Transcription
AuthorTraves D. Crabtree M.D.Resident in General Surgery, Department of Surgery, University of Virginia, Charlottesville, VirginiaAssociate EditorsEugene F. Foley M.D.Associate Professor of Surgery; Director of Colon & Rectal SurgeryDepartment of Surgery, University of Virginia, Charlottesville, VirginiaRobert G. Sawyer M.D.Assistant Professor of SurgeryDepartment of Surgery, University of Virginia, Charlottesville, VirginiaContributorsLaurence H. Brinckerhoff M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaJames Forrest Calland M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaGerald A Cephas M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaJeffrey A. Claridge M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaTraves D. Crabtree M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaSteven M. Fiser M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaJames J. Gangemi M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaThomas G. Gleason M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaSantosh N. Krishnan Ph.D., M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaSteward M. Long III M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaPatrick J. O'Neill Ph.D., M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaAllan J. Parungao M.S., M.D.Resident in Plastic Surgery, Southern Illinois University School of Medicine, Springfield, IllinoisShawn J. Pelletier M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaDaniel P. Raymond M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, Virginia
P. James Renz III M.D.Resident in General Surgery, Southern Illinois University School of Medicine, Springfield, IllinoisCraig L. Slingluff Jr. M.D.Associate Professor of SurgeryDivision of Surgical Oncology, University of Virginia Health System, Charlottesville, VirginiaLisa M. Sullivan M.D.Resident in Anesthesiology, University of Virginia Health System, Charlottesville, VirginiaRobert D. Sullivan M.D.Resident in Anesthesiology, University of Virginia Health System, Charlottesville, VirginiaJames W. Thiele M.D.Resident in General Surgery, Southern Illinois University School of Medicine, Springfield, IllinoisLee W. Thompson M.D.Resident in General Surgery, University of Virginia Health System, Charlottesville, VirginiaSecondary EditorsElizabeth NieginskiEditorJulie P. MartinezEditorial DirectorBridget BlatteauDevelopment EditorDvora KonstantDevelopment EditorAimee SirmonM arketing M anagerDarrin KiesslingM anaging Editor
DedicationThis book is dedicated to my two little girls, Abby and Ellie, and to my wife, Faye, for her unconditional support, patience, and love, andunderstanding that “I'll be home soon” is very much a relative term during a surgical residency.Traves D. Crabtree
PrefaceWith continued advances in the field of surgery, a comprehensive textbook covering all aspects of surgery, though important as areference guide, can be overwhelming to the medical student or junior resident seeking a general review of the entire field. BRS GeneralSurgery represents a concerted effort on the part of the faculty and resident staff at the University of Virginia and Southern IllinoisUniversity to provide a concise review of surgery for medical students and junior residents, specifically for the surgical section of theUnited States M edical Licensing Examination (USM LE Step 2).This text covers the background principles of surgery, in addition to major topics in general surgery, with essential information onepidemiology, pathogenesis, diagnosis, and treatment. It is designed to provide an understanding of the details of each disease process,but intentionally focuses on the practical clinical approach to diagnosis and management of surgical problems. To this end, we have heavilyrelied on outlines, tables, figures, and clinical questions with explanations, instead of depending solely on standard text.This book incorporates input from a large number of faculty and residents from two separate institutions. Recognizing that no one style ofpresentation is appropriate for all students or all topics, we hope to have combined the best aspects of the teaching skills from thisdiverse group of “experts.” We are hopeful that this text will provide an interesting, effective, and enjoyable clinical review for studentsof surgery at this critical and exciting point in their careers.Eugene F. Foley M .D.
AcknowledgmentI would like to especially thank Dr. Kristen M . Jacobs and Dr. James Thiele for their valuable input and assistance during the writing of thisbook.
1AnesthesiologyRobert D. SullivanLisa M. SullivanI. Initial Assessment and MonitoringA. Preoperative assessment of the surgical patient1. The American Society of Anesthesiologists (ASA) Classificationis part of the physical evaluation of the patient (Table 1-1).2. The classification systemis graded as classes 1–6 in order of increasing risk of mortality.B. Blood pressure1. Noninvasive blood pressure monitoringa. An appropriate size cuffis most often placed on the arm, avoiding limbs with arterial-venous shunts or intravenous (IV) sites.b. A cuff that is too narrowrelative to patient size may give a falsely elevated blood pressure.2. Intra-arterial blood pressure monitoringa. Indications for intra-arterial monitoring includeelective hypotension.anticipation of wide blood pressure variation.the need for frequent blood sampling.b. The most common sites of measurementare the radial and femoral arteries.C. Electrocardiogram (ECG)1. The ECG is used for detection ofcardiac dysrhythmias.myocardial ischemia.electrolyte abnormalities, which are not uncommon under anesthesia.2. Leads V2 and V5together can detect 95% of intraoperative ischemia, allowing for early intervention.Table 1-1. American Society of Anesthesiologists (ASA) Physical Status ClassificationClass 1: Healthy
Class 2: M ild systemic disease without functional limitationClass 3: M oderate to severe systemic disease with functional limitationClass 4: Severe systemic disease that is constantly life-threatening and functionally incapacitatingClass 5: Not expected to survive 24 hours with or without surgeryClass 6: Organ donorE: Added to classification if procedure is an emergencyD. Pulse oximetry1. An oximeteris placed on any perfused tissue that can be transilluminated.2. This providesan estimate of the level of oxygen binding by hemoglobin in the blood, providing an early warning of hypoxia.3. Arterial oxygen saturation (SaO2)of 70%, 80%, and 90% corresponds to arterial oxygen tensions (PaO 2) of 40, 50, and 60, respectively.4. In the presence of severe anemiaoximeter readings may be normal even when tissue hypoxia is present.E. Temperature1. Monitoring sites includeesophagus.nasal pharynx.axilla.bladder.2. Maintenance of normothermiacan improve tissue perfusion and limit coagulopathies.3. Elective hypothermiais used to decrease tissue oxygen demand, particularly for some cardiac and neurosurgical procedures.F. Urine output (UOP)1. Monitoring UOPvia a Foley catheter provides an estimate of end-organ perfusion and fluid status.2. This is generally usedfor all surgeries over 2 hours.
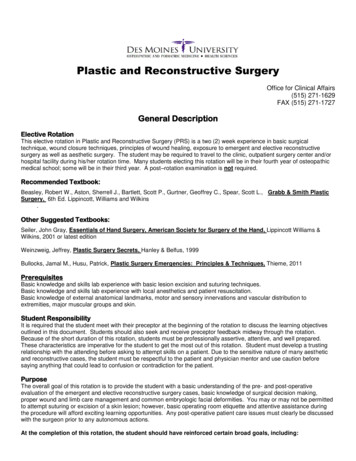
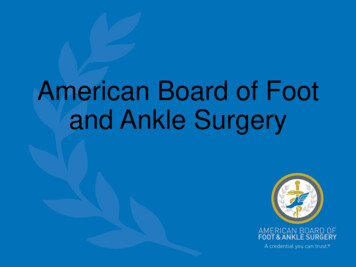
to decompress the bladder to avoid injury during laparoscopic procedures and cesarean sections.G. Swan-Ganz catheter1. The tip of this catheterlies in the pulmonary arterial system.2. The pressure changesobserved during initial placement of a Swan-Ganz catheter are demonstrated in Figure 1.1.3. This catheter is used to monitorleft ventricular filling pressures.cardiac output.systemic vascular resistance.Figure 1.1. Swan-Ganz catheter placement. A pressure tracing during passage of a Swan-Ganz catheter from the right atrium (RA) tothe point where the catheter tip is wedged within a branch of the pulmonary artery (PCWP). Passage into the right ventricle (RV) ismarked by a sudden increase in systolic pressure, the pulmonary artery (PA) by an increase in diastolic pressure, and PCWP by adecrease in pressure. (Reprinted with permission from M organ E, M ikhail N: Clinical Anesthesiology, 2nd ed. Stamford, CT, Appleton& Lange, 1996, p 89.)H. Capnography1. This methodprovides measurement of end-tidal carbon dioxide (CO2) tension.confirms adequacy of ventilation and thus endotracheal tube (ETT) placement.2. This measurement is an estimate of PaCO 23. The same device also measures inspiratory and expiratory anesthetic gas concentrations, confirming anesthetic gas delivery.4. Unexpected severe hypercapnia can also be a sensitive indicator of malignant hyperthermia.I. Transesophageal echocardiogram (TEE)
may be used to monitor cardiac function, particularly during cardiac or aortic procedures.II. Induction of AnesthesiaA. Methods1. IV or mask inductionof general anesthesia may be used.2. Children frequently undergo a mask induction with volatile anesthetic gas before placement of an IV, whereas adults most oftenundergo an IV induction.3. A variable combination of agents is based on patient characteristics and the surgical procedure.These include an amnestic, analgesic, hypnotic, muscle relaxant, and volatile agent.4. A “rapid sequence” inductionis performed by sequential IV administration of fast-acting agents with rapid endotracheal intubation.a. Pre-oxygenation with 100% oxygenallows de-nitrogenation of the patient's functional residual volume.provides extra time for airway management before arterial oxygen desaturation occurs.b. Indications for rapid sequence induction includerecent oral intake.symptomatic gastroesophageal reflux disease (GERD).delayed gastric emptying (e.g., gastroparesis) or previous gastrectomy.pregnancy.bowel obstruction.B. Analgesic agents1. Analgesic agents are generally administeredin boluses at induction and before surgical incision, then in maintenance doses as needed.2. Additional doses may be administeredbased upon signs of the sympathetic response to pain, such as increasing heart rate and blood pressure.3. Fentanylis a synthetic narcotic.has an onset of action in 2 minutes and peak effect in 5 minutes.a. This drug is metabolizedby the liver.b. Airway reflexes are blunted with minimal cardiac depression.Like other narcotics, this may induce respiratory arrest.4. Morphine sulfateis a narcotic.has a 5-minute onset of action and 20 minutes to peak effect.a. The active metabolites are cleared by the kidney.Therefore morphine should be used cautiously in patients with impaired renal function.
b. This may cause histamine releaseand associated mild hypotension.5. Alfentanil, sufentanil, and remifentanilare synthetic narcotics.have very fast onset and progressively shorter durations of action.6. Ketamineis a phencyclidine (PCP) analog.a. This drug provides intenseanalgesia.amnesia.dissociative anesthesia.b. It alsogenerally increases heart rate and blood pressure.maintains spontaneous ventilation.is an excellent bronchodilator.c. Illusions and dysphoria are commonbut can be limited by premedicating with a benzodiazepine.d. Ketamineis not a respiratory depressant.may be given as the sole anesthetic agent.is one of several agents used for induction of anesthesia (Table 1-2).C. Sedative–hypnotic agents1. Sodium thiopental (see Table 1-2)is a barbiturate.induces unconsciousness within 30 seconds without providing analgesia.reduces cerebral oxygen demand and is an excellent anticonvulsant.a. After a single dose, drug redistribution into muscle may result in rapid awakening.Therefore frequent repeated dosing is necessary.b. Side effects includehypotension that may be profound in the setting of hypovolemia.heart failure.beta-blockade.c. Thiopental may also causerespiratory arrest.Table 1-2. Anesthetic Induction AgentsA g entBlo o d Pr essur eM etabo lismA nalg esiaOnsetA ctio ns and Effects
KetamineStableLiverPotentFastIllusions and dysphoriaSodium lDecreasedLiver and plasma esterasesM ildFastAntiseizure, infusionsEtomidateStableLiver and plasma esterasesNoneFastAdrenocortico depressant2. Propofol (see Table 1-2)is also a fast-acting agent.does not produce a “hangover” effect, thus it is ideal for outpatient surgeries.possesses antipyretic and antiemetic properties.a. Rapid metabolismoccurs via the liver and plasma esterases.b. Side effects includehypotension.blunting of airway reflexes facilitating intubation.respiratory arrest.c. This drug may be usedto maintain anesthesia.in the intensive care unit to provide sedation.d. Propofolis suspended in a 10% lipid solution providing 1.1 kCal/mL.3. Etomidate (see Table 1-2)is a fast-acting hypnotic agent.is commonly used for induction when hypotension must be minimized.a. Rapid metabolismis via the liver and plasma esterases.b. Continuous infusionsare avoided because of the risk of adrenocortical suppression.c. Other side effectsinclude myoclonus.4. Benzodiazepinesa. These drugs provideanxiolysis.hypnosis.amnesia.anticonvulsant effects.some skeletal muscle relaxation.b. They do not provideanalgesic properties.
c. The most commonly used benzodiazepineis the short-acting agent, midazolam.d. These agentsare hepatically metabolized.may have prolonged activity in geriatric patients and patients with liver failure.e. Morphine agents may causerespiratory arrest, especially when combined with a narcotic.f. Flumazenil is a benzodiazepine antagonist used to treat overdoses.However, this agent may be associated with seizure development.D. Muscle relaxants (Table 1-3)Table 1-3. Neuromuscular Blocking AgentsA g entDepo lar izing Blo ck adeFasiculatio nsM etabo lismIncr eased Ser umPo tassiumA ctiv itySuccinylcholine Pseudocholinesterase Fastest onset and shortestdurationRocuronium–Liver–Fastest onset of nonde-polarizersPancuronium–Renal–Longest ion not prolonged in renal orliver diseaseM ivacurium–Pseudocholinesterase–Brief duration1. Muscle relaxation is often usedto facilitate endotracheal intubation.during abdominal surgery.when movement could be devastating (neurosurgery).2. These drugs do not posses properties of analgesia, hypnosis, or amnesia.Patients are paralyzed, but will still feel and remember the surgery.3. Relaxants are divided into depolarizing and nondepolarizing agents.Depolarizing agents cause an initial transient muscle fiber activation before relaxation occurs.4. Succinylcholineprovides rapid depolarizing neuromuscular blockade.a. This agentmimics acetylcholine.
has a rapid onset of 30 seconds.has a short duration of action (5–10 minutes).b. It is rapidly metabolizedby plasma pseudocholinesterase.c. Patients with abnormal pseudocholinesterasemay have prolonged paralysis after administration of succinylcholine.1. About 1 in 3000 patients are homozygous for this trait.2. The onset of this effect is heralded by muscle fasciculations.d. Cellular potassium release from initial muscle fiber activation causes an increase in serum potassium that can be dangerous in somepatients.Patients with the potential for a greatly exaggerated increase in serum potassium are at risk for hyperkalemic cardiac arrest.e. Conditions where this agent is contraindicated includedenervation injuries (e.g., stroke).myopathy.major burn injuries.severe trauma.potentially undiagnosed myopathy (i.e., children).bedridden states.f. Malignant hyperthermiais a rare complication associated with succinylcholine administration.is an autosomal dominant hypermetabolic disorder of skeletal muscle.1. The combinationof volatile anesthetics and succinylcholine most frequently triggers this disorder.2. Manifestations may includeacidosis.trismus/masseter muscle spasm.hypercapnia.tachycardia.rapid temperature kalemia.myoglobinuria.3. Treatment involvesdiscontinuing the volatile agent.cooling the patient.IV dantrolene.5. The nondepolarizing neuromuscular blocking agents m.
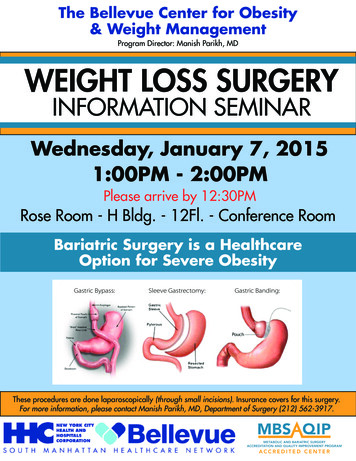
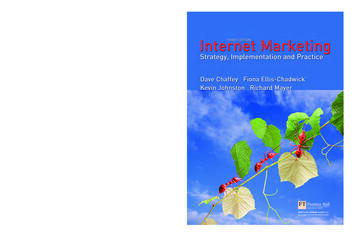
mivacurium.a. These agentscompetitively inhibit acetylcholine at the neuromuscular junction.b. These agents do not causefasciculations.an increase in serum potassium.c. Rocuroniumhas the fastest onset (45–60 seconds).is often substituted for rapid sequence induction when succinylcholine is contraindicated.d. Pancuroniumis inexpensive and used when prolonged paralysis is needed.1. This agent blocks autonomic ganglia, resulting in a mild tachycardia.2. Clearance is dramatically prolonged in renal failure.e. Atracuriumundergoes esterase elimination.does not require the kidney or liver for metabolism.f. Mivacurium metabolism is dependent on pseudocholinesterase.g. All agents are potentiated byhypokalemia.hypocalcemia.hypermagnesemia.h. The degree of neuromuscular blockadecan be monitored by peripheral nerve stimulation.i. To reverse neuromuscular blockadeacetylcholinesterase inhibitors (e.g., neostigmine) given with an anticholinergic (e.g., glycopyrrolate) to counteractbradycardia are often administered at the end of a surgery.III. AirwayA. Mask ventilationis used at the time of induction.can be the sole means of airway management in a patient with minimal risk of aspiration.1. The head and jawmust be positioned appropriately to open the airway and to avoid collapse of soft tissues.2. Ventilation can also be facilitatedby either an oral or a nasal airway device (Figure 1.2).a. Oral airway devicesprevent the tongue from obstructing the oropharynx.b. Insertion of nasal airway devices
may be tolerated by an awake patient.Figure 1.2. Interventions providing airway patency without endotracheal intubation. All of these measures alleviate obstructionoften caused by the tongue allowing for ventilation, but these do not protect against aspiration. (A) M ask ventilation with jawthrust. (B) Oropharyngeal airway device. (C) Nasopharyngeal airway device. (Adapted with permission from Dorsch JA, Dorsch SE:Understanding Anesthesia Equipment: Construction, Care, and Complications. Baltimore, Williams & Wilkins, 1994, p 371.)B. A laryngeal mask airway (LMA) deviceis designed to lodge in the hypopharynx superior to the larynx.prevents soft tissue obstruction of the airway.a. The LMA can be usedto ventilate a patient with up to 20 cm H20 pressure (the competency of the upper esophageal sphincter).b. This device is contraindicatedin patients at risk for aspiration.in cases where paralysis, controlled ventilation, or both, are necessary.C. Endotracheal intubationinvolves placement of a tube through the vocal cords into the trachea under direct visualization.1. Placement of an ETT allows forventilatory support.
oxygenation.relative protection of the airway from aspiration.2. Tube position may be confirmed byobserving bilateral chest rising with ventilation.looking for condensation of breaths within the ETT.3. Continuous measurement of end-tidal CO2may also confirm appropriate placement of the tube within the trachea.4. If a patient appears difficult to intubatethe safest option is to allow for spontaneous ventilation and intubate with topical airway anesthetics and minimal sedation.5. Fiberoptic laryngoscopycan aid in the intubation of the difficult airway, especially in patients with head and neck injuries.IV. Inhalational AnestheticsA. After inductionanesthesia is maintained with a volatile anesthetic.B. The volatile anesthetics providehypnosis.amnesia.some degree of analgesia and muscle relaxation.C. The agents differ inblood solubility.potency.side effect profiles.1. The minimum alveolar concentration (MAC)is the smallest concentration of anesthetic at which 50% of patients will not move in response to surgical incision.2. The MAC of the agentsare generally additive, while the side effects are not.Combining different agents to optimize the M AC while minimizing potential side effects is referred to as balanced anesthesia.3. The solubility of the agentwithin the blood correlates with speed of induction.Thus insoluble agents provide the quickest onset.D. The volatile agents commonly used today includehalothane.isoflurane.
sevoflurane.desflurane (Table 1-4).Table 1-4. Inhalational Anesthetic AgentsA g ent*Blo o d Pr essur eM uscleRelaxatio nBr o ncho dilatatio nExpands A irCav itiesM isc.HalothaneDecreased cardiacoutput -Rarely causeshepatitisIsofluraneDecreased vascularresistance -Used in cardiac andCNSSevofluraneDecreased vascularresistance -Used in maskinductionsDesfluraneDecreased vascularresistance -Irritating to airwayNitrous oxide(N2O)Stable-- M ask analgesiaCNS central nervous system.*The agents are listed in order of decreasing blood solubility (faster induction and emergence) and also in order ofdecreasing potency (higher percentage of inhaled gas required for effect).E. Side effects1. Cardiovasculara. All of these agents cause hypotensioneither through depression of myocardial contractility (e.g., halothane) or via vasodilation.b. These agents, particularly halothanetend to be arrhythmogenic, an effect potentiated in many cases by epinephrine.c. Isoflurane is often preferredfor patients with cardiac disease because it causes the least cardiac depression and the most coronary artery dilation.2. Respiratorya. Volatile agents causerapid shallow breathing, resulting in a net decrease in minute ventilation.bronchodilation.b. All agents severely blunt hypoxic driveand to a lesser degree, blunt hypercapnic drive, in subanesthetic concentrations.3. Central nervous system
a. These agentsimpair cerebral autoregulation, or the ability of the brain vasculature to control blood flow over a wide range of bloodpressures.b. Isofluraneused in conjunction with hyperventilation minimizes the impaired autoregulation.is used in patients with increased intracranial pressure.4. Halothanecan rarely cause a chemical hepatitis.5. All volatile agents causesignificant muscle relaxation independent of paralytic agents.F. Nitrous oxide (N2O)requires high inhalational concentrations (not potent).is insoluble in blood.1. Cardiac effectsN20 causes minimal cardiac depression.It generally does not alter blood pressure.2. Respiratory effectsThis agent shares many of the respiratory effects of the volatile agents.However, it is not bronchodilatory and causes an increase in pulmonary vascular resistance.3. This agent does notprovide muscle relaxation.4. Administration of N20 may expand air cavitiesby diffusing in faster than nitrogen diffuses out.5. This agent should be avoided in patients witha pneumothorax.intracranial air.intestinal obstruction.middle ear occlusion.V. Regional AnesthesiaA. Overview1. Many surgeries can be successfully performedwith neuraxial or peripheral application of local anesthetics.2. Regional anesthesia may also be usedfor postoperative pain relief.3. Upper extremity regional blocks includeintrascalene.supraclavicular.
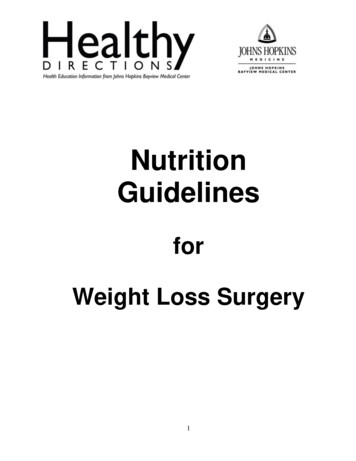
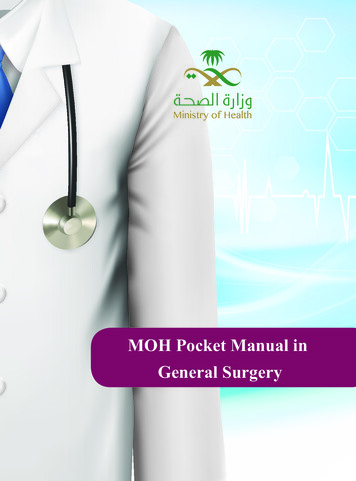
axillary nerve blocks.4. A femoral nerve block can be used for lower extremity anesthesia.5. A Bier block involves IV injection of local anesthetic for upper and occasionally lower extremity anesthesia.Before IV injection of anesthetic into the designated extremity, the venous system is emptied by compression with elastic wrapsand a tourniquet is placed to block arterial inflow.6. Neuraxial blockade involvesinjection of anesthetic into either the epidural or subarachnoid spaces.7. Contraindications shared by the Bier and neuraxial blocks includelocal or systemic infection.coagulopathy.hypotension.8. Complications includeheadache.urinary retention.rarely, epidural or intraspinal hematomas or infection.a. Postpuncture dural headachesare positional, being much worse when the patient is upright.b. Treatment of these headaches ural blood patching.c. For an epidural blood patch, peripherally drawn blood is injected into the epidural space at the dural puncture site to seal theinjured dura.B. Spinal anesthesia (Figure 1.3)
Figure 1-3. Lumbar spinal versus epidural anesthesia. (Reprinted with permission from M organ E, M ikhail N: Clinical Anesthesiology,2nd ed. Stamford, CT, Appleton & Lange, 1996, p 222.)1. A small gauge needle (e.g., 22 gauge)designed to minimize dural trauma is usually inserted midline in the L3–L4 interspace.2. Free flow of cerebrospinal fluid (CSF)confirms subarachnoid placement where local anesthetic is injected.3. Anesthesiaonset occurs within minutes.can last up to 2 hours depending on the agent and dosage.4. The level of sympathetic blockadeis typically higher than the level of sensory block.a. This is, in turn, above the level of motor block.b. These differences are caused by variations in nerve size and myelination.5. Sympathetic blockade results in hypotension that may be profound.6. Excessively high spinal anesthesia may cause respiratory depression.7. Motor function typically recovers before sensation.8. Small doses of narcoticscan also be injected intrathecally to provide analgesia or to augment local anesthetic action.9. A “saddle block”provides anesthesia to the perineum by using hyperbaric solutions (solutions more dense than CSF) to block the sacral dermatomes.C. Epidural anesthesia1. A cathetermay be placed in the epidural space, allowing for continuous infusion of anesthetic agent to relieve perioperative pain or laborpain.2. Dilute concentrations of anestheticallow for sparing of motor function.3. The final level of sensory blockadeis related to the volume injected, which is in contrast to spinal anesthesia, where it is related to dosage.4. The onset of blockadeoccurs more slowly than with spinal anesthesia.5. A caudal blockinvolves placement of anesthetic into the epidural space through the sacral hiatus.D. Local anestheticsmay be infiltrated in a wound to provide local pain relief.1. The most common agents are
lidocaine.ropivacaine.bupivacaine.a. These agents may be associated withseizures and severe refractory arrhythmias if injected intravascularly, particularly bupivacaine.b. Early manifestations may includeperioral numbness.visual and hearing disturbances.sedation.2. Epinephrine-induced local vasoconstriction may prolong the anesthetic effects of these agents.Epinephrine with local anesthetics should be used cautiously in patients with cardiac disease, uncontrolled hypertension, or wheninfiltrating tissues with minimal collateral blood flow (e.g., digits, ears, nose, penis).VI. Pain ManagementA. Patient controlled analgesia (PCA)is often used for postoperative pain relief.a. Narcoticsare self-administered by the patient through a device that allows a selected dose to be delivered at specific time intervals to apreset maximum.b. The pump can also be setto deliver a basal rate of medication per hour.c. PCA is designed toprovide better pain control.avoid over-medication of the patient.B. Pain management clinicsspecialize in the treatment of chronic pain.a. Components of treatment of chronic painroutinely include psychological evaluation and therapy.b. Narcotics are avoided when possible in favor of other agents includingnonsteroidal anti-inflammatory agents.antiseizure medications (e.g., gabapentin).antidepressant medications (e.g., amitriptyline).c. Regional anesthetic techniquesare also frequently used.Review TestDirections: Each of the numbered items or incomplete statements in this section is followed by answers
or by completions of the statement. Select the ONE lettered answer or completion that is BEST in eachcase.1. At emergence from an uncomplicated general anesthetic for a laparoscopic appendectomy, an otherwisehealthy 19-year-old male smoker develops a severe cough. Intravenous lidocaine is administered and theendotracheal tube is pulled before the patient is responsive to verbal commands. The patient becomescyanotic and the SaO2 is 75%. The anesthesiologist is unable to administer positive pressure maskventilation. What is the most appropriate initial step in the management of this patient?(A) Intravenous naloxone(B) Deepen anesthetic depth(C) Re-intubate the patient(D) Intravenous succinylcholine(E) Intravenous fentanyl1–D. The anesthesiologist is probably unable to ventilate the patient because the patient is inlaryngospasm. Intravenous (IV) lidocaine is effective at preventing and treating laryngospasm butsmokers have particularly reactive airways that predispose to coughing and laryngospasm at emergence.IV or intramuscular succinylcholine can rapidly relieve the spasm. Partial laryngospasm (stridor) oftenresponds to gentle positive pressure ventilation, deepening the anesthetic volatile agent, or both. Aninitial attempt at intubation would likely be unsuccessful and can worsen the spasm. Neither naloxone norfentanyl is likely to have much effect. Healthy adults can generate enough negative intrathoracic pressureagainst a closed glottis that they can suffer postobstructive pulmonary edema.2. A 27-year-old woman with gastroesophageal reflux disease (GERD) undergoes a rapid sequence anesthetic induction for an anteriorcruciate ligament repair. She is pre-oxygenated with 100% oxygen (4 deep breaths) and induced with propofol, lidocaine, and fentanyl.Succinylcholine is administered and cricoid pressure applied. The endotracheal tube (ETT) is placed with direct laryngoscopy to 20 cmat the teeth and the SaO2 is 100%. What is the most reliable indication of ETT placement in the trachea?(A) Persistent ETCO 2 measurement with ventilation(B) Bilateral breath sounds with ventilation(C) Breath condensation in the ETT(D) Absence of sound over the epiga
BRS General Surgery represents a concerted effort on the part of the faculty and resident staff at the University of Virginia and Southern Illinois University to provide a concise review of surgery for medical students and junior residents, specifically for the surgical section of the Unit