Transcription
Oral Pathology: A Clinical Review4 Credit Hours (4 CEs)Materials fromUnited States Air Force 2013Instructional Materials in the Public Domain for Dental ProfessionalsWith updates from Oral Cancer Foundation from 2019Revised and updated by Megan Wright, RDH, MSPublication Date: October 2012Updated Date: February 2020Expiration Date: February 2023The Academy of Dental Learning and OSHA Training, LLC is an ADA CERP RecognizedProvider. ADA CERP is a service of the American Dental Association to assist dentalprofessionals in identifying quality providers of continuing dental education. ADA CERP does notapprove or endorse individual courses or instructors, nor does it imply acceptance of credit hoursby boards of dentistry.Conflict of Interest Disclosure: ADL does not accept promotional or commercial funding inassociation with its courses. In order to promote quality and scientific integrity, ADL's evidencebased course content is developed independent of commercial interests. Refund Policy: If youare dissatisfied with the course for any reason, prior to taking the test and receiving yourcertificate, return the printed materials within 15 days of purchase and we will refund your fulltuition. Shipping charges are nonrefundable.California Registered Provider Number: RP5631
Answer Sheet: Oral Pathology Clinical 4.19.24.5.10.15.20.25.Name: Profession:License State: License Number: Expiration DateAddressCity: State: Zip Code:Telephone: Fax:E-mail:If you have downloaded the course and printed the answer sheet from the Internet please enterpayment information below.Card type: Card Number:Exp. Date: Name as it appears on card:*To enter your answers online you MUST return to our website www.dentallearning.org.Return answer sheet: Via fax: 518.514.1103Via email: CESupport@dentallearning.comPostal Mail: ADL, PO Box 14585, Albany, NY 12212***PLEASE PRINT CLEARLY; ILLEGIBLE ANSWER SHEETS WILL NOT BEPROCESSED.Notes:1
Course EvaluationPlease place an X in the box to rate thesestatements:PoorFairGoodVeryGoodExcellentThe content fulfills the overall purpose of the course.The content fulfills each of the course objectives.The course subject matter is accurate.The material presented is understandable.The teaching/learning method is effective.The answers to the test questions are appropriatelycovered in the course.How would you rate this course overall?Hours:Time to complete the entire course and the test?Minutes:GoogleOther Search EngineFriend/CoworkerOtherDo you have any suggestions about how we can improve this course? If so please note them on aseparate sheet of paper and send it in with your answer sheet.If you studied the course online, did all the links work? If not please note the page and link on a separatesheet of paper and send it in with your answer sheet so we can fix it.2
Instructions1. Review the Objectives: Objectives provide an overview of the entire course.2. Read the course material.3. Complete the test:a. Return to our website: www.dentallearning.org, click on Take the Exam,enter your answers, register, if you are new customer (existing customerslogin), pay for the course, click Grade Test. Your test will be gradedimmediately. If required, complete the course evaluation. Your certificatewill display for you to print.b. If you would rather, you may return your completed answer sheet andcourse evaluation to us via the options listed below.To successfully complete the course you must score 80% or above on the test. If youdo not score 80% you may retake the test one more time free of charge. If you fail asecond time you must purchase a new course and test.If you’ve downloaded this coursebook off the Internet you can: Return to our website (www.dentallearning.org) to take the test online (only if youhave not purchased the coursebook separately). You will need to provide creditcard information at the time you submit your test online for scoring. Write your answers on the one-page answer sheet included in this book,complete the credit card payment information, and return the form to the addressbelow, fax, or email address below. Or, you may send a check or money order tothe address below with your answer sheet.Academy of Dental Learning and OSHA Training, LLC (ADL)P.O. Box 14585Albany, NY 12212Fax: 518-514-1103Email: CESupport@dentallearning.orgAnswer sheets received without payment will not be processed.We grade all tests in a timely manner; if you do not receive your certificate within fivedays, please email (CESupport@dentallearning.org) or call us: 518-209-9540.There is no time limit for return of your answer sheet. Completion dates are taken fromthe envelope postmark or the finish date recorded in the computer when you do anonline exam. Tests MUST be completed in the licensing cycle you wish to use thecredits.If you are dissatisfied with the course for any reason, prior to taking the test andreceiving your certificate, return the printed materials within 15 days of purchase and wewill refund your full tuition. Shipping charges are nonrefundable.3
If someone else would like to use this material after you are done, he or she mayregister with us and take advantage of a “sharing discount”. Courses downloaded fromthe Internet can be shared at the same tuition rate as currently available on our website.Please call us if you need an extra answer sheet or download one from our website.There is no “sharing discount” for online exams.The author and ADL have made every effort to include information in this course that isfactual and conforms to accepted standards of care. This course is not to be used as asole reference for treatment decisions. It is your responsibility to understand your legalobligations and license requirements when treating patients. ADL is not responsible forthe misuse of information presented in this course. The material in this course cannotbe reproduced or transmitted in any way without the written consent of ADL.4
Table of ContentsAnswer SheetEvaluationInstructionsTable of ContentsObjectivesIntroduction2016 Statistics on Worldwide OccurrenceOral Pathology Clinical Review1. Fibroma2. Pyogenic Granuloma3. Peripheral Ossifying Fibroma4. Peripheral Giant Cell Granuloma5. Gingival Overgrowth6. Gingival Cyst7. Benign Migratory Glossitis8. (Pseudomembranous) Candidiasis9. Apthous Ulcer10. Herpetic Stomatis11. Herpes Zoster (Shingles)12. Lichen Planus13. Pemphigus Vulgaris14. Pemphigoid15. Benign Mixed Tumor (Pleomorphic Adenoma)16. Mucoepidermiod/Ranula17. Dermoid Cyst18. Labial Melanotic Macule19. Racial Pigmentation20. Minocycline Staining21. Medication Induced Pigmentation22. Amelogenesis Imperfecta23. Opalescent Teeth24. Buccal Bifurcation Cyst25. Dentigerous (Follicular) Cyst26. Ameloblastoma27. Odontogenic Keratocyst (Odontogenic Tumor)28. Stafne Defect29. Paripical Cememto-Osseous Dysplasia (PCOD)30. Idiopathic Osteosclerosis31. Bisphosphonate Related Osteonecrosis of the Jaw (BRONJ)Oral Cancer and Technology in ResearchConclusionReferencesCourse 9293030313233343537373839434344
ObjectivesUpon completion of this course, the student will: Remember major examples of oral pathology included in the course survey.Recognize the major characteristics of the types of oral pathology aspresented.Understand major aspects of differential diagnosis (DDX).Know major aspects of treatment, management, and prognosis.Improve diagnostic knowledge of radiographic interpretation.Know specific points to communicate to patients about prognosis.IntroductionThe practice of dentistry is an application of art and science. In everyday practice, thedental practitioner reviews many cases of suspected pathology, and while some casepresentations are very common, others are not common. This course is a refreshercourse of fairly common oral pathology conditions. A very strong background in clinicaldental practice is assumed for this course. The course is most suitable for dentists anddental hygienists who want a good review with clinical case presentations andradiographs to support the text. However, the course would be a useful summary andreview for all members of the dental team who want to familiarize themselves with anoverview oral pathology in clinical practice. This course is ADA CERP approved for 4hours of continuing education credit, and fulfills credit hours toward license renewal.Individuals must check with their state licensing boards for exact requirements for dentallicense renewal.2019 Statistics on Worldwide OccurrenceCiting the Oral Cancer Foundation:Oral cancers are part of a group of cancers commonly referred to as head andneck cancers, and of all head and neck cancers, they comprise about 85% ofthat category. Brain cancer is a cancer category unto itself and is not included inthe head and neck cancer group.Historically the death rate associated with this cancer is particularly highnot because it is hard to discover or diagnose, but due to the cancer beingroutinely discovered late in its development. Today, (2019) that statement isstill true, as there is not a comprehensive program in the US to opportunisticallyscreen for the disease, and without that; late stage discovery is more common.Another obstacle to early discovery (and resulting better outcomes) is the adventof a virus, HPV16, contributing more to the incidence rate of oral cancers,particularly in the posterior part of the mouth (the oropharynx, the tonsils, thebase of tongue areas) which many times does not produce visible lesions or6
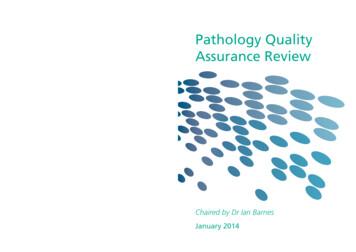
discolorations that have historically been the early warning signs of the diseaseprocess.Often oral cancer is only discovered when the cancer has metastasized toanother location, most likely the lymph nodes of the neck. Prognosis at this stageof discovery is significantly worse than when it is caught in a localized intra oralarea. Besides the metastasis, at these later stages, the primary tumor has hadtime to invade deep into local structures.Oral cancer is particularly dangerous because in its early stages it may not benoticed by the patient, as it can frequently prosper without producing pain orsymptoms they might readily recognize, and because it has a high risk ofproducing second, primary tumors. This means that patients who survive a firstencounter with the disease, have up to a 20 times higher risk of developing asecond cancer. This heightened risk factor can last for 5 to 10 years after the firstoccurrence. There are several types of oral cancers, but around 90% aresquamous cell carcinomas.Dental Professionals are often times the first line in defense, in simplyrecognizing abnormailities in a patient. Clearly, the earlier the detection, thehigher the rate of survival for patients.Oral Pathology Clinical Review1. FibromaFibroma Characteristics: “Irritation fibroma” “traumatic fibroma”BenignReactive vs. Neoplastico mature pyogenic granuloma?Buccal mucosa, labial mucosa, tongue, gingivalVariant on lingual surface canine area of mandibleo --Retrocuspid papillaPink7
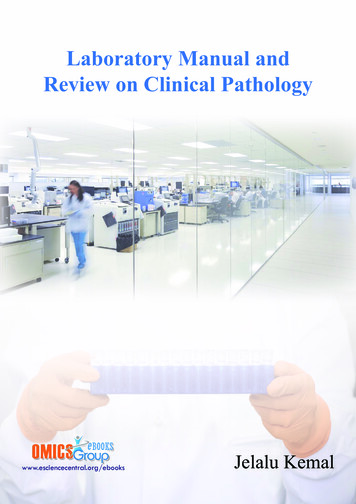
o /- pigmentationo /-hyperkeratosisSessile or pedunculatedFibroma of left labial commissure in a 59 y/o man (Medscape, 2013)Differential Diagnosis (DDX) FibromaNeurofibromaPyogenic granulomaPeripheral ossifying fibromaBenign mesenchymal neoplasmManagement / Prognosis ExcisionRemoval of causative agentsRecurrence rare2. Pyogenic GranulomaPyogenic Granuloma Characteristics Tumor-like growthNon-neoplastic, typically reactiveResponse to irritation, traumao --antecedent historyo --oral hygiene8
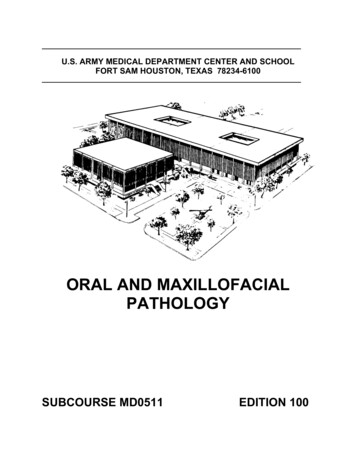
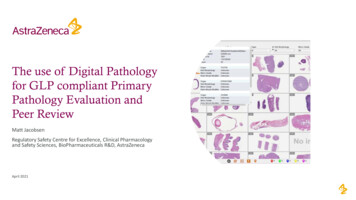
o --pregnancyGingiva, lips, tongue, buccal mucosaSmooth or lobulatedPink, red, purpleUlcerationVascularo --bleedingDifferential Diagnosis (DDX) Pyogenic granulomaPeriferal ossifying fibromaPeripheral giant cell granulomaLobular capillary hemangiomaEpulis granulomatosaPeripheral odontogenic neoplasmPyogenic Granuloma HistologyTypical appearance of a pyogenic granuloma involving the buccal gingiva of teeth numbers 20 and 21.Note the extreme vascularity. (Medscape, 2013)Diagnostic Aids RadiographPeriodontal probingVitality testingManagement / Prognosis Excision9
Excision to periosteum (gingival lesions)Removal of irritative sourcesRecurrence possible (inform patient)Pregnancy: defer until delivery if possible (recurrence common)3. Peripheral Ossifying FibromaPeripheral Ossifying Fibroma Characteristics Common gingival growthReactiveMaturing pyogenic granuloma (?)Sessile or peduncutlatedRed to pinkUlcerationMineralizationo --bone, cementum, dystrophic calcificationso --osteoid to mature lamellar boneDifferential Diagnosis Pyogenic granulomaPeripheral ossifying fibromaPeripheral giant cell granulomaLobular capillary hemangiomaPeripheral odontogenic fibroma10
Ossyfiying Fibroma / Wikipedia 2013Management / Prognosis ExcisionExcision to periosteum (gingival lesions)Removal of irritative sourcesRecurrence 8-16% (inform patient)4. PERIPHERAL GIANT CELL GRANULOMAPeripheral Giant Cell Granuloma Characteristics aka ‘peripheral giant cell eupulis’ReactiveGingiva, edentulous ridgeRed to re-blue ‘dusky’ massSimilar in appearance to pyogenic granulomaCupping resporption of underlying boneMulti-nucleated giant cells11
MitosesHemorrhageo --hemosiderinUlcerationDDX Pyogenic granulomaPeripheral giant cell granulomaCentral giant cell granulomao hyperparathyroidismo renal osteodystrophyo cherubismManagement and Prognosis ExcisionExcision to periosteum (gingival lesions)Removal of irritative sourcesRecurrence 10% (inform patient)Consider ruling out:o Central giant cell granulomao hyperparathyroidism5. Gingival OvergrowthAssociations Medicationso Calcium channel blockers (i.e. Nifedipine, Amlodipine)o Dilantino Cyclosporineo CyclophosphamideHereditary fibromatosesHyperplastic gingivitis12
o Also consider plasma cell gingivitis (cinnamon)Leukemic infiltrateManagement Alter medication if possibleRemove causative agentsRemove and avoid irritants (cinnamon)Genetic counselingManagement of malignancy (leukemia)6. Gingival CystGingival Cyst Characteristics DevelopmentalUsually mandibular anterior / biscuspidUsually facial gingivaPainless, dome-like swelling Lateral periodontal cystEpithelial inclusion cystDDXManagement and Prognosis ExcisionRecurrence rare13
7. Benign Migratory GlossitisBenign Migratory Glossitis Characteristics aka “geographic tongue”, erythema migransGreater incidence in femalesUnknown pathogenesiso may be associated with psoriaisisWell demarcated zones of erythemaAtrophy of filiform papillaeYellow-white serpentine borderPatient describes healing, then migrationFissured tongue Benign migratory Glossitis / erythema migransBurning tongue / burning mouthNutritional deficienciesRadiation – chemotherapy stomatitisDDXManagement and prognosis No treatment generally requiredPatient reassuranceAvoidance of irritating agentsTopical steroidsFluocinonide (Lidex) 0.05% gel, 30 gm tube, applied 2x/day if symptomatic14
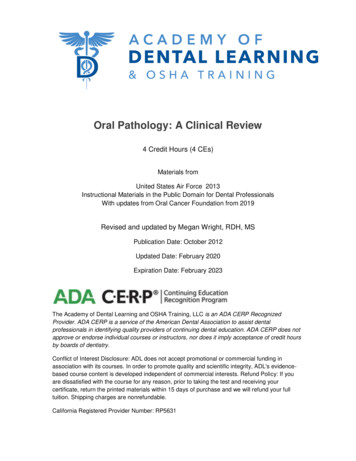
8. (Pseudomembranous) CandidiasisCytologic smear with fungal hyphaePseudomembranous Candidiasis Characteristics Considerationso oral inhaled steroidso systemic antibioticso immune suppressionDiabetes mellitusCytology / histologyInfectiouso candida specieso normal oral florao Cytologic smear using periodic acid Schiff (PAS)o candidal hyphaeForms Pseudomembranouso rubs off, leaving erythematous baseErythematouso red, burning sensationMedian rhomboid Glossitiso midline tongue, red, papillary atrophyAngular cheilitiso denture wearers, reduced VDAHyperplastico white, corrugated, does not rub offOthers15
DDX Varies according to typeFrictional irritation / hyperkeratosisSquamous cell carcinomaMateria alba **ck thisAnti-fungal StrategiesSystemic Nizoral (ketoconazole 200mg) 200-400mg/ dayo metabolized in liver, take with food, better absorbtion with acidic pHDiflucan (fluconazole 100mg/200mg) 100-200 mg/ dayo metabolized in kidney, food electiveTopical Mycelex (clotrimazole 10 mg), dissolve 1 troche 5x/dayMycostatin (nystatin)o suspension, swish and swallow500,000 U, 3 tsp/dayo vaginal troche, dissolves100,000 U, 3-5x/dayo Mycolog cream for angular cheilitisMycostatin Powder100,000U/gm, for dentureso Sporanox (itraconazole 10mg/ mL)10mL 2x/dayo Fungizone (amphotericin 100mg/ mL) 1 mL 4x/dayo Oravig (myconazole 50mg tablet)1x/day 14 days9. Apthous UlcerTypes Pathogenesis uncertaino T-cell mediatedo Immunodysregulation16
VariantsMinorooooNon keratinized mucosaSmall (3-10mm) fibrinopurulent membrane1-5 lesionsFewest recurrencesMajorooooLarger (1-3cm)Longest durationLabial, soft palate, tonsillar, oropharyngealScarringHerpetiformooooMultiple lesions (up to 100)1-3mmLesions coalesceRecurrences closely spacedCorticosteroids for Apthous UlcersSystemic Prednisone Tapering Dose:o 25mg / day x 15 dayso 12.5 mg / day x 15 dayso 6.25 mg / day x 15 dayso 6.25 mg / every other dayMedrol DosePak as directedTopical Lidex (fluocinonide 0.05%) Apply 3x / dailyTriamcinolone 0.01% susp Rinse 1 tsp 4 x / day, hold 3 mins, expectorate,NPO x 30 minsKenalog in Orabase Apply 3x / day17
10. HERPETIC STOMATISHerpes Simplex CharacteristicsHuman herpesviruses #1-8HSV1, HSV2, V2V, EBV, CMV, HHV-6/7, HHV-8HSV1 spread by salivaPrimary Infection / Primary herpetic gingivostomatis HSV-1Age range 6 mo – 5 yearLymphadenopathy, chills/ fever, nausea, vomiting, anorexia, irritability, orallesions, pharyngotonsillitisVesicles which ruptureGingival edema, erythema, enlargementSelf-innoculationContagious (hand hygiene)Secondary Infection Vermillion border / skin of lipsHerpes labalisProdromeVesicles which rupture and crustHerpetic whitlowLatencyAntivirals for Herpetic LesionsTopical Zovirax (acyclovir 5% ointment) Apply q3hr x 7 daysDenavir (penciclovir 1%) Apply q2hr x 4 days18
Other agents: Abreva (docosanol 10% cream) Apply 5x / day until resolutionDyclonine (0.5-1.0%) Apply prnSystemic Zovirax (acyclovir 200/400/800mg)Valtrex (valacyclovir 500mg)Famvir (famciclovir 125/250/500mg)11. Herpes Zoster (Shingles)Herpes Zoster Characteristics VZV (HHV-3)Latency in sensory nerves (CN-V)3 phases:1.2.a.b.c.d.e.3.Prodome (pain, itching, burning)Acute:Exanthem / rash along dermatomesVesiclesScarring, pigmentary changesOcular involvementFacial paralysis / auditory loss (RAMSAY HUNT)Chronic (post-herpetic neuralgia)19
Antivirals for Herpes ZosterSystemic FamciclovirValacyclovirAcyclovirPrednisoneTopical Zostrix (capsaisin)Lidocaine patch12. Lichen PlanusLichen Planus Characteristics Dermatologic diseaseVariety of causes:o T-cell mediatedo medication inducedo foreign bodyo stress / anxietyFemale predominanceSkin lesionso purple, pruritic, polygonalo lace-like striations (Wickham’s striate)o dysplastic nailsOral lesionso reticular formo erosive form20
HyperkeratosisAcanthosis (epithelial thickening)“Sawtooth” rete ridgesDegeneration of basal layersBand-like lymphocytic infiltrateDDX Lichen planusLichenoid drug / amalgam reactionGraft versus host diseaseOral mucosal cinnamon reactionManagement and Prognosis Reticular form usually requires no treatmentErosive forms use topical corticosteroido --Fluocinonide (Lidex)o --Clobetasol (temovate)o --Steroids may be compounded with OraBase or methylcellulose13. Pemphigus VulgarisPemphigus Vulgaris Characteristics Blistering diseaseAutoimmune reactiono desmosomesIntra-epithelial splitOther etiologieso medication inducedo paraneoplastic pemphiguso familial forms (Hailey-Hailey)Often manifest first intraorallyo precedes skin lesions up to 1 yr21
Soreness, erosions, ulcerationso desquamative gingivitisVesicles, bullae rupture quicklyNikolsky signo rubbing / pressure to mucosa induces blistersPeri-lesional tissue importantSeparation between cellso intraepithelial cleftingAcantholysis (lysis between the cells)o desmosomal attachments lostManagement and Prognosis Before treatment, cases were routinely fatalWith treatment, cases are less commonly fatalUsually systemic corticosteroids and other immune suppressive agentsrequiredManage in consultation with physicianPrednisone high initial dose (40-80mg daily) tapered over several weeks oncepatient responds.14. PemphigoidPemphigoid Characteristics(benign mucous membrane pemphigoid, cictricial pemphigoid) Most common auto-immune blistering disorderAutoantibodies vs. basement membraneUsually older patients (60-80 y/o)PruritisMultiple tense skin bullaeo rupture / heal w/o scarring22
Oral uncomono bullaeo shallow ulcerationsOcular involvemento symblepharon (adnesions)o cicatrix (scarring)o blindnessPeri-lesional tissue importantSeparation at basement membraneo subepithelial cleftingAcute / chronic inflammationManagement and Prognosis Refer to opthamalogist (important!)For oral mucosal lesions, start with topical steroidsMedications for Oral Mucosal DiseasesSystemic Prednisone 40-80 mg / dayPrednisone 40 mg / 30 mg (am/pm)Dapsone 50-300 mg/ dayDoxycycline 20 mg 2x / dayNiacinamide 0.5-2.0 mg daily (w/TCNs)Topical LidexTemovateUltravateDexamethasoneTriamcinolone23
15. Benign Mixed Turmor (pleomorphic adenoma)Benign Mixed Turmor (pleomorphic adenoma) Characteristics Most common salivary neoplasmParotid gland most common siteUpper lip, buccal mucosa, posterior palatePainless, slow growing massYoung to middle ageMore females than maleo --most salivary neoplasms show female predilectionCircimscribed to encapsulated3 major elements:1.Glandular epithelium (ducts)2.Myoepithelial cells3.hyalinizationOther elementso --keratinizing squamous cellso --mucous producing cellso --chondromyxoid (loose cartilaginous) backgroundDDX Pleomorphic adenomao other benign salivary neoplasmsMalignant salivary neoplasmso mucoepidermoid carcinomaLymphomaManagement and Prognosis ExcisionFor superficial parotid: superficial parotidectomyFor deep parotid or other gland: excision of entire gland sparing facial nerveCure rate 95%24
Recurrence possible, especially more myxoid / genetainous tumors (mayresult in tumor seeding during surgery)Carcinoma – mixed tumor possible16. Mucoepdermoid CarcinomaMucoepdermoid Carcinoma Characteristics Most common salivary malignancyConsidered a low grade malignancyParotid, palateLower lip, floor of mouth, tongue, retromolar padMassPainFacial palsyAsymptomatic swellingo fluctuanceo blue / red color (clinically mistaken for mucocele)Cystic spacesMucous-producing cellsSquamous elementsMay see keratinizationDDX Mucoepidermoid carcinomaSquamous cell carcinomaMucoceleSalivary duct cyst25
Management and Prognosis Determined by histologic grade and tumor stageSubtotal / total parotidectomy /- facial nerve sparingTotal excision of other glands with margin of normal tissue for minor glandsRadical neck dissection for invasive / high grade tumorsPost-operative radiation therapy for high-grade, invasive, or incompletely /non-excisable tumors90-98% cure for low grade tumors; 30-54% for high grade tumors17. Mucocele / RanulaMucocele / Ranula ( Mucocele on floor of mouth) Characteristics Mucous retentiono sometimes called ‘salivary duct cyst’Mucous extravasationo mucous escapes from ruptured ductDome shaped mucosal swellingFlutuant to firmRecurrence / association with eatingSialoliths / sialolithiasis (salivary stones)Spilled mucinGranulation tissueInflammation, foamy macrophagesChronic inflammation, fibrosisSialoadenitis (inflamed salivary glands)DDX MucoceleSalivary duct cystDermoid cystManagement and Prognosis Some mucoceles / ranulas rupture and self-healExcision usually required26
Remove adjacent glands (total sublingual or submandibular) to minimizerecurrencePrognosis excellent, other than recurrence18. Dermoid CystDermoid Cyst Characteristics DevelopmentalBenign cystic form or teratomaCommonly midline floor of mouthHistologyo squamous cell epitheliumo keratino adnexal (skin) structures in the wall: sebaceous, hair follicles, sweatglandsHistologic variation:o Epidermoid (1 germ layer)o Dermoid (2 germ layers)o Teratoma (3 germ layers)DDX Dermoid cystThyroglossal duct cystManagement and Prognosis ExcisionIntraoral approach if above mylohyoidExtraoral approach if below mylohyoidRecurrence uncommon27
19. Labial Melanotic MaculeLabial Melanotic Macule Characteristics BenignFlat brown mucosal discolorationIncreased melanin depositionIncreased melanocytesNot related to sun exposureSolitary, well-demarcatedTan to dark brown (blue, black)Non-enlargingDDX Melanotic maculeAmalgam tattooRule out the following features of melanoma: A B C D E:o A Asymmetryo B Borders irregularo C Color variationo D Diameter 6mmo E EvolutoionManagement and Prognosis Benign lesionBiopsy to rule out melanomaOften no further treatment required unless cosmetic28
20. Racial PigmentationRacial Pigmentation / Management and Prognosis No treatment required21. Minocycline StainingMinocycline Staining Characteristics / DDX Medication-induced pigmentationo anti-malarials (cloroquinine et al.)o antibiotics (tetracyclines, et al.)o tranquilizers (chlorpromazine)Racial pigmentationAddison’s disease29
22. Medication Induced PigmentationManagement and Prognosis No treatment requiredRemoval or alteration of medication may result in long term partial orcomplete resolution of pigmentConsult physician before considering alteration of mediation23. Amelogenesis ImperfectaAmelogenesis Imperfecta Characteristics Defect in enamel developmentComplex multiple forms:o hypoplastico hypocalcificationo hypomaturationo association with taurodontismComplete genotypic and phenotypic profileComplex classification30
Management and Prognosis Treatment focused on dental rehabilitationCaries controlManagement of loss of vertical dimensionFixed or removable dental prosthesis24. Opalescent TeethOpalescent Teeth Characteristics Rule out dentinogenesis imperfecta Rule out osteogenesis imperfectaDentinogenesis Imperfecta Defect in dentin and pulp developmentMultiple formso dentinogenesis imperfecto dentin dysplasiao opalescent teetho pulp malformationso root malformations31
Dentinogenesis imperfectaManagement and Prognosis Treatment focused on dental rehabilitationCaries controlTeeth are poor candidates for fixed prostheses (poor dentin characteristics)Removable / complete dental prostheses often requiredPulpal pathology common, endodontic therapy is challenging (pulp canalalteration or obliteration)25. Buccal Bifurcation CystBuccal Bifurcation Cyst (Inflammatory Buccal Cyst) Characteristics Inflammatory odontogenic cystLocations:o buccal aspect, mandibular first molaro distal buccal, third molars (paradental cyst)Associations:o cervical enamel extensionso eruption-associated inflammationRadiographic:o unilocular radiolucencyo buccal bifurcation and rootso occlusal radiograph: tipping of root apices toward lingual cortex32
DDX Buccal bifurcation cystInflammatory cyst (periodontal, endodontic)Other odontogenic cyst or tumorManagement and Prognosis Debridement – treat as a periodontal pathologyRemoval of cervical enamel projections and enamel pearls / beware of pulphornsExtraction usually not necessary26. Dentigerous (Follicular) CystDentigerous (Follicular) Cyst Characteristics Developmentalo most common developmental odontogenic cystAssociated with follicle / crown of developing tootho usually unerupted third molars, caninesRadiographico unilocular radiolucencyo crown of developing tootho well defined sclerotic borderDDX Dentigerous cystGlandular odontogenic cystameloblastomaOdontogenic keratocystManagement and Prognosis Careful cyst enucleation with extraction of toothSubmit entire cyst for evaluation33
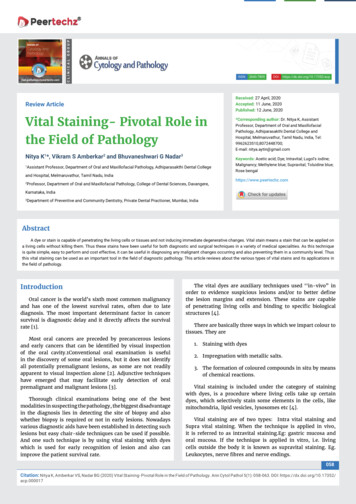
Tooth may be left if eruption anticipatedMarsupialization / decompression of large cysts may be consideredRecurrence rare with adequate enucleationMalignant transformation and development of odontogenic tumors are rare27. AmeloblastomaAmeloblastoma Characteristics Most common odontogenic tumorOdontogenic epithelial originBenign but aggressive3 variantsconventional solid / multi-cystic (most common type)unicystic3. peripheral / extraosseousMandible, usually molar-ramusPainless swelling and expansionRadiographic--multiocular (or uniocular)--“soap bubble” or “honeycomb” appearance on radiograph--associated with unerupted toothAmeloblastoma / Mayo ClinicHistology (follicular or variant)34
Islands of odontogenic epitheliumMature fibrous stromaTall columnar cellsPalisading (nuclei line up)Reverse polarity (nuclei away from basement membrane)Stellate reticulum (loose cellular architecture in the center of the nests /islands of epithelium.DDX AmeloblastomaDentigerous cystOdontogenic keratocystAmeloblastic fibroma / fibro-odontoma (child)Central giant cell granulomaManagement and Prognosis Wide excision usually recommended:1-1.5 cm marginRecurrence Enucleation: 50-90% recurrenceExcision:15%28. Odontogenic Keratocyst (Odontogenic Tumor)35
Odontogenic Keratocyst Characteristics Posterior body / ramus of mandibleRadiology well defined uni / multilocular radiolucencydefined bordersunerupted tooth (25-40%)Histology Clear/ cheesy fluid within cyst lumenEpithelium 6-8 cell thicknessFlat epithelium, lack rete ridgesWavy parakeratosisPalisaded basal layerInflammation may mask featuresDDX (often based on location) Dentigerous cyst (with unerupted tooth)Radicular cyst (at root apex)Residual cyst (in site of extracted tooth)Lateral periodontal cyst (along side of root)Nasopalatine duct cyst (mid-line, anterior palate)Glandular odontogenic cyst (often in anterior mandible)Odontogenic keratocyst (any location)Ameloblast
Oral Pathology Clinical Review 7 1. Fibroma 7 2. Pyogenic Granuloma 8 3. Peripheral Ossifying Fibroma 10 4. Peripheral Giant Cell Granuloma 11 5. Gingival Overgrowth 12 6. Gingival Cyst 13 7. Benign Migratory Glossitis 14 8. (Pseudomembranous) Candidiasis 15 9. Apthous Ulcer 16 10.