Transcription
An Illustrative Review ofParotid PathologyJared Kirkland, M.D.Scott McCusker, M.D.David Douglas, M.D.Maria Gorospe, M.D.William T. O’Brien, Sr., D.O.1David Grant Medical Center,Travis Air Force Base
Disclosures The authors have no related financialdisclosures or conflicts of interest “The views expressed in this material arethose of the authors and do not reflect theofficial policy or position of the U.S.Government, the Department of Defense, orthe United States Air Force”2
ObjectivesFollowing this presentation, one will be able to understand: Normal boundaries and associated structures of theparotid glands Imaging patterns and appearances of variousinflammatory, infectious, obstructive, and autoimmuneprocesses of the parotid glands Clinical and multi-modality imaging manifestations ofcommon benign and malignant parotid neoplasms Characteristic findings associated with congenital cysticand vascular lesions of the parotid glands3This presentation is best suited for radiologists in training andradiologists seeking a refresher of various parotid pathologies
The Parotid Gland Parotid gland is the largest salivary gland It has the highest incidence of pathologyamong the major salivary glands– Benign processes far outweigh malignant processesin terms of incidence Imaging is useful in:– Determining the morphology of parotid lesions andpotential etiologies– Surgical planning for resection– Evaluating extent of malignant spread, if present4
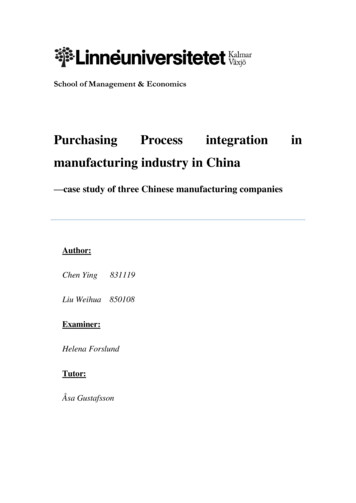
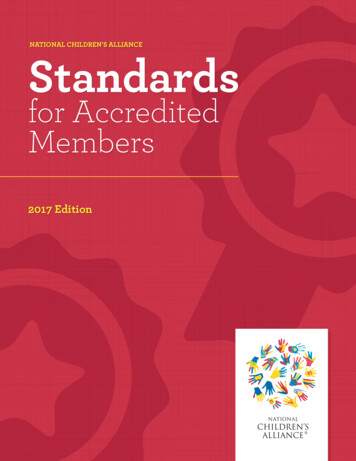
Parotid Gland AnatomyBoundaries of Parotid Gland Posterolateral to massetermuscle & mandible Anterior to mastoid process Medial margin extends thrustylomandibular tunnel withdeepest portion positioned inthe prestyloid compartment Surrounded by superficiallayer of the deep cervicalfascia5T1 Axial image highlighting the parotid gland(*) and its boundaries
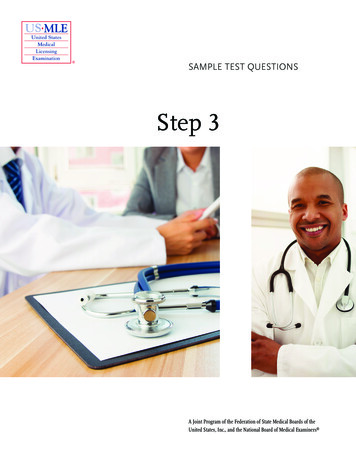
Parotid Gland AnatomyAssociated Structures Parotid (Stenson’s) Duct– Arises anteriorly from the parotid gland– Parallel course to masseter before turning mediallyto pierce buccinator & oral mucosa at level of the2nd molar Facial vein– Divides parotid gland into superficial and deeplobes Facial Nerve– Often difficult to visualize extracranial segments– Exits styloid foramen lateral to styloid process andposterior belly of the digastric muscle– Pierces posterior aspect of parotid gland– 5 branches arise while traversing parotid gland6T1 & T2 axial images of parotid glandhighlighting associated structures
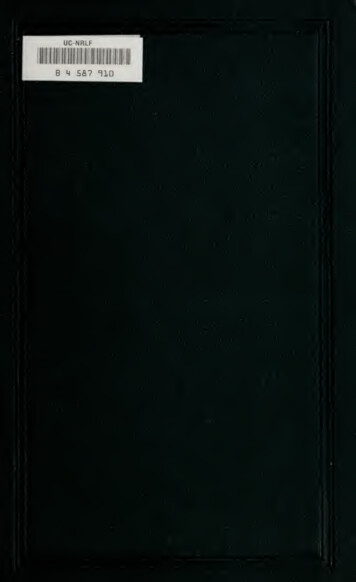
Pathology of the ParotidParotitis– Infectious– Sialolithiasis/ Obstructive– AutoimmuneAIDS-related parotid lesions– Benign lymphoepitheliallesions (BLELs)Tumors– Benign– MalignantCongenital lesions– First Brachial Cleft Cyst– VenolymphaticMalformation7Axial contrast enhanced CT MIPshowing a large left parotid mass
Parotitis Refers to Inflammation ofparotid gland caused by:– Viral or bacterial infection May be acute or chronic– Ductal obstruction Obstructing mass (e.g.sialolithiasis) Scarring of the parotid duct– Autoimmune diseases Sjögren Disease, Lymphoepitheliallesions (LELs) May be acute or chronic– Chronic inflammation leads toglandular fibrosis & atrophy8Axial contrast enhanced CT showing anenlarged left parotid gland with surroundinginflammation
Infectious ParotitisImaging CT, MRI and Ultrasoundshow similar features:– Enlargement of gland– Hyperemia/enhancement– Surrounding inflammation Viral causes have apredilection for bilateralinvolvement Bacterial etiologies typicallyunilateral & more likely tohave surroundinginflammation withsuppurative lymph nodes9Coronal & axial contrast enhanced CT imagesshowing an enlarged, hyperenhancing leftparotid gland and suppurative adenopathy
SialolithiasisBackground Refers to calcification within a salivary duct More common in submandibular duct, butalso affects the parotid duct May form anywhere along the duct or withinthe parotid gland When large enough, the calcification canobstruct the duct and result in inflammation10
Parotid SialolithiasisImaging Calcification along course of parotidduct best seen on CT– May also be seen on ultrasound With obstruction, often see:– Dilatation of parotid ductproximal to stone– Inflammation, enlargement, &hyperenhancement of gland MRI valuable for determining if theobstruction is acute or chronic– Acute: Increased T2 signal dueto inflammation– Chronic: Increased T1 due tofatty glandular atrophy11Axial CT image showing a calcified stone within theproximal aspect of the parotid ductGrayscale sonographic image of same patient with adilated parotid duct & heterogeneous echotexturewithin the parotid gland tissue
Parotid SialolithiasisImaging: MRIWith permissions: O’Brien WT. Top 3 Differentials in Neuroradiology. Thieme, 2015T2 and enhanced T1 fat sat images show enlargement, increased T2 signal &enhancement of the right parotid gland, as well as dilatation andinflammation along Stenson‘s duct; a T2 hypointense obstructing stone isseen within the distal duct12
Sjögren SyndromeBackground Autoimmune disease with cellmediated destruction of salivary &lacrimal glands Results in xerostomia &keratoconjunctivitis sicca Anti-Ro and Anti-La antibodies Chronic lymphocytic inflammationincreases risk for non-HodgkinlymphomaLow PowerPathologic Findings Infiltrative lymphoid tissue Interfollicular plasmacytosis Interstitial fibrosis and acinaratrophy13High PowerH&E stain showing infiltration of lymphocyteswhich appear to be destroying salivary glandacini while sparing the ductal epithelium
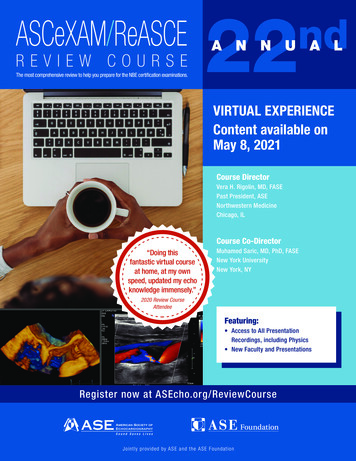
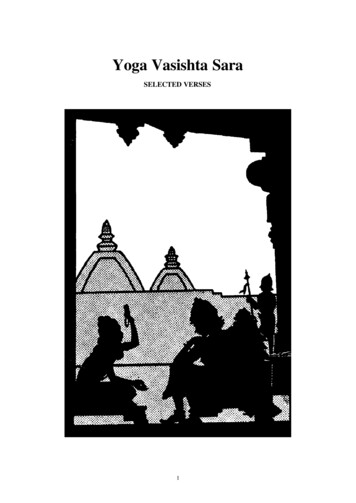
Sjögren SyndromeImaging Early appearance showsdiffuse small parotid cysts Subsequently, solidintraparotid lesions developalongside cysts End stage disease showsglandular atrophy with fattyreplacement and/or fibrosis Findings best visualized on MRI– T2 hyperintense cysts– Eventual decreased T1 & T2signal due to fibrosis14Axial & coronal T2 fat-sat images showinginnumerable bilateral T2 hyperintense parotidcysts in a patient with Sjögren syndrome
AIDS-related Parotid LesionsBackground Benign lymphoepithelial lesions(BLELs) occur in 5% of AIDS patients Results from lymphoid hyperplasiaPathologic findings See lymphoid hyperplasia, cysts, &intraparotid ductal dilatationCourtesy of Richard Latchaw, M.D.Imaging Bilateral mixed cystic and solid parotidlesions of varying sizes Cervical adenopathy commonly seen Prominent adenoidal tissue (commonin AIDS)15Coronal contrast enhanced CT and T1 MR imageshighlighting numerous hypodense (CT ) and T1hypointense (MR) cysts involving both glands,representing lymphoepithelial lesions
Common Parotid Tumors16BenignMalignant PleomorphicAdenoma Warthin Tumor MucoepidermoidCarcinoma Adenoid CysticCarcinoma Lymphoma
Parotid Tumors 85% of salivary gland neoplasms occur in theparotid glands 80% are benign, 20% malignant Clinical presentation typically not useful indistinguishing between benign & malignantdisease17
Pleomorphic AdenomaBackground Also known as benign mixed tumorMost common parotid neoplasm (80%)Typically presents between 40 and 60years of age as a painless palpable massMost often located within thesuperficial lobe, but may involve thedeep lobe as wellCan occasionally degenerate intocarcinomaPathologic findings 18Biphasic epithelial & mesenchymal cellsEpithelial cells may be spindled orroundedStroma is usually myxoid or chondroidLow PowerLow PowerHigh PowerH&E stain showing a well circumscribedbiphasic nodule with a mixture of blandround epithelial cells, spindled myoepithelialcells and a background of myxoid stroma
Pleomorphic AdenomaImaging US– Hypoechoic ovoid or lobularlesion– /- posterior acousticenhancement CT– Solid ovoid mass withhomogeneous & oftendelayed enhancement MRI– T1 hypointense ovoid mass– T2 hyperintense– Homogenous enhancement19Axial & coronal contrast enhanced CT images of apleomorphic adenoma showing an ovoid enhancingmass in the superficial right parotid lobe
Pleomorphic AdenomaImaging: MRIAxial MR imaging showing an intraparotid mass that is T2hyperintense, T1 hypointense, and enhances following contrastadministration20
Warthin TumorBackground Benign parotid tumor Also referred to as papillarycystadenoma lymphomatosum 2nd most common salivarygland tumor Typically diagnosed between 60and 70 years of age Strong association with smoking Slow painless growth, typicallyin the tail of the parotidLow PowerPathologic Findings Double layer of epithelial cellsoverlying lymphoid stroma May develop papillaryprojections or fluid-filled cysts21High PowerH&E stain with low and high power microscopy. Thisencapsulated lesion is composed of oncocytic cells withtrademark “double layers”. The stroma consists oflymphocytes with germinal centers. Small cysts are present.
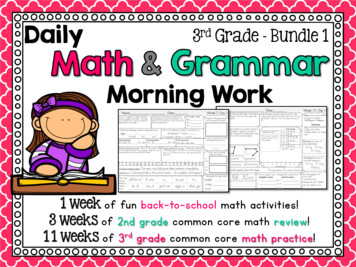
Warthin TumorImaging 22Ultrasound:– Ovoid mass with hypoechoic solidcomponent & hypo- to anechoic cysticcomponents– Solid components often demonstrateinternal vascular flowCT:– Ovoid cystic & solid mass with mildenhancement of solid componentsMRI:– Solid portion of mass is T1 hypointense– Cystic component often T2 hyperintensebut variable based on proteinaceouscontent– Minimal-mild enhancementGrayscale sonographic images showing anovoid/lobular anechoic lesion with a hypoechoicsoft tissue component peripherally
Warthin TumorAxial enhanced MIP & coronal CT images showing acystic and solid mass within a fatty parotid gland23
Mucoepidermoid CarcinomaBackground Most common salivary gland malignancyTypically diagnosed between 30 and 60 yearsof ageSlight female predominancePatients usually present with a painless andpalpable massHigh-grade lesions may present with painassociated with extraglandular spread,perineural invasion, or intracranial extensionLow PowerPathologic Findings Clustered cords of squamous, mucous, orintermediate cellsOccasional sebaceous or goblet type cells– Inflammatory reaction to mucin or keratin24High PowerH&E stain show a macro and microcystic mass withgoblet cells, mucin pools, and bland intermediate cells
Mucoepidermoid CarcinomaImaging Solid mass with varying degree ofcystic change, if present May have circumscribed orirregular (high grade) borders Ultrasound:– Heterogeneously hypoechoic CT– Hyperdense with enhancement ofsolid components MRI– T1 hypointense and T2 intermediateto hyperintense– Enhancement of solid components25Enhanced CT images showing a lobular,peripherally enhancing mass within thesuperficial left parotid lobe
Mucoepidermoid CarcinomaImaging: MRI High grademucoepidermoidcarcinomaAxial T1 and coronal T2 fat sat imagesdemonstrate a superficial parotid mass withirregular borders & increased T2 signal intensity26
Adenoid Cystic CarcinomaBackground 2nd most common primary parotidmalignancy Peak incidence between 40 and 60years of age High risk for perineural invasion– Symptoms of facial pain or facialnerve paralysisLow PowerPathologic Findings Cribriform, solid, or tubular pattern Small bland myoepithelial cells withscant cytoplasm & dark compactangular nuclei PAS excess basement membranematerial & mucin Peripheral perineural invasion27High PowerH&E Stain showing a proliferation of blandmyoepithelial cells forming the classic cribriform (or“punched-out” cyst-like) ductal structures whichare filled with mucoid material
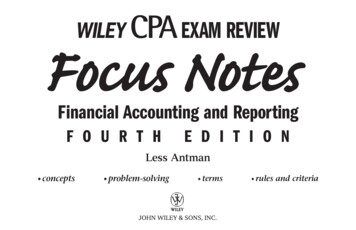
Adenoid Cystic CarcinomaImaging Often has irregular margins US– Hypoechoic mass– /- posterior acousticenhancement CTUS imaging showing a hypoechoic parotid mass withangulated margins– Homogeneously enhancingparotid mass– May have smooth orirregular borders MRI– Low signal on T1– Moderate T2 hyperintensity– Homogeneousenhancement28Contrast enhanced T1 weighted images show an irregularlymarginated & diffusely enhancing mass involving thesuperficial and deep parotid lobes
Parotid LymphomaBackground Malignant lymphomatous involvement ofparotid gland–– Non-Hodgkin lymphoma, or less commonly:Primary parenchymal type (MALT)Risk factors–––ImmunodeficiencyAutoimmune diseases, including SjögrensyndromePrior radiation treatmentLow PowerPathologic findings 29Microscopic features vary depending onlymphoma subtype, but are morphologicallyand immunophenotically similar to the nodalcounterpartsDepending on the subtype, microscopy showsproliferation of small mature or largerimmature cellsHigh PowerH&E stain showing an intraparotid lymph node withproliferation of small mature lymphocytes witheffacement of the normal lymph node architecture.Lesional cells demonstrated an immunoprofilecompatible with chronic lymphocytic lymphoma.
Parotid LymphomaImaging May be solitary, multiple,unilateral, bilateral, or diffuse Often see associated cervicaladenopathy Ultrasound– Hypoechoic mass(es)– /- Hypervascularity on colorDoppler CT– If nodal type, nodes will bediscrete masses with moderateenhancement– If parenchymal, will see illdefined infiltrative solid mass MRI30– Intermediate signal on T1 &variable but often intermediateto low signal on T2 withmoderate enhancementAxial enhanced CT images showing a largemass infiltrating the right parotid gland withassociated conglomerate cervical adenopathy
Developmental Lesions First Branchial Cleft CystBackground Results from abnormal closure of developmentalbranchial cleft First branchial cleft cysts:– Second most common branchial cleft anomaly after the farmore common 2nd branchial cleft cyst– Occur anywhere from the external auditory canal to the angleof the mandible Commonly located within the parotid gland– May have a draining sinus tract to the external or middle ear Risk of:– Superinfection– Mass effect on adjacent structures31
First Branchial Cleft CystImaging Oval, round, or lobulated cystic mass US:– Anechoic to hypoechoic– Posterior acoustic enhancement CT:– Simple fluid density– Thin wall MRI:– High T2 signal intensity– Variable T1 signal based on proteincontent No enhancement unlesssuperinfected; then may seeperipheral and surroundinginflammatory enhancement32Axial contrast enhanced CT imageshowing a hypodense, nonenhancingcystic mass within the left parotid gland
Venolymphatic MalformationBackground Spectrum of venous & lymphaticdevelopmental abnormalities Lesions often cross fascial planes toinvolve multiple spaces of the neckImaging Venous malformations avidly enhance– May contain flow voids– Presence of phlebolith is consideredpathognomonic Lymphatic malformations may beunilocular or multilocular– Fluid-fluid levels, due to hemorrhage,are characteristic– Peripheral & septal enhancement morepronounced with superimposedinfection Many cases demonstratecharacteristics of both33Axial T2 fat sat image showing a multi-loculatedcystic mass on the right involving multiplespaces of the neck, including the parotid space;fluid-fluid levels with different signal intensitiesare consistent with intralesional hemorrhage.
Summary A variety of pathologic processes affect the parotid glands Common congenital lesions include a Type 1 branchial cleft cyst andvenolymphatic malformation– Congenital lesions may be complicated by infection of hemorrhage Inflammatory parotitis may result from an infectious process, autoimmunedisorder, or ductal obstruction– Viral parotitis and Sjögren are typically bilateral processes– Bacterial parotitis and ductal obstruction are typically unilateral Benign lymphoepithelial lesions are not uncommon in AIDS patients– Often see associated adenopathy and prominent adenoidal soft tissue The majority of parotid neoplasms are benign with pleomorphic adenomabeing the most common– Irregular margins suggest malignancy over a benign lesion It is essential to have a working knowledge of the imaging manifestationsof parotid lesions, as imaging plays a key role in work-up and management34
References 35Abdullah A, Rivas FFR, Srinivasan A. 'Imaging of the Salivary Glands.’ Semin Roentgenol 48.1(2013): 65-74. Web. 13 Nov. 2015.Bialek EJ, Jakubowski W, Zajkowski P, et al. 'US of the Major Salivary Glands: Anatomy andSpatial Relationships, Pathologic Conditions, and Pitfalls.’ RadioGraphics 26.3 (2006): 745-763.Web. 13 Nov. 2015.Burke CJ, Thomas RH, Howlett D. 'Imaging The Major Salivary Glands.’ Br J Oral MaxillofacSurg 49.4 (2011): 261-269. Web. 13 Nov. 2015.Cheng L, Bostwick DG. Essentials of Anatomic Pathology. New York: Springer, 2011. Print.Dispenza F, Cicero G, Mortellaro G, et al. 'Primary Non-Hodgkins Lymphoma of the ParotidGland.’ Braz J Otorhinolaryngol (Impr.) 77.5 (2011): 639-644. Web. 13 Nov. 2015.Dubois J, Soulez G, Berthiaume MJ, et al. 'Soft-Tissue Venous Malformations In Adult Patients:Imaging and Therapeutic Issues.' RadioGraphics 21.6 (2001): 1519-1531.Hellquist HB, Skálová A. Histopathology of the Salivary Glands. New York: Springer, 2014. Print.Kumar V, et al. Robbins Basic Pathology. Philadelphia, PA: Elsevier/Saunders, 2013. Print.Shekar K, Singh M, Godden D, et al. 'Recent Advances in the Management of Salivary GlandDisease.’ Br J Oral Maxillofac Surg 47.8 (2009): 594-597. Web. 13 Nov. 2015.Yousem DM, Kraut MA, Chalian AA. 'Major Salivary Gland Imaging1'. Radiology 216.1 (2000): 1929. Web. 13 Nov. 2015.
Contact InformationJared Kirkland, M.D.Captain, USAF, MC––––36Address: 101 Bodin Circle, Travis AFB, CA 94535Office phone number: (707)-423-7182Work email address: jared.kirkland.2@us.af.milPersonal email address: jared.kirkland@gmail.com
An Illustrative Review of Parotid Pathology Jared Kirkland, M.D. Scott McCusker, M.D. David Douglas, M.D. Maria Gorospe, M.D. William T. O’Brien, Sr., D.O. 1 David Grant Medical Center, T