Transcription
INSIGHT on the IssuesAARP Public Policy InstituteRemoving Barriers to Advanced Practice RegisteredNurse Care: Hospital PrivilegesAndrea BrassardAARP Public Policy InstituteMary SmolenskiConsultantThe Institute of Medicine recommends that advanced practice registered nurses(APRNs) practice to the full extent of their education and training, which includesbeing able to admit their patients to the hospital and other facilities. This reportdiscusses barriers to hospital privileges and outlines the benefits to consumersand the health care system when APRNs have hospital privileges.IntroductionContinuity of care is improved whennurse practitioners (NPs) and otheradvanced practice registered nurses(APRNs) who care for patients inprimary care settings can follow theirpatients and their families when theyare admitted to the hospital. AlthoughAPRNs have made headway inpracticing to the full extent of theireducation and training, barriers stillhamper continuous, seamless patientcare.Federal and state laws and regulations,as well as individual hospital bylaws andpolicies, can block hospitalized patients’access to their provider of choice, ifthat provider is an APRN. Removingbarriers to care reduces costs, increasesconsumer choice, and improves healthcare quality.1This report discusses barriers tohospital privileges and expands onrecommendations of the Institute ofMedicine (IOM) report The Future ofNursing: Leading Change, AdvancingHealth2 that APRNs be eligible forhospital clinical privileges, admittingprivileges, and hospital medical staffmembership and also be permittedto perform hospital admissionassessments—documenting medicalhistories and performing physicalexaminations.APRNs Provide High Quality Carein Hospitals and Other Health CareSettingsThe ability of a primary care providerto care for a patient who is admitted toan acute care facility is more criticalthan ever. As noted in a previous AARPPublic Policy Institute paper, Creatinga 21st Century Nursing Workforce toCare for Older Americans: ModernizingMedicare Support for NursingEducation, cost containment effortshave shortened the average hospital stayfrom 8.7 days in 1990 to 5.5 days by2006. Hospital admissions frequentlyrequire a coordinated team to providecomprehensive and efficient care. Boththe numbers and life expectancy ofpersons ages 65 and over are increasing.Chronic illness afflicts nearly half ofAmericans, and just under one quarterhave five or more chronic conditions.3
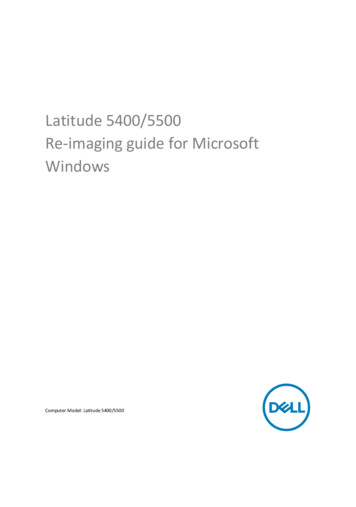
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital PrivilegesWho Are Advanced Practice Registered Nurses?Advanced practice registered nurses (APRNS): Areregistered nurses (RNs) with master’s, post-master’s, or doctoral degrees Pass national certification exams Teach and counsel patients to understand their health problems and what they cando to get better Coordinate care and advocate for patients in the complex health care system Refer patients to physicians and other health care providersTypes of Advanced Practice Registered NursesWho AreThey?NPsHow Manyin U.S.?158,348CNSs59,242CRNAs34,821CNMs18,492What do they do?Take health histories and provide complete physical exams;diagnose and treat acute and chronic illnesses; prescribe and managemedications; order and interpret lab tests and X-rays; provide healthteaching and supportive counseling.Provide advanced nursing care in hospitals and other clinical sites; provideacute and chronic care management; develop quality improvementprograms; serve as mentors, educators, researchers, and consultants.Administer anesthesia and related care before and after surgical,therapeutic, diagnostic, and obstetrical procedures, as well as painmanagement. Settings include operating rooms, outpatient surgicalcenters, and dental offices.Provide primary care to women, including gynecological exams,contraceptives, prenatal care, management of low-risk labor anddelivery, and neonatal care. Practice settings include hospitals, birthingcenters, and community clinics.Sources: AARP Public Policy Institute, Center to Champion Nursing in America. Preparation and Roles of Nursing Care Providers inAmerica. Washington, DC, 2009, PRN-Types 1.pdf; U.S. Department of Health andHuman Services, Health Resources and Service Administration. The Registered Nurse Population: Initial Findings from the 2008National Sample Survey of Registered Nurses . Washington, DC, 2010. (APRNs are identified by their responses to the NationalSample Survey and may not reflect the true population of clinical nurse specialists.)Patients with extremely complexconditions and with multiple diseaseprocesses are cared for in thecommunity on a daily basis by APRNs,particularly NPs. Hospitals employ nursepractitioners in their outpatient clinics,emergency departments, and inpatientunits.and approximately 20 percent of theseNPs see patients ages 65 and over morethan half of their clinical time. For justunder 11 percent of all nurse practitioners,patients ages 85 and over are morethan half of their patient population.4More than 88 percent of family nursepractitioners and adult nurse practitionersaccept Medicare patients, and more than80 percent of both groups accept Medicaidpatients.5Survey data from the American Academyof Nurse Practitioners demonstrate thatNPs care for large numbers of olderpeople and people with chronic, multipledisease processes. Three-quarters ofall nurse practitioners have a patientpopulation that includes people over 65,Another category of APRNs, certifiedregistered nurse anesthetists (CRNAs),ensure access to anesthesia and painmanagement services, particularly in2
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital Privilegesrural and underserved communities. A2007 Government Accountability Officestudy revealed that CRNAs predominatewhere more Medicare patients reside.6An aging population with increasingchronic conditions requires health careservices that are focused on primarycare, disease management, carecoordination, transitional care, andprevention of disease deterioration.APRNs are educated and trained toprovide high-quality health care servicesin hospitals and other settings.providers, allowing a more expedient,nonstressful admission for both patientand parent. Because of their nursingeducation and clinical training, APRNsknow the concerns of their patients andcan help make the hospital experience amore pleasant, less stressful time, therebyexpediting recovery time and improvingquality of life for patients.Based on data from the most recent NPsurvey of the American Academy ofNurse Practitioners (AANP), only about43 percent of the NPs in the United Stateshave hospital privileges, and just overhalf of these have admitting privileges,meaning that they can admit patientsfrom an office or outpatient setting to ahospital. This is a slight increase from the2005 AANP survey data, when 39 percentof NPs had privileges. The reason themajority of NPs do not have admittingprivileges is unclear.13States vary in how they license eachcategory of APRN. Ongoing efforts bystate licensure, accreditation, certification,and education organizations7 to standardizenational credential requirements willfacilitate the mobility and interstatepractice of this major primary careprovider group, thus decreasing one barrierto care. The IOM report The Future ofNursing: Leading Change, AdvancingHealth9 recognizes the positive impactAPRNs can have on the health care systemif barriers to care are removed.The three other categories of advancedpractice registered nurses, certifiedregistered nurses anesthetists (CRNAs),certified nurse-midwives (CNMs), andclinical nurse specialists (CNSs), typicallypractice in hospitals and other acute caresettings. The American Association ofNurse Anesthetists membership data for2010 reveal that approximately 37 percentof CRNAs are employed by hospitals andanother 34 percent are employed by ananesthesia group, with the vast majorityof CRNAs indicating that their primaryplace of employment is a hospital oraffiliated clinic.14APRNs, specifically NPs, hold prescriptiveprivileges in all 50 states, with the abilityto prescribe controlled substances in 48of them. Prescriptive authority is onearea of state nurse practice acts that hasbecome more uniform. A total of 96.5%of NPs prescribe medications, averaging20 prescriptions per day,8 making it a partof routine care. Prescribing a medicationregime or changing the existingmedications of a patient who is admitted tothe hospital is part of APRN education andtraining.According to the American College ofMidwifery Certification Board, as ofJanuary 2011 there were nearly 12,000certified nurse-midwives in the UnitedStates. The most recent American Collegeof Nurse-Midwives membership surveydata show that approximately 52 percentof respondents (22 percent of total)are employed by hospitals and privatephysicians. The majority of CNMs(69 percent) attend live births in hospitalsor hospital-based birthing centers.15A multitude of studies show that thequality, efficiency, patient satisfaction,and cost-effectiveness of APRN care isas good as, and in some cases better than,the care provided by physicians.10,11,12Care coordination and transitions ofcare are extremely important to positiveoutcomes of hospital care, not onlyfor older patients but for any patient.Pediatric patients respond best to familiar3
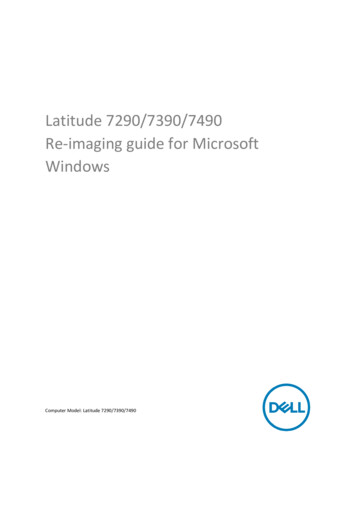
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital PrivilegesPrivileging CNMs as full active medicalstaff would promote continuity of carefor their patients, and birth certificate datawould more accurately reflect providertype and outcomes.16Metropolitan ChicagoHealthcare CouncilThe Metropolitan Chicago HealthcareCouncil (MCHC) is a membershipand service organization dedicatedto helping members care for theircommunities through access to healthcare and improved delivery of services.The Advanced Practitioner RegionalCollaborative surveyed MCHCmember organizations to determinehospital demographics, credentialingand privileging processes, scopeof practice, and APRN activities.Seventeen member organizationsrepresenting almost 1,200 APRNswere surveyed. Key findings:Traditionally, clinical nurse specialistsother than those who function in mentalhealth have not sought credentialing andprivileging, and then only if they haveprescriptive authority—the legal rightto prescribe medications. The practiceof CNSs is primarily an extension andadvancement of nursing practice ratherthan of the physician model of care thatwould require hospital privileges.17 Thistrend may change as more CNSs willhave the option of prescriptive authoritywith the full implementation of theAPRN Consensus Model. The APRNConsensus Model establishes nationalstandards for education and trainingfor all categories of APRNs and wouldextend to consumers in all states accessto comprehensive care by APRNs.18 APRNsby category included60 percent NPs, 18 percentCRNAs, 16 percent CNSs, and6 percent CNMs. Sixty-threepercent of the APRNswere employed by the hospital;16 percent by hospital-ownedphysician practices; 16 percent byindependent physicians; 5 percentin other venues such as nursemanaged clinics.Numbers of practitioners holding hospitalclinical and admitting privileges varyacross the category and type of APRNs,with each group having the same hurdleof meeting the requirements of thehospital credentialing committee. In theNurse Practitioner’s Business Practiceand Legal Guide, Buppert19 states thatan NP must consider many issues whenapplying for hospital privileges, withor without admitting privileges. Is itnecessary for the type of practice thenurse practitioner has? Does the nursepractitioner feel comfortable in the hospitalcare setting? The newest subspecialty ofnurse practitioners, acute care NPs, receivespecific education and clinical training topractice in hospital settings. Onlya few organizations bill forAPRN services. Reasonsorganizations hiredAPRNs included the following:–Improve patient safety andqualityIncrease patient throughputComply with AccreditationCouncil for Graduate MedicalEducation standard forresident work hoursAcute care NPs are only 5.6 percent of theNP population,20 but NPs are part of therapid expansion of hospitalist services.21For NPs who practice in primary caresettings, hospital privileges may benecessary to be considered primary careproviders (PCPs). Private insuranceIncrease physician productivityImprove continuity of careSource: Trish Anen. “Advancing APNs: A RegionalCollaborative.” Metropolitan Chicago Healthcare Council,December 13, 2010.4
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital Privilegescompanies typically require hospitalprivileges before they will allow a PCP ontheir provider panel and to bill for officebased services.22and other professional qualifications.Privileging refers to authorizing thecredentialed individual to perform ororder specific diagnostic or therapeuticservices within the hospital. Hospitalprivileges, which used to be a simplematter, can now include a list of hundredsof diagnostic and treatment procedures.23Even though a practitioner may have thecredentials to perform certain diagnosticand treatment procedures, the practitionermust still be privileged, or grantedpermission, by the hospital or relatedentity to perform those procedures.Complexities of care, coordination ofcare, and transitions into and out of thecommunity during illness necessitate atransparent and seamless process thatallows providers to gain access to thepatients they have cared for and knowbest. Coordination of care and teamworkamong all health care providers is notonly advantageous but necessary forefficient and cost-effective care. Efforts tobreak down barriers between professionsare showing positive results, and APRNsare leading the way. However, continuityof care is often blocked by the inabilityto gain privileges within the admittinghospital facility.While increased numbers of APRNswork within acute care settings, not allof them are employees of the facility.Many are contractors, employees ofphysicians with hospital privileges, orless often, independent practitioners.There is wide variation in how hospitalbylaws categorize and define health careproviders such as APRNs. APRNs maybe identified by category (e.g., nursepractitioner) or may simply be definedby a broad statement (e.g., health careprovider, health care professional,nonphysician provider). This creates aconfusing process for the credentialer.What Does It Mean to beCredentialed with HospitalPrivileges?Hospitals and other health care institutionsgrant medical professionals the privilege orauthority to practice in their facility.Credentialing and privileging wereoriginally applicable only to physicians.Physicians were granted the privilege ofadmitting patients to the facility with theauthority to order or perform all tests,diagnostic procedures, and treatments.When specialization of physicianpractice and board certification gainedacceptance and hospital accreditationbecame the norm, the need for a morespecialized privileging process alsoarose. Credentialing and privileging aretwo administrative processes that areintended to ensure that practitioners havethe necessary qualifications to directthe clinical care provided to patientsin hospitals. A hospital establishesrequired credentials for practitionersand then reviews, verifies, and evaluatesan applicant’s credentials—education,clinical training, certification, licensure,Hospital bylaws describe the credentialingand privileging process, spell out policiesand governance procedures, identify stafflevels of appointment, and provide therules and regulations for the hospital.Hospital bylaws will also designate levelsof medical staff privileges, such as active,honorary, consulting, affiliate, allied, andassociate. Bylaws can vary considerablyfrom one hospital to another even in thesame city or state.Hospital bylaws typically followthe standards and guidelines of theJoint Commission on Accreditationof Healthcare Organizations (JointCommission), which accredits U.S.health facilities. Starting in January2011, the Joint Commission requiresthat privileging of APRNs and physicianassistants (PAs) be carried out through the5
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital Privilegesprocess outlined in the Overview sectionof the Joint Commission’s Medical Staffstandards. In other words, facilities mustfollow the same privileging processthey use for physicians to credentialAPRNs and other medical staff, and notuse any “equivalent” process, whichwas previously acceptable.24 However,current Joint Commission standardspermit hospitals to privilege APRNs asless than active medical staff and withoutmedical staff membership. Only activemembers of the hospital’s medical staffare permitted to admit patients, and onlymedical staff members have voice andvote in medical staff governance. Withoutvoice and vote, APRNs can be voted offmedical staff rosters individually andcategorically without recourse.be composed of other practitionersappointed by the governing body.”“(c) Standard: Medical staff bylaws.The medical staff must adopt andenforce bylaws to carry out itsresponsibilities. The bylaws must:(5) Include a requirement that aphysical examination and medicalhistory be done no more than7 days before or 48 hours after anadmission for each patient by adoctor of medicine or osteopathy.”The Medicare requirement that only aphysician may conduct a history andphysical is duplicative and unnecessary.APRNs are qualified to conduct medicalhistories and perform physical examsthrough their education, certification,and experience. Medicare reimbursesAPRNs for performing these servicesin outpatient settings. Although thisregulation applies specifically toMedicare, it is frequently applied topatients with Medicaid and privateinsurance as well. This regulation iscostly and burdensome to hospitals,physicians, and patients. APRNs canand should document medical historiesand perform physical examinations inhospitals in addition to the other settingswhere they are licensed to practice.Federal and state laws and regulationsare additional barriers to hospitalprivileges for APRNs. These barriers areoutlined in the following sections.Medicare Regulations PreventAPRNs from Conducting PatientExams in HospitalsMedicare regulations allow APRNsmedical staff membership if permittedby state law but do not mandate APRNmembership. The Medicare HospitalConditions of Participation (CoP) containbarriers to APRNs obtaining hospitalclinical privileges. Pertinent Medicareregulations include the following:State Laws are a Barrier forAPRNs and Their PatientsThe Medicare Hospital CoP specify that ahospital’s medical staff may include otherpractitioners such as APRNs if permittedby state law. In the 1970s, Oregon wasthe first state to allow CNMs, and thenNPs, hospital privileges.26 The law statedthat NPs were subject to the credentialinginstitution’s bylaws and that a hospitalcould limit the scope of practice, requiremonitoring by physicians, or require thatNPs co-admit with a physician. Since thattime, many states have enacted similarlegislation.42 C.F.R. 482.22 Condition ofparticipation: Medical staff25“The hospital must have anorganized medical staff thatoperates under bylaws approvedby the governing body and isresponsible for the quality ofmedical care provided to patientsby the hospital. The medicalstaff must be composed of doctorsof medicine or osteopathy and, inaccordance with State law, may also6
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital PrivilegesThe Pearson Report, an annual state-bystate review of NP legislation, queries eachstate regarding legislative prohibitionsagainst hospital privileges. The 2011Pearson Report identified two states thatprohibited NPs from hospital privileges.Ohio law prohibits NPs from admittingpatients, and Maine law requires NPsto be supervised by a physician whenproviding patient care in the hospital.Even where state law does not prohibithospital privileges, hospitals may stillnot grant privileges (e.g., Florida). Onlya few states address inclusion of APRNsas part of medical staff, and variationsof state laws may not be consistent withnursing regulations regarding scope andauthority of APRNs. In Arizona, forinstance, the nurse practice act includesadmitting privileges to acute care facilities.The Arizona Department of Health rules,however, state that all patients admittedto a hospital must have an attendingphysician.27Nurse Practitioner Elected MedicalStaff PresidentBob Donaldson is clinical director ofemergency medicine and presidentof the medical staff at EllenvilleRegional Hospital in New York. Hiscurrent projects sound much like anymedical staff president’s goals. Whatmight surprise you is that Donaldsonis not a physician but a nursepractitioner. He was elected to thisinfluential position by his physiciancolleagues and enjoys great supportfrom the hospital’s medical staff.As an admitting provider in the ER,the hospital’s medical staff got toknow Donaldson well and in 2008he was invited to be on the teamto review and revise the medicalstaff bylaws. “The medical staff, allphysicians, voted to give equal rightsto nurse practitioners on the medicalstaff,” says Donaldson. “Whichmeans if you have a practice hereand you are involved in admissionsto this hospital, that you are equalto a doctor as far as privileges at thefacility and within the medical staff.”Hospital Bylaws Are a Barrier forAPRNs and Their PatientsEach hospital’s bylaws specify whetherand how APRNs may be grantedprivileges. Since almost all hospitals areaccredited by the Joint Commission,hospital bylaws typically follow the JointCommission standards. In 1983, theJoint Commission opened medical staffmembership to nonphysician health careprofessionals, including APRNs, whom theCommission referred to as “limited licensepractitioners.”28In another unusual move, Donaldson’swork in the ER means he admitspatients to the hospital and its variousproviders every day, so the hospitaldecided to give him attending status.Donaldson says that in 2009 thehospital needed to fill the position ofmedical staff president and was havingdifficulty attracting volunteers. So heput his name in the hat. “I look at thatas like anything else nurse practitionershave done,” he says. “There’s a voidand we step in and we do the job. Sothat’s what I did.” Clearly, this hospitalhas collaborative practice figured out.Hospitals may decide not to credentialand privilege APRNs29; that is, theirbylaws may not address any nonphysicianproviders at all. If hospital bylaws doaddress APRNs, the bylaws may includeprovisions for supervision of APRNsthat are more restrictive than state laws.When physicians are required to superviseAPRNs, the physician’s workload andperceived liability increase. Whenphysicians are required to cosign allSource: Excerpted from Rebecca Hendren. “NursePractitioner elected Medical Staff President.”HealthLeaders Media (February 8, 2011). AccessedAugust 9, 2011. urse Practitioner Elected Medical Staff President.html7
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital PrivilegesAPRN orders, clinical care can be delayed.Inappropriate physician oversight increasescosts and can diminish quality.30orders, deliver the baby, and providepostpartum care independently withinthe scope of the CNM’s education andtraining. When CNMs have hospitaladmission privileges, women planning ahospital birth or requiring hospitalizationduring pregnancy can remain in amidwifery practice. No obstetricalinterventions should be mandated unlesswarranted by a woman’s condition. Whena pregnant woman’s condition warrantsreferral to a physician, the establishedrelationship between the woman andthe nurse-midwife can help the womanto understand and make decisionsabout interventions proposed by theobstetrical specialist and allows for bettercontinuity than if her care is assumed bya stranger.35 The Medicare requirementfor a physician-conducted history andphysical even for a normal delivery in ahospital adds costs when the woman’sinsurance coverage is through an insurerthat follows this Medicare precedent.Several hospitals have welcomed APRNs,developing strategies to integrate andcapitalize on their contributions. A fewhospitals have set up special models orcommittees to facilitate credentialingand incorporating APRNs within theinstitution while recognizing their uniquecontributions.31 One hospital created aChief of Advanced Practice position toformally recognize and manage APRNs,similar to the Chief of Medicine positionsthat have existed for physicians fordecades.32 These efforts help to educate allhospital staff on the valuable contributionAPRNs make to the health care systemand pave the way for full integration.Consumers Benefit when APRNsHave Hospital PrivilegesThe greatest benefit of APRN hospitalprivileging is continuity of care forpatients. A distinguished panel of the IOMexamined the record, conducted hearings,and issued a report recommending thatAPRNs be permitted to practice tothe full extent of their education andtraining, and that nurses be preparedand enabled to lead change and advancehealth.33 The IOM recommended thatAPRNs be eligible for hospital clinicalprivileges, admitting privileges, andhospital medical staff membership andalso be permitted to perform hospitaladmission assessments—documentingmedical histories and performingphysical examinations.Children and their parents benefit whenpediatric nurse practitioners in primarycare practices have hospital privileges.Continuity of care between primary careproviders and the hospital decreasesthe number of strangers children mustdeal with and improves provider-parenteducation and communication.36Patients with cancer and other chronicillnesses benefit when APRNs havehospital privileges. Many cancer patientshave multisystem, complex, chronicillnesses that require coordination not onlyto follow the various disease processes, butto manage the symptoms and emphasizepreventive and health promotion aspects.A recent literature review found thatcontinuity of cancer care is significantlyenhanced when primary care NPs andoncology NPs are involved in patient careacross settings. NPs assume a variety ofcancer-related roles, including cancerspecialists, educators, researchers, andconsultants, extending across settingsWomen benefit when they receivehospital care from CNMs. Certified nursemidwives’ patients have significantlylower rates of cesarean sections, fewerepisiotomies, and higher rates ofbreastfeeding compared to those caredfor by physicians.34 In a normal hospitaldelivery, a nurse-midwife can admit thewoman to the hospital, write medical8
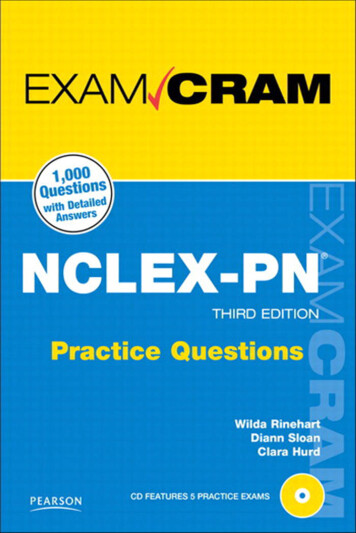
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital PrivilegesBenefits and Challenges Benefits–Expanding consumer choice and access to careImproving continuity of careIncreasing cost-effectiveness (decreased rehospitalizations, decreased medicationerrors, fewer C-sections, decreased duplication of services, to name a few)Improving interprofessional collaboration and team careImproving education of other professionals regarding APRNsIncreasing long-term survivorship in multisystem, chronic disease, andcomplex cancer patientsDecreasing patient stressors, especially for older, obstetric, and pediatric patientsProviding models for hospitals to use for credentialing APRNsUsing available health care workforce most efficiently to coordinate anddeliver care Challenges–Educating hospital boards, credentialing committees, and medical staff aboutthe practice of APRNs to assist in updating hospital bylawsEncouraging hospitals to increase the number of APRNs on hospitalcommittees/services that can make needed changesEducating consumers about their rights to continuity of care and transitional careAdvocating to hospitals that the primary care professionals of record be allowedaccess to the hospital records of their patients when the patient is admittedEncouraging patients/consumers cared for by APRNs to advocate for them ascompetent providers to both the physicians who care for them and the hospitalsto which they would be inclined to be admittedto radiation clinics, hospitals, oncologyclinics, and primary care settings.37medication regimens—often withprescriptions from several providers—andextensive changes in their medicationsduring hospitalization. Nearly20 percent of Medicare patients arerehospitalized within 30 days of an indexhospitalization.38 A recent transitional careprogram for heart failure patients led byAPRNs significantly reduced readmissionrates.39 These types of programs maybe expanded nationally as APRNs withhospital privileges coordinate care forvulnerable populations.Patients transitioning from hospitalsto community care benefit whenAPRNs have hospital privileges andcan minimize medication discrepanciesbetween settings. Findings from patientstransitioning from hospital to communityindicated that medication discrepancieswere astoundingly widespread, with94 percent of the participants having atleast one discrepancy. Older adults areparticularly vulnerable to medicationdiscrepancies following hospitaldischarge because they frequently havechronic comorbid medical conditions,functional impairments, complexInterprofessional collaboration is enhancedwhen APRNs have hospital privileges.Patients benefit when APRNs andphysicians learn from each other, improve9
Removing Barriers to Advanced Practice Registered Nurse Care: Hospital Privilegestheir respective practices, and gain a deeperunderstanding of one another’s expertiseand philosophy. This is the kind of practicethat patients are entitled to and deserve.increasing their numbers. In addition tothe shortage of primary care providers,the d
consumer choice, and improves health care quality. 1. This report discusses barriers to hospital privileges and expands on . recommendations of the Institute of Medicine (IOM) report . The Future of Nursing: Leading Change, Advancing Health. 2. that APRNs be eligible for hospital clinical pri