Transcription
Emergency Managementin Neurocritical Care(NEUROLOGY IN PRACTICE SERIES)NEUROLOGY IN PRACTICEEDITED BYSeries editors Robert A. Gross & Jonathan W. MinkEdward M. Manno, MD, FCCM, FAAN, FAHA, Head, Neurological Intensive Care Unit, Cleveland Clinic,Cleveland, OH, USAAcute neurological illness is traumatic for patients and their families. Physicians caring forthese patients are often under great distress and need to rapidly assess the situation to allowappropriate stabilization and management.Emergency Management in Neurocritical Care gives you the tools you need to perform underpressure in the neurocritical or emergency care unit. The no-nonsense approach correspondsto the attitude needed in both acute emergencies and in the neurocritical care unit. Packedwith handy tips to improve your care of patients, and written by internationally renownedexperts, the book covers: Acute Management of Neurological EmergenciesCerebrovascular Critical CareInfections of the Nervous SystemNeuromuscular Complications Encountered in the Intensive Care UnitNeurological Complications and Consultations in General Intensive Care UnitsAcute Neuroimaging and Neuromonitoring in Neurocritical CareClinical in approach, practical in execution, Emergency Management in Neurocritical Care willhelp you perform better in pressure situations.NEUROLOGY IN PRACTICES E R I E S E D I TO R SRobert A. Gross, MD, PhD, Department of Neurology, University of Rochester Medical Center, Rochester, NY, USAJonathan W. Mink, MD, PhD, Department of Neurology, University of Rochester Medical Center, Rochester, NY, USA Algorithms and guidelines where they are appropriate‘Tips and Tricks’ boxes – hints on improving outcomes‘Caution’ warning boxes – hints on avoiding complications‘Science Revisited’ – a quick reminder of the basic science principlesSummaries of key evidence and suggestions for further readingMannoThe Neurology in Practice series provides clinical ‘in the office’ or ‘at the bedside’ guides to effective patient care forneurologists. The tone is practical, not academic, with authors offering guidance on what might be done and whatshould be avoided. The books are informed by evidence-based practice and feature:Emergency Management in Neurocritical CareRapid response, assessment and management are crucial forneurocritical situationsEmergency Managementin Neurocritical CareEdited byEdward M. Manno
NEUROLOGY IN PRACTICE:SERIES EDITORS: ROBERT A. GROSS, DEPARTMENT OF NEUROLOGY, UNIVERSITY OF ROCHESTER MEDICAL CENTER, ROCHESTER, NY, USAJONATHAN W. MINK, DEPARTMENT OF NEUROLOGY, UNIVERSITY OF ROCHESTER MEDICAL CENTER, ROCHESTER, NY, USAEmergency Management inNeurocritical CareEDITED BYEDWARD M. MANNOMD, FCCM, FAAN, FAHAHead, Neurological Intensive Care UnitCleveland ClinicCleveland, OH, USA
This edition first published 2012, Ó 2012 by John Wiley & Sons, Ltd.Wiley-Blackwell is an imprint of John Wiley & Sons, formed by the merger of Wiley’s globalScientific, Technical and Medical business with Blackwell Publishing.Registered office:John Wiley & Sons, Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UKEditorial offices:9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USAFor details of our global editorial offices, for customer services and for information about how to applyfor permission to reuse the copyright material in this book please see our website atwww.wiley.com/wiley-blackwellThe right of the author to be identified as the author of this work has been asserted in accordancewith the UK Copyright, Designs and Patents Act 1988.All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted,in any form or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permittedby the UK Copyright, Designs and Patents Act 1988, without the prior permission of the publisher.Designations used by companies to distinguish their products are often claimed as trademarks. All brandnames and product names used in this book are trade names, service marks, trademarks or registeredtrademarks of their respective owners. The publisher is not associated with any product or vendor mentionedin this book. This publication is designed to provide accurate and authoritative information in regard to thesubject matter covered. It is sold on the understanding that the publisher is not engaged in renderingprofessional services. If professional advice or other expert assistance is required, the services of acompetent professional should be sought.The contents of this work are intended to further general scientific research, understanding, and discussiononly and are not intended and should not be relied upon as recommending or promoting a specific method, diagnosis,or treatment by physicians for any particular patient. The publisher and the author make no representations orwarranties with respect to the accuracy or completeness of the contents of this work and specifically disclaim allwarranties, including without limitation any implied warranties of fitness for a particular purpose. In view of ongoingresearch, equipment modifications, changes in governmental regulations, and the constant flow of informationrelating to the use of medicines, equipment, and devices, the reader is urged to review and evaluate theinformation provided in the package insert or instructions for each medicine, equipment, or device for, amongother things, any changes in the instructions or indication of usage and for added warnings and precautions.Readers should consult with a specialist where appropriate. The fact that an organization or Website is referredto in this work as a citation and/or a potential source of further information does not mean that the authoror the publisher endorses the information the organization or Website may provide or recommendations it maymake. Further, readers should be aware that Internet Websites listed in this work may have changed ordisappeared between when this work was written and when it is read. No warranty may be created or extendedby any promotional statements for this work. Neither the publisher nor the author shall be liable for anydamages arising herefrom.Library of Congress Cataloging-in-Publication DataEmergency management in neurocritical care / edited by Edward M. Manno.p. ; cm.Includes bibliographical references and index.ISBN 978-0-470-65473-6 (pbk. : alk. paper)I. Manno, Edward M.[DNLM: 1. Central Nervous System Diseases–therapy. 2. Emergencies. 3.Care–methods. 4. Intensive Care Units. WL 301]Critical616.80 0425–dc232012002556A catalogue record for this book is available from the British Library.Wiley also publishes its books in a variety of electronic formats. Some content that appears in print maynot be available in electronic books.Set in 8.75/11.75 pt Utopia by Thomson Digital, Noida, India12012
ContentsList of ContributorsSeries ForewordPrefaceviviiiixPART I: ACUTE MANAGEMENT OF NEUROLOGICAL EMERGENCIES1 Hypertensive Emergency3Laurie McWilliams2 Airway Management in the Neurological and Neurosurgical Patient12Michael J. Souter3 Traumatic Brain Injury and Intracranial Hypertension21Iain J. McCullagh and Peter J.D. Andrews4 Critical Care Management of Acute Spinal Cord Injury32Edward M. Manno5 Subarachnoid Hemorrhage37Muhammad A. Taqi and Michel T. Torbey6 Acute Management of Cerebral Ischemia45Leonid Groysman and Gene Sung7 Neurocritical Care of Intracerebral Hemorrhage55James M. Gebel Jr8 Acute Management of Status Epilepticus63Jan ClaassenPART II: CEREBROVASCULAR CRITICAL CARE9 Post-procedural Management of Patients with Aneurysmal SubarachnoidHemorrhage73Tomoko Rie Sampson and Michael N. Diringer10 Care of the Neurointerventional Patient in the Neurointensive Care Unit84Rishi Guptaiii
iv . Contents11 New Treatment Strategies in the Management of Large HemisphericStrokes and Intracerebral Hemorrhages92Edward M. Manno12 Presentation and Management of Acute Cerebral Venous Thrombosis99Patrı cia Canhão and José M. FerroPART III: INFECTIONS OF THE NERVOUS SYSTEM13 Infections in the Neurocritical Care Unit111Denise H. Rhoney, Karen J. McAllen, and Dennis Parker14 Diagnosis and Management of Bacterial and Viral Meningitis123Maxwell S. Damian15 Encephalitis: Presentation and Management132Ali E. Elsayed and Barnett R. NathanPART IV: NEUROMUSCULAR COMPLICATIONS ENCOUNTERED IN THE INTENSIVE CARE UNIT16 Practical Management of Guillain–Barré Syndrome and Myasthenic Crisis143Alejandro A. RabinsteinPART V: NEUROLOGICAL COMPLICATIONS AND CONSULTATIONS IN GENERAL INTENSIVE CARE UNITS17 Metabolic Encephalopathies155Edward M. Manno18 Delirium and Sedation in the ICU162Jennifer A. Frontera19 Neurologic Complications of Cardiac Surgery174Cathy Sila20 Neurological Complications of Medical Illness: Critical IllnessNeuropathy and Myopathy182Edward M. Manno21 Hypothermia: Application and Use in Neurocritical Care188Edward M. Manno22 Etiologies of Posterior Reversible Encephalopathy Syndrome and Formsof Osmotic Demyelination SyndromeJ. Javier Provencio197
Contents . vPART VI: ACUTE NEUROIMAGING AND NEUROMONITORING IN NEUROCRITICAL CARE23 Application of MR Diffusion, CT Angiography and Perfusion Imagingin Stroke Neurocritical Care207Carlos Leiva-Salinas, Wade Smith and Max Wintermark24 Advanced Monitoring of Brain Oxygenation and Metabolism214Bharath R. Naravetla and J. Claude Hemphill IIIIndexThe color plate can be found facing page 54.225
ContributorsPeter J.D. Andrews, MD, MB, ChB, FRCACentre for Clinical Brain SciencesUniversity of EdinburghEdinburgh, UK o, MD, PhDPatrı́cia CanhaDepartment of NeurosciencesServiço de NeurologiaHospital de Santa MariaUniversity of LisbonLisboa, PortugalJan Claassen MD, PhDDivision of Neurocritical Care andthe Comprehensive Epilepsy CenterDepartment of NeurologyColumbia UniversityNew York, NY, USAMaxwell S. Damian, MD, PhDDepartment of Neurology andthe Neurocritical Care UnitCambridge University HospitalsCambridge, UKMichael N. Diringer, MDNeurology/Neurosurgery IntensiveCare UnitDepartment of Neurology andNeurological SurgeryWashington University Schoolof MedicineSaint Louis, MO, USAAli E. Elsayed, MDMountainside HospitalMontclaire, NJ, USA M. Ferro, MD, PhDJoseDepartment of NeurosciencesServiço de NeurologiaHospital de Santa MariaUniversity of LisbonLisboa, PortugalviJennifer A. Frontera, MDNeuroscience Intensive Care UnitDepartments of Neurosurgery and NeurologyMount Sinai School of MedicineNew York, NY, USAJames M. Gebel, Jr, MD, MS, FAHACerebrovascular CenterCleveland ClinicCleveland, OH, USALeonid Groysman, MDNeurocritical Care and Stroke DivisionUniversity of Southern CaliforniaLos Angeles, CA, USARishi Gupta, MDDepartment of Neurology, Neurosurgeryand RadiologyEmory University School of MedicineMarcus Stroke and Neuroscience CenterGrady Memorial HospitalAtlanta, GA, USAJ. Claude Hemphill III, MD, MASDepartment of NeurologyUniversity of CaliforniaSan Francisco, CA, USACarlos Leiva-Salinas, MDDepartment of RadiologyNeuroradiology DivisionUniversity of VirginiaCharlottesville, VA, USAKaren J. McAllen, Pharm.DDepartment of Pharmacy ServicesSpectrum Health HospitalsGrand Rapids, MI, USAIain J. McCullagh, MBChB, FRCADepartment of Anaesthesia, Critical Careand Pain ManagementUniversity of EdinburghEdinburgh, UK
Contributors . viiEdward M. Manno, MD, FCCM,FAAN, FAHANeurological Intensive Care UnitCleveland ClinicCleveland, OH, USALaurie McWilliams, MDNeurocritical Care UnitCerebrovascular CenterDepartment of Neurology and NeurosurgeryCleveland clinicCleveland, OH, USABharath R. Naravetla, MDDepartment of NeurologyNeurovascular ServiceUniversity of California, San FranciscoSan Francisco, CA, USABartnett R. Nathan, MDDepartments of Neurology and InternalMedicineNeuroCritical Care and NeuroInfectiousDiseaseUniversity of VirginiaCharlottesville, VA, USADennis Parker, Jr, Pharm.DEugene Applebaum College ofPharmacy & Health SciencesWayne State UniversityDetroit, MI, USAJ. Javier Provencio, MDCerebrovascular CenterCleveland ClinicCleveland, OH, USAAlejandro A. Rabinstein, MDDepartment of NeurologyMayo Clinic College of MedicineRochester, MN, USADenise H. Rhoney, Pharm.D,FCCP, FCCMEugene Applebaum College of Pharmacy &Health SciencesWayne State UniversityDetroit, MI, USATomoko Rie Sampson, MD, MPHNeurology/Neurosurgery Intensive Care UnitDepartment of Neurology and NeurologicalSurgeryWashington University School of MedicineSaint Louis, MO, USACathy Sila, MDDepartment of NeurologyCase Western Reserve UniversitySchool of Medicineand Stroke & Cerebrovascular Center,Neurological InstituteUniversity Hospitals–Case Medical CenterCleveland, OH, USAWade Smith, MD, PhDDepartment of NeurologyUniversity of CaliforniaSan Francisco, CA, USAMichael J. Souter, MB, ChB, FRCADepartment of Anesthesiology & Pain Medicine;and Department of Neurological SurgeryUniversity of Washington;Department of AnesthesiologyHarborview Medical CenterSeattle, WA, USAGene Sung, MD, MPHNeurocritical Care and Stroke DivisionUniversity of Southern CaliforniaLos Angeles, CA, USAMuhammad A. Taqui, MDDepartment of Neurology and NeurosurgeryThe Ohio State UniversityColumbus, OH, USAMichel T. Torbey, MD, MPH, FAHA, FCCMDepartment of Neurology and NeurosurgeryThe Ohio State UniversityColumbus, OH, USAMax Wintermark MDDepartment of RadiologyNeuroradiology DivisionUniversity of VirginiaCharlottesville, VA, USA
Series ForewordThe genesis for this book series started with theproposition that, increasingly, physicians wantdirect, useful information to help them in clinicalcare. Textbooks, while comprehensive, are usefulprimarily as detailed reference works but posechallenges for uses at the point of care. By contrast, more outline-type references often leaveout the “hows and whys” – pathophysiology,pharmacology – that form the basis of management decisions. Our goal for this series is topresent books, covering most areas of neurology,that provide enough background information toallow the reader to feel comfortable, but not somuch as to be overwhelming; and to associatethat with practical advice from experts aboutcare, combining the growing evidence base withbest practices.Our series will encompass various aspects ofneurology, with topics and the specific contentchosen to be accessible and useful.Chapters cover critical information that willinform the reader of the disease processes andmechanisms as a prelude to treatment planning. Algorithms and guidelines are presented,when appropriate. “Tips & Tricks” boxes provide expert suggestions, while other boxespresent cautions and warnings to avoid pitfalls. Finally, we provide “Science Revisited”sections that review the most important andrelevant science background material, andviii“Bibliography” sections that guide the readerto additional material.We welcome feedback. As additional volumesare added to the series, we hope to refine thecontent and format so that our readers will bebest served.Our thanks, appreciation, and respect go out toour editors and their contributors, who conceivedand refined the content for each volume, assuringa high-quality, practical approach to neurologicalconditions and their treatment.Our thanks also go to our mentors and students(past, present, and future), who have challengedand delighted us; to our book editors and theircontributors, who were willing to take on additional work for an educational goal; and to ourpublisher, Martin Sugden, for his ideas and support for wonderful discussions and commiseration over baseball and soccer teams that mightnot quite have lived up to expectations. We wouldlike to dedicate the series to Marsha, Jake andDan; and to Janet, Laura and David. And also toSteven R. Schwid, MD, our friend and colleague,whose ideas helped to shape this project andwhose humor brightened our lives, but he couldnot complete this goal with us.Robert A. GrossJonathan W. MinkRochester, July 2011
PrefaceSince its beginning in the early 1980s the field ofneurocritical care has expanded at a dramatic rate.In the last decade there has been the developmentof an international society with over 1000 members, a specialized journal with a growing impactfactor, accredited fellowship programs, and aboard certification process through the UnitedCouncil of Neurological Subspecialties. To datethere are close to 100 neurocritical care units in theUnited States, a similar number in Europe, and agrowing presence in South America and Asia. Theinclusion of a textbook of Neurocritical Care in theNeurology in Practice series is a testimony to thefield’s growing influence.The rapid growth of neurocritical care has encouraged a commensurate growth of literature inthe field. Interestingly, this has mostly taken theform of single author texts or handbooks primarilydesigned to disseminate information quickly andsystematically to keep pace with this growing field.This book, Emergency Management in Neurocritical Care is the first multi-authored textbookin the field since the first text, Neurological andNeurosurgical Intensive Care, was edited by AllanRopper and Sean Kennedy in 1983. The primaryaim is to provide a comprehensive guide to themanagement of acutely ill neurological or neurosurgical patients wherever they may be locatedin the hospital. The scope of the book will includebasic principles in emergency neurology andcritical care, which will review the underlyingbasic science and cerebrovascular physiology ofthe critically ill neurological patient. Later sections will focus more on the critical aspects of theneurologically ill. Specific sections dedicated tocerebrovascular disease, neuromuscular disor-ders, epilepsy, and neurological consultations ingeneral intensive care unit are included. A finalsection on neuroimaging and neuromonitoringreflects the growing reliance on technology inneurological critical care.The chapters are written by experts in theirrespective areas and represent a worldwide distribution of multidisciplinary authors. The bookcontains more detailed information than a handbook, but is presented in a concise and userfriendly manner to serve as a quick referencewhen needed. The “Tips & Tricks” and “ScienceRevisited” sections are designed to increase thereadability of the chapters.Endeavors of this size are not undertaken without help, and I would like to thank JonathanMink MD, one of the series editor, for includingthis topic. I would also like to thank LewisO’Sullivan, Martin Sugden, Michael Bevan, andLucinda Yeates at Wiley–Blackwell Publishingwho were instrumental in guiding me throughthis process.Finally, my father passed away during the editing of this text, and on retrieving his personalitems I discovered a number of medals of valor hereceived during World War II. He never spoke ofthese and my family was unaware of his possessions. This book is dedicated to him and to all thephysicians, nurses, and personnel in the neurological intensive care unit and elsewhere whoperform daily acts of valor with no expectationof recognition.Edward M. MannoClevelandix
Part IAcute Management of NeurologicalEmergencies
1Hypertensive EmergencyLaurie McWilliamsNeurocritical Care Unit, Cerebrovascular Center, Department of Neurology andNeurosurgery, Cleveland Clinic, Cleveland, OH, USAIntroductionHypertension and neurologic disease coexistfrequently, either as a cause or consequenceof the underlying neurologic disease. In addition,the management of elevated blood pressures inthis setting has significant impact on outcomes.Hypertension is defined as systolic blood pressure greater than 140 mmHg or diastolic bloodpressure greater than 90 mmHg. The NationalHealth and Nutrition Survey (NHANES) is conducted by the Centers for Disease Control andPrevention obtaining data from US householdindividuals regarding health and nutrition for thepurpose of improving the US health throughpolicy. The NHANES 2005 to 2006 data reportedthat 29% of the United States population 18 yearsand older are diagnosed with hypertension. Ofthe population with treated hypertension, greaterthan 64% has controlled hypertension. Men havea higher rate of hypertension until the age of 45when the incidence of hypertension equalizesbetween men and women.In 2006 the mortality from hypertension wasreported in 56,561 individuals. Both the prevalence from hypertension and mortality has increased from the late 1990s to the 2000s. Theestimated direct and indirect cost of hypertension for the year 2010 was 76.6 billion US dollars.The sequelae of hypertension include strokes,myocardial ischemia, aortic dissection, and renalinsufficiency. The remaining text of the chapterwill focus on the management of blood pressurein the specified acute neurologic diseases.Hypertensive crisis is defined as an abruptelevation of blood pressure, to a point that theblood vessels are unable to maintain constantblood flow in the setting of increasing perfusionpressures to specific organs, also known as disruption of autoregulation. The end result leads toend-organ damage from ischemia or hemorrhage. The end result leads to end-organ damagefrom ischemia or hemorrhage.Patients with blood pressure elevations greaterthan 180/110 mmHg are categorized into the following diagnoses:1. Severe hypertension: no to mild symptomsand no acute end-organ damage2. Hypertensive urgency: significant symptomsand mild acute end-organ damage. Mildend-organ damage is defined as dyspnea andheadaches.3. Hypertensive emergency: severe symptomswith life-threatening end-organ damage.Life-threatening end-organ damage is defined asacute ischemic stroke, intracerebral hemorrhage,subarachnoid hemorrhage, acute aortic dissection, myocardial infarction, acute heart failure, eclampsia, renal insufficiency, and acuteEmergency Management in Neurocritical Care, First Edition. Edited by Edward M. Manno. 2012 John Wiley & Sons, Ltd. Published 2012 by John Wiley & Sons, Ltd.3
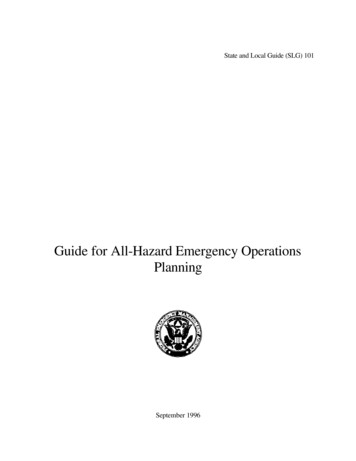
4 . Acute Management of Neurological Emergenciespulmonary edema, to name a few. The firstinstinct when dealt with this situation as a practitioner is to acutely correct the problem. However, there are some considerations prior toacutely correcting the blood pressure in a hypertensive crisis. The remainder of the chapter willdiscuss these considerations in relation to neurologic emergencies.Hypertensive urgencies include 25% of EDmedical visits, while hypertensive emergenciesare one-third of the cases. CNS complicationsare the most frequent of the hypertensive emergencies. The hypertensive emergent patient withneurologic sequelae needs urgent attention, withhourly blood pressure monitoring and neurologicexamination in an intensive care unit. Prior todiscussing blood pressure management, a discussion of cerebral autoregulation and the parental antihypertensive agents will be reviewed.Cerebral AutogregulationCerebral blood flow (CBF) is tightly controlledunder the normal conditions, with cerebral perfusion pressures (CPP) ranging from 50 to 150mgHg. Cerebral perfusion pressures can be calculated from mean arterial pressure (MAP) minusjugular vein pressure (JVP). Intracracranial pressure (ICP) is substituted for JVP under conditionswhere the ICP is greater than the JVP. Cerebralautogregulation involves arteriole caliberchanges in response to changes in the bloodpressure; however, there are upper and lowerlimits that lead to a disruption of this systemwith resultant ischemia or cerebral edema(Figure 1.1).The underlying mechanisms of autoregulationthat allow for vessel caliber changes are myogenic and metabolic. When the MAP decreases,the arterioles constrict to increase the CBF;however, if hypotension persists beyond thelower limit threshold, resultant cerebral ischemia exists. If the blood pressure continues toincrease above the higher limit threshold, theresult is hyperemia and cerebral edema. However, in brain dysfunction, the blood–brainbarrier and cerebral endothelium is disrupted,leading to leaky blood vessels with subsequentfibrinoid deposition into the cerebral vasculature. This results in vascular narrowing, withcompensatory vasodilation. In these circumstances the autoregulation curve follows a morelinear pattern with the CBF being dependent onperfusion pressures.Normal CBF is 50 mL/100 g brain tissue perminute. Reversible injury, occurs at 15–20 mL/100 g/min, and irreversible injury is less than15 mL/100 g/min. The occurrence of cell deathis based on the product of the degree and lengthof time of ischemia. The ischemic penumbra isvulnerable tissue with impaired autoregulationand low blood flow despite high oxygen extraction. Therefore the tissue is salvageable but has ahigh risk of becoming ischemic if the blood flowis not recovered in a short period of time.Figure 1.1. Autoregulation maintains cerebral blood flow relatively constant between 50 and 150 mmHgmean arterial pressure. The range is right shifted in chronically hypertensive patients. (Reproduced from Rulandand Aiyagari. Hypertension 2007; 49: 978, with permission from Wolters Kluwer Health.)
1 Hypertensive Emergency . 5SCIENTIFIC EVIDENCEAn EEG is a useful tool for monitoringseizures, but also for detecting cerebralblood flow. In the operation room, olderstudies have shown that EEG can detectreal-time ischemia. When cerebral bloodflow reaches 25–30 mL/100 g/min, an EEGdemonstrates a change in morphology,amplitude, and frequency. When the CBFdecreases to less than 15 mL/1006/min, theEEG becomes isoelectric. The neurons thatproduce the excitatory post-synaptic potential (EPSP) and inhibitory post-synapticpotential (IPSP) for the electrodes are thesame neurons (pyramidal neurons) that aresensitive to hypoxia.Antihypertensive AgentsHypertensive emergency can be fatal, and needsprompt treatment. The initial treatment is bloodpressure control, in a reliable and controlledfashion, therefore oftentimes, requiring parentalagents and arterial blood pressure monitoring.There are multiple classes of antihypertensivesone has to choose from; however, there are alsomany factors to consider prior to administration.The most important factor to consider in neurologic damage is increased intracranial pressure.A few class of antihypertensive agents workvia vasodilatory mechanisms, which can lead tofurther increases in intracranial pressure andpotentially further worsening of neurologic injury. Another factor is the onset and duration ofaction. Rapid fluctuations of hypotension andhypertension can lead to worsening cerebral injury. An agent that can be turned off and out ofthe system quickly is more desirable in case of anacute hypotensive episode.Preferred Agents for HypertensiveEmergencies with BrainDysfunctionBeta BlockersLabetalol is a selective alpha-1 and nonselectivebeta antagonist. The onset of action is 2–5 minutes with a peak effect seen in 5–15 minutes. Thehypertensive effect can last for 2–4 hours. Betaaction does cause a decrease in heart rate butmaintains the cardiac output. Similarly, cerebralperfusion is maintained with the use of betablockers.Start with a loading dose of 20 mg, increasingsubsequent doses from 20 to 80 mg every 10 minutes to the desired effect. In the author’s institution, if repeat labetalol boluses do not result inthe desired effect, an infusion is initiated startingat 1–2 mg/min.Esmolol is a short-acting beta antagonist, withno direct affect on the peripheral vasculature.Decreased blood pressure is secondary by decreasing cardiac output. The onset of action is60 seconds, with a duration of action of 10–20minutes. esmolol has a unique metabolic profile,being metabolized by red blood cell (RBC) esterases. In the setting of anemia, Esmolol canhave a prolonged effect. Due to its pure betaaction, caution should be used in patients withCOPD. Similarly it should be avoided in patientsin decompensated heart failure, due to compromising myocardial function.Start with a loading dose of 500–1000 mg/kg,with a continuous infusion at 50 mg/kg/min to amaximum of 300 mg/kg/min.TIPS & TRICKSBeta blocker toxicity can present withbradycardia, hypotension, bronchospasm,and hypoglycemia. An ECG can be helpfulwith detecting PR prolongation. QTprolongation can sometimes be detected.It should be treated with atropine forbradycardia, intravenous fluids andvasopressors for hypotension. Glucagon isa well-known antedote for the treatment ofbeta blocker toxicity.Calcium Channel BlockersThree types of calcium channel blocker exist:dihydropyridines, phenylalkylamines, and benzothiapines. The two types of calcium channelsthat exist in the vasculature are L-type andT-type.
6 . Acute Management of Neurological EmergenciesThe action of calcium channel blockers onL-type channels decrease calcium influx, resulting in elevated GMP levels. The elevated GMPlevels lead to vascular smooth muscle relaxation, vasodilation and decrease systolic bloodpressure.Nicardipine and clevidipine are the preferredparental calcium blocker agents for cerebrovascular hypertensive emergencies. Nicardipinecrosses the blood brain barrier, leading to vasodilation of the small-resistance arterioles, withlittle to no increases in intracranial pressure.The infusion rate starts at 5 mg/h, with incremental increases 2.5 mg/h every 5 minutes for amaximum infusion 30 mg/h. The onset of actionis 5–15 minutes, with duration of action 4 to6 hours.Of note, nicardipine has other properties thatmake it attractive in neurological diseases. It hasa high affinity to ischemic cerebral tissue due tothe acidic pH of ischemic tissue. Once in the cell,it is transformed to its active form, which maylead to a direct neuroprotective effect.The effect of nicardipine on intracranial pressure has been studied. Narotam et al. (2008)performed a prospective case-control study of30 patients with hypertensive emergencies inacute brain disease. Nicardipine was the first-lineantihypertensive agent. The results supportedthe ability t
pressure in the neurocritical or emergency care unit. The no-nonsense approach corresponds to the attitude needed in both acute emergencies and in the neurocritical care unit. Packed with handy tips to improve your care of patients, and written by internationally renowned experts, the bo