L.10For example, if 3 L of air from a calibration syringeare injected into a spirometer that already contains2 L of air, the spirometer’s recorded volume shouldincrease to 5 L. If the spirometer already contains 4L of air, injecting an additional 3 L should increasethe spirometer’s recorded volume to 7 L. Volumelinearity can be checked in three steps, e.g.,starting with 0, 2, and 4 L already in the spirometerbefore using the syringe to inject an additional 3L of air. Volume linearity can also be checked inmore detail, e.g., starting with 0, 1, 2, 3, 4, and 5 Lof air in the spirometer and then using a syringeto inject an additional 3 L of air each time. If thespirometer’s recorded volume increases by 3.5%of 3 L, or 2.90–3.10 L in response to each injection,regardless of the starting volume of air in thespirometer, the spirometer is accurate across itsentire range and it passes its linearity check.If a chart drive is used, the speed of the chart driveshould also be checked quarterly. To do this, checkthat the pen takes 10 seconds (s) 2% or 9.8–10.2 sto traverse a strip of chart paper that is marked as10 s in length.Flow-type spirometer calibration checks: Ona daily basis, check the calibration of flowtype spirometers by injecting 3 L of air from acalibration syringe at three different speeds. Thesyringe should be emptied once in approximately0.5 s (6 L/s), once in 3 s (1 L/s), and once in 6 s(0.5 L/s). If the spirometer has no time scale, usea clock or watch to gauge the speed of injection.(If needed, count “one-one-thousand, two-onethousand” etc., while emptying the syringe, togauge the speed of emptying.) In response to eachinjection, the spirometer should read within /- 3.5percent of 3 L, or 2.90–3.10 L. Failure to recorda value in this range at even one of the speedsindicates that the injection should be repeated,and the cause of the incorrect value should beidentified and repaired. Often the 6-secondinjection detects problems with loose connections,aging parts, and sensor problems. Failure at anyspeed indicates that spirometry testing shouldnot be performed using the spirometer untilcorrections are made and all speeds are accurate.If using disposable sensors, a new sensor shouldbe used for each day’s calibration check sinceaccuracy of sensors can vary within and betweenO CC U PAT I O N A L S A F E T Y A N D H E A LT H A D M I N I S T R AT I O N
batches. Ideally, the calibration check should beperformed with the same sensor that each workerwill use, but this is often not possible because oftime constraints.Daily Calibration ChecksVolume Spirometers*:1.Check that there are no leaks causing anair loss 0.030 L/min. (30 ml/min.).2. Inject 3 L air and verify that the recordedvalue is between 2.90 and 3.10 L.*Quarterly checks are also needed for volumespirometers – see text for details.Flow Spirometers:1.Inject 3 L air at three speeds (takingapproximately 0.5 s, 3 s, and 6 s)
accuracy, preparing and coaching workers during testing, and determining whether tests are valid. Motivation to effectively test each worker and the ability to recognize and correct testing errors are essential qualities in a technician. OSHA states: “The most im