Transcription
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina IIISandro SiervoSUTURING TECHNIQUESIN ORAL SURGERYillustrations by LuisaLorenziniQuintessenza Edizioni S.r.l.Milano, Berlino, Chicago, Tokyo, Barcellona, Istanbul, Londra, Mosca,Nuova Delhi, Parigi, Pechino, Praga,San Paolo, Seul, Varsavia
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina XContentsSurgical wounds2 Introduction3 Tissue healing: general considerations and clinical aspects4 Tissue healing: cellular and molecular mechanisms11The physiology of wound healing: an overview11Inflammatory phase (days 0–3)12Proliferation or fibroblast phase (days 3–12)14The remodeling phase (days 6–14)15Wound healing: peculiarities of the gastroenteric tract16The role of growth factors in tissue healing17Sepsis and scar formation18Treatment of infected surgical wounds20Use of growth factors in clinical practice20The role of integrins in re-epithelialization23 Classification of wounds25 Tissue reactions to sutures27
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina XITechnological aspects34 Suture needles35Technological and commercial characteristics of suture needles35Suture needle anatomy39Optical microscopic analysis of suture needles on the market50 Sutures: general characteristics and able sutures60Non-resorbable sutures63Suture removal64Packaging65Optical microscopic analysis of the junction between needle and suture thread67Auxiliary materials72 Instruments for use in oral-surgery procedures73Needle holders73Forceps75Scissors77 Gripping needle holders and scissors80
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina XIIContentsClinical applications82 Interrupted sutures83CASE 185The interrupted suture88The full surgeon’s knot90The full lock knot or Toupet’s knot93CASE 295 The single stitch continuous sutureThe simple or spiral continuous suture9799The locked continuous suture104The locked and secured continuous suture109 The mattress suture113CASE 3116CASE 4118CASE 5119The external horizontal mattress suture122The external vertical mattress suture124The buried horizontal mattress suture126The buried vertical mattress suture132CASE 6142 Suturing on more than one plane145Coronal seal of the mattress suture145CASE 7145CASE 8150Single stitch associated with the external horizontal mattress suture153
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina XIIISingle stitch associated with the external vertical mattress sutureThe Gottlow suture155157The horizontal Gottlow suture158The vertical Gottlow suture159The figure-of-eight suture161The figure-of-eight suture: step by step technique162 The anchored suture165CASE 9166CASE 10168The simple anchored (sling) suture170The sliding anchored (sling) suture174CASE 11177CASE 12179The criss-cross anchored suture182The “H”, “U” and “X” anchored sutures186The continuous sling suture193 Protective sutures199CASE 13199CASE 14200Cornick’s suture203 A word about nerve suturing206Quick Reference Guide210Bibliography224Index233
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina VIIPrefaceThe great surgeon has just successfully completed a delicate operation; he removes his gloves and gives afew suggestions to his collaborators as they begin closing the access route. Having sutured the deeperplanes in their turn they leave the skin suturing to the youngest member, who is still specializing. Thus aphase of surgery that, in some branches, is a fundamental one is left in the least expert hands. Suturing theaccess route has always been neglected, put in place quickly and no more than adequately, while in oralsurgery, and obviously in facial surgery, it is of fundamental importance. Whereas in the latter field theesthetic consequences of a badly executed suture can readily be understood, for many operations in oralsurgery proper suturing determines success. How many bone grafts have become infected because thesuture did not provide a proper seal? How many exposed membranes or gingival recessions are linked to atechnical defect in suturing? For these reasons I particularly appreciate the work of Siervo and collaborators,who have tackled the subject, and given the suture the role it deserves.The argument is treated with a clear and rational approach, including the indispensable biologicalaspects required to understand the various problems, and with illustrations that make even the lessunderstandable details clear. So it is with great pleasure that I present this book, the latest undertaking ofSandro Siervo, whose serious and committed approach to all the problems he has dealt with I have come toappreciate greatly since I first met him.I am sure that this book will have great success, that its readers will appreciate its message, and that itwill have a positive influence on day-to-day surgical practice.Roberto Brusati
Cap00 - Siervo Introd4.qxp7-11-200710:22Pagina VIIIwith collaboration from:Samuele Burastero Doctor of Medicine and Surgery, Specialist in Pneumology, Specialist inImmunology, Researcher at the San Raffaele Hospital, MilanCristian CorainiDoctor of Dentistry and Dental Prosthetics, Private Practitioner in MilanEnrico CerriDoctor of Medicine and Surgery, Specialist in Dentistry, Private Practitioner in MilanCarlo MarchettiDoctor of Medicine and Surgery, Specialist in Dentistry, Private Practitionerin Morbegno and MilanLuigi PagliaDoctor of Medicine and Surgery, Specialist in Dentistry, Head of the Children’sDentistry Department, Instituto Stomatologico Italiano.Massimo RadiciDoctor of Dentistry and Dental Prosthetics, Private Practitioner in MorbegnoPaolo SiervoDoctor of Medicine and Surgery, Specialist in Maxillo-Facial Surgery, PrivatePractitioner in MilanRaffaele SiervoDoctor of Medicine and Surgery, Specialist in Dentistry, Private Practitioner in Milan
Cap01 - Siervo Le Fer4.qxp7-11-200710:27Pagina 2Suturing techniques in oral surgerySURGICAL WOUNDS
Cap01 - Siervo Le Fer4.qxp7-11-200710:27Pagina 3Introductionhe importance of soft-tissue managementsynthetic or a natural thread, a single or a multipleis today an absolute priority in any intra-filament, a resorbable or a non-resorbable suture,and extra-oral surgical procedure if amust be reasoned and never left to chance. Thecorrect esthetic and functional result is to be achieved.thread is always used with a needle,the characteristicsThere are at least two aspects that are of equalof which also contribute to differentiating its use inimportance in reaching this goal: on one hand theorder to achieve the required results. A precisedesign and consequent management of the flap,andknowledge of these variables is part of the body ofon the other hand the suturing technique.technical and theoretical expertise of every oralTThe development of infections along the line ofsurgeon; the goal of this book is to provide usefulthe incision is potentially a dangerous post-operativeindications for the most appropriate choice inevent.Some infections that affect the wound marginsdifferent clinical situations.in certain areas of the body may put the prognosis,inThe primary function of sutures is to help toterms of the patient's life, at serious risk. In lessstabilize the flap during the healing phases withoutdramatic situations they in any case delay healing ofimposing needless traction on the soft tissue. Thethe tissues involved in the surgery. The suturingsuturing technique is thus chosen according to itsmaterials and techniques used to reconstruct thecharacteristics.These characteristics,in the individualplanes can thus have a direct and determinatecircumstances, enable the flaps in question to beinfluence on the phases of healing, making an in-everted or to be introflected, or make it possible todepth and detailed knowledge of the physical,exercise compression on the surrounding tissues inchemical and technological properties of suturingorder to ensure hemostasis, or again to create a sealmaterials an absolute necessity. The clinical choiceon the different planes to guarantee their hermeticthat,on each individual occasion,leads us to prefer aclosure.The aim is always to optimize the functional
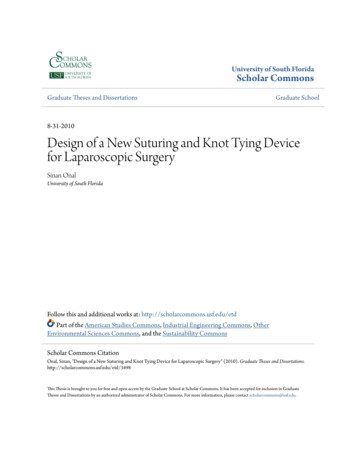
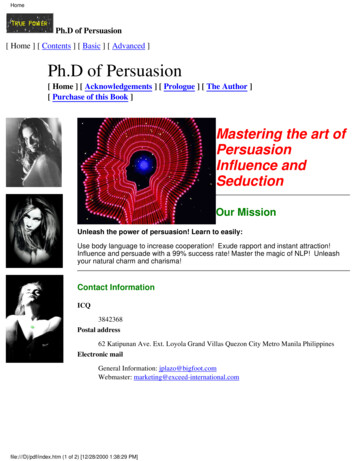
Cap04 - Siervo Applic4 copia.qxp7-11-200712:35Pagina 176C L I N I C A L A P P L I C AT I O N SBy passing beneath the periosteum, the suture canbe anchored and thus attached.176If the full surgeon’s knot is placed moreapically on the vestibular side, thevestibular flap will be displacedapically. This suturing technique isindicated in resective periodontaltherapy, where the suture helps toreposition the flap apically.The thread passes completely outside the flap to reachthe palatal side. Here it pierces the flap from the outsideinwards, again engaging the periosteum. The flap maybe pierced more coronally and the needle can leavemore apically, or the entrance hole can be more apicaland the exit hole more coronal. Both methods arecorrect, although the second is easier to perform.Anchorage to the palatal periosteum is the secondanchorage point to attach this suture.If the knot is positioned at the levelof the cemento-enamel junction, theflap will be passive with no tendencyto displacement.If the knot is positioned palatally,the suture will displace thevestibular flap coronally. This typeof flap displacement is preferablewhen the tooth in question hasundergone regenerative surgery.
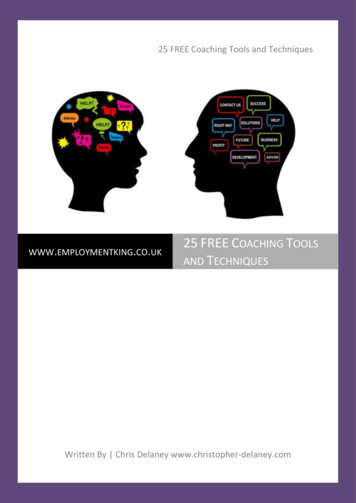
Cap04 - Siervo Applic4 copia.qxp7-11-200712:35Pagina 177CASE 11Case 11Clinical documentation illustrates the great utility ofthis type of suture. The treatment plan in this caseentailed resective periodontal therapy in order todecrease the depth at probing.After having resected a mixed-thickness flap (fullthickness at the more coronal part and halfthickness at the more apical part) the root surfacesand the bone defects are surgically cleansed.177Using rotating instruments, the bone surround ismodified, taking particular care to reconstruct acorrect bone anatomy.Suturing begins high up in the vestibule, well abovethe muco-gingival line, with the needle enteringperpendicular to the underlying bone and piercingthe periosteum, where it finds a point of anchorage.
Raffaele Siervo Doctor of Medicine and Surgery, Specialist in Dentistry, Private Practitioner in Milan Cap00 - Sierv