Transcription
CLASSIFICATIONOF DIABETESMELLITUS2019
Classification of diabetes mellitusISBN 978-92-4-151570-2 World Health Organization 2019Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGOlicence (CC BY-NC-SA 3.0 IGO; igo).Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided thework is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorsesany specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then youmust license your work under the same or equivalent Creative Commons licence. If you create a translation of this work,you should add the following disclaimer along with the suggested citation: “This translation was not created by the WorldHealth Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English editionshall be the binding and authentic edition”.Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of theWorld Intellectual Property Organization.Suggested citation. Classification of diabetes mellitus. Geneva: World Health Organization; 2019. Licence: CC BY-NC-SA 3.0 IGO.Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests forcommercial use and queries on rights and licensing, see http://www.who.int/about/licensing.Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figuresor images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission fromthe copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work restssolely with the user.General disclaimers. The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or areaor of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps representapproximate border lines for which there may not yet be full agreement.The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommendedby WHO in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names ofproprietary products are distinguished by initial capital letters.All reasonable precautions have been taken by WHO to verify the information contained in this publication. However, the publishedmaterial is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretationand use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.Design and layout by Hélène Dufays.Photo credits:Cover: WHO/Tania HabjouqaPages 5, 37: WHO/Eduardo MartinoPages 7, 28: WHO/Atul LokePage 12, 17: WHO/Frederik Naumann
Classification of diabetes mellitusTable of contentsAcknowledgements. 2Executive summary. 3Introduction . 51. Diabetes: Definition and diagnosis. 61.1 Epidemiology and global burden of diabetes. 61.2 Aetio-pathology of diabetes .72. Classification systems for diabetes. 82.1 Purpose of a classification system for diabetes .82.2 Previous WHO classifications of diabetes . 92.3 Recent calls to update the WHO classification of diabetes .112.4 WHO classification of diabetes 2019.112.4.1 Type 1 diabetes.132.4.2 Type 2 diabetes.142.4.3 Hybrid forms of diabetes.152.4.4 Other specific types of diabetes.182.4.5. Unclassified diabetes.232.4.6. Hyperglycaemia first detected during pregnancy .233. Assigning diabetes type in clinical settings.243.1 Age at diagnosis as a guide to subtyping diabetes.243.1.1. Age 6 months.243.1.2. Age 6 months to 10 years.253.1.3. Age 10 to 25 years.253.1.4. Age 25 to 50 years.263.1.5. Age 50 years.263.2 Differential diagnosis of individuals presenting with ketosis or ketoacidosis.264. Future classification systems . 27References. 291
AcknowledgementsWHO gratefully acknowledges the technical input and expert advice provided by the followingexternal experts.Amanda Adler, Addenbrooke’s Hospital, Cambridge, UKPeter Bennett, Phoenix Epidemiology & Clinical Research Branch, National Institute of Diabetes andDigestive and Kidney Diseases, National Institutes of Health, Phoenix, USAStephen Colagiuri (Chair), Boden Institute, University of Sydney, AustraliaEdward Gregg, Centers for Disease Control and Prevention, Atlanta, USAKM Venkat Narayan, the Rollins School of Public Health, Emory University, Atlanta, USAMaria Inês Schmidt, University of Rio Grande do Sul, Porto Alegre, BrazilEugene Sobngwi, Faculté de Medecine et des Sciences Biomedicales et Centre de Biotechnologie,Université de Yaounde 1, CameroonNaoko Tajima, Jikei University School of Medicine, Tokyo, JapanNikhil Tandon, All India Institute of Medical Sciences, New Delhi, IndiaNigel Unwin, Chronic Disease Research Centre, The University of the West Indies, Bridgetown, Barbados,and MRC Epidemiology Unit, University of Cambridge, UKSarah Wild, University of Edinburgh, UKJohn Yudkin, University College London, UKThe suggestions and contributions of the following peer reviewers are gratefully acknowledged:Naomi Levitt, Diabetic Medicine and Endocrinology, Department of Medicine at Groote Schuur Hospitaland University of Cape Town, South AfricaViswanathan Mohan, Dr Mohan’s Diabetes Specialities Centre, Chennai, IndiaSarah Montgomery, Primary Care International, Oxford, UKMoffat J Nyirenda, Medical Research Council/Uganda Virus Research Institute/London School ofHygiene and Tropical Medicine, Uganda Research Unit, Entebbe, UgandaJaakko Tuomilehto, Dasman Diabetes Institute, KuwaitSpecial thanks to Saskia Den Boon (consultant) and Samantha Hocking (Boden Institute, Universityof Sydney, Australia) for the preparation of background documents.WHO expresses special appreciation to US Centers for Disease Control and Prevention for financialsupport through grant GH14-1420.2
Classification of diabetes mellitusExecutive summaryThis document updates the 1999 World Health Organization (WHO) classification of diabetes. It prioritizesclinical care and guides health professionals in choosing appropriate treatments at the time of diabetesdiagnosis, and provides practical guidance to clinicians in assigning a type of diabetes to individualsat the time of diagnosis. It is a compromise between clinical and aetiological classification becausethere remain gaps in knowledge of the aetiology and pathophysiology of diabetes.While acknowledging the progress that is being made towards a more precise categorization of diabetessubtypes, the aim of this document is to recommend a classification that is feasible to implement indifferent settings throughout the world. The revised classification is presented in Table 1.Unlike the previous classification, this classification does not recognize subtypes of type 1 diabetesand type 2 diabetes and includes new types of diabetes (“hybrid types of diabetes” and “unclassifieddiabetes”).3
Table 1 : Types of diabetesType of diabetesBrief descriptionChange from previous classificationType 1 diabetesβ-cell destruction (mostly immunemediated) and absolute insulindeficiency; onset most common inchildhood and early adulthoodType 1 sub-classes removedType 2 diabetesMost common type, various degreesof β-cell dysfunction and insulinresistance; commonly associatedwith overweight and obesityType 2 sub-classes removedHybrid forms of diabetesNew type of diabetesSlowly evolving, immunemediated diabetes of adultsSimilar to slowly evolving type1 in adults but more often hasfeatures of the metabolic syndrome,a single GAD autoantibody andretains greater β-cell functionNomenclature changed – previouslyreferred to as latent autoimmunediabetes of adults (LADA)Ketosis-prone type 2 diabetesPresents with ketosis and insulin deficiencybut later does not require insulin; commonepisodes of ketosis, not immune-mediatedNo changeOther specific typesMonogenic diabetes- Monogenic defects of β-cell function- Monogenic defects in insulin actionCaused by specific gene mutations, hasseveral clinical manifestations requiringdifferent treatment, some occurring in theneonatal period, others by early adulthoodCaused by specific gene mutations;has features of severe insulinresistance without obesity; diabetesdevelops when β-cells do notcompensate for insulin resistanceUpdated nomenclature forspecific genetic defectsDiseases of the exocrine pancreasVarious conditions that affect thepancreas can result in hyperglycaemia(trauma, tumor, inflammation, etc.)No changeEndocrine disordersOccurs in diseases with excess secretionof hormones that are insulin antagonistsNo changeDrug- or chemical-inducedSome medicines and chemicalsimpair insulin secretion or action,some can destroy β-cellsNo changeInfection-related diabetesSome viruses have been associatedwith direct β-cell destructionNo changeUncommon specific forms ofimmune-mediated diabetesAssociated with rare immunemediated diseasesNo changeOther genetic syndromes sometimesassociated with diabetesMany genetic disorders and chromosomalabnormalities increase the risk of diabetesNo changeUnclassified diabetesUsed to describe diabetes that does notclearly fit into other categories. Thiscategory should be used temporarily whenthere is not a clear diagnostic categoryespecially close to the time of diagnosisNew types of diabetesHyperglycaemia first detected during pregnancyDiabetes mellitus in pregnancyType 1 or type 2 diabetes firstdiagnosed during pregnancyNo changeGestational diabetes mellitusHyperglycaemia below diagnosticthresholds for diabetes in pregnancyDefined by 2013 diagnostic criteriaDiagnostic criteria for diabetes: fasting plasma glucose 7.0 mmol/L or 2-hour post-load plasma glucose 11.1 mmol/L orHba1c 48 mmol/molDiagnostic criteria for gestational diabetes: fasting plasma glucose 5.1–6.9 mmol/L or 1-hour post-load plasma glucose 10.0 mmol/Lor 2-hour post-load plasma glucose 8.5–11.0 mmol/L4
Classification of diabetes mellitusIntroductionSince 1965 the World Health Organization has periodically updated and published guidance on how toclassify diabetes mellitus (hereafter referred to as “diabetes”) (1). This document provides an updateon the guidance last published in 1999 (2).Diabetes comprises many disorders characterized by hyperglycaemia. According to the currentclassification there are two major types: type 1 diabetes (T1DM) and type 2 diabetes (T2DM).The distinction between the two types has historically been based on age at onset, degree of loss of β cellfunction, degree of insulin resistance, presence of diabetes-associated autoantibodies, and requirementfor insulin treatment for survival (3). However, none of these characteristics unequivocally distinguishesone type of diabetes from the other, nor accounts for the entire spectrum of diabetes phenotypes.There are several reasons for revisiting the diabetes classification. Firstly, the phenotypes of T1DMand T2DM are becoming less distinctive with an increasing prevalence of obesity at a young age,recognition of the relatively high proportion of incident cases of T1DM in adulthood and the occurrenceof T2DM in young people. Secondly, developments in molecular genetics have allowed clinicians toidentify growing numbers of subtypes of diabetes, with important implications for choice of treatmentin some cases. In addition, increasing knowledge of pathophysiology has resulted in a trend towardsdeveloping personalized therapies and precision medicine (3). Unlike the previous classification,this classification does not recognize subtypes of T1DM and T2DM, includes new types of diabetes(“hybrid types of diabetes” and “unclassified diabetes”), and provides practical guidance to cliniciansfor assigning a type of diabetes to individuals at the time of diagnosis.5
1. Diabetes: Definition and diagnosisThe term diabetes describes a group of metabolic disorders characterized and identified by the presenceof hyperglycaemia in the absence of treatment. The heterogeneous aetio-pathology includes defects ininsulin secretion, insulin action, or both, and disturbances of carbohydrate, fat and protein metabolism.The long-term specific effects of diabetes include retinopathy, nephropathy and neuropathy, amongother complications. People with diabetes are also at increased risk of other diseases including heart,peripheral arterial and cerebrovascular disease, obesity, cataracts, erectile dysfunction, and nonalcoholicfatty liver disease. They are also at increased risk of some infectious diseases, such as tuberculosis.Diabetes may present with characteristic symptoms such as thirst, polyuria, blurring of vision,and weight loss. Genital yeast infections frequently occur. The most severe clinical manifestationsare ketoacidosis or a non-ketotic hyperosmolar state that may lead to dehydration, coma and, in theabsence of effective treatment, death. However, in T2DM symptoms are often not severe, or may beabsent, owing to the slow pace at which the hyperglycaemia is worsening. As a result, in the absenceof biochemical testing, hyperglycaemia sufficient to cause pathological and functional changes maybe present for a long time before a diagnosis is made, resulting in the presence of complications atdiagnosis. It is estimated that a significant percentage of cases of diabetes (30–80%, depending onthe country) are undiagnosed (4).Four diagnostic tests for diabetes are currently recommended, including measurement of fasting plasmaglucose; 2-hour (2-h) post-load plasma glucose after a 75 g oral glucose tolerance test (OGTT); HbA1c;and a random blood glucose in the presence of signs and symptoms of diabetes. People with fastingplasma glucose values of 7.0 mmol/L (126 mg/dl), 2-h post-load plasma glucose 11.1 mmol/L(200 mg/dl) (5), HbA1c 6.5% (48 mmol/mol); or a random blood glucose 11.1 mmol/L (200 mg/dl) in the presence of signs and symptoms are considered to have diabetes (6). If elevated values aredetected in asymptomatic people, repeat testing, preferably with the same test, is recommended assoon as practicable on a subsequent day to confirm the diagnosis (6).A diagnosis of diabetes has important implications for individuals, not only for their health, but alsobecause of the potential stigma that a diabetes diagnosis can bring may affect their employment,health and life insurance, driving status, social opportunities, and carry other cultural, ethical andhuman rights consequences.1.1 Epidemiology and global burden of diabetesDiabetes is found in every population in the world and in all regions, including rural parts of low- andmiddle-income countries. The number of people with diabetes is steadily rising, with WHO estimatingthere were 422 million adults with diabetes worldwide in 2014. The age-adjusted prevalence in adultsrose from 4.7% in 1980 to 8.5% in 2014, with the greatest rise in low- and middle-income countriescompared to high-income countries (7). In addition, the International Diabetes Federation (IDF) estimatesthat 1.1 million children and adolescents aged 14–19 years have T1DM (8). Without interventionsto halt the increase in diabetes, there will be at least 629 million people living with diabetes by 20456
Classification of diabetes mellitus(8). High blood glucose causes almost 4 million deaths each year (7), and the IDF estimates that theannual global health care spending on diabetes among adults was US 850 billion in 2017 (8).The effects of diabetes extend beyond the individual to affect their families and whole societies. It hasbroad socio-economic consequences and threatens national productivity and economies, especiallyin low- and middle-income countries where diabetes is often accompanied by other diseases.1.2 Aetio-pathology of diabetesIt is now generally agreed that the underlying characteristic common to all forms of diabetes is thedysfunction or destruction of pancreatic β-cells (9–12). Many mechanisms can lead to a decline infunction or the complete destruction of β-cells (these cells are not replaced, as the human pancreasseems incapable of renewing β-cells after the age of 30 years (13)). These mechanisms includegenetic predisposition and abnormalities, epigenetic processes, insulin resistance, auto-immunity,concurrent illnesses, inflammation, and environmental factors. Differentiating β-cell dysfunction anddecreased β-cell mass could have important implications for therapeutic approaches to maintainingor improving glucose tolerance (11). Understanding β-cell status can help define subtypes of diabetes,and guide treatment (12)7
2. Classification systems for diabetes2.1 Purpose of a classification system for diabetesHyperglycaemia is the defining common feature of all types of diabetes, but aetiology, underlyingpathogenic mechanisms, natural history and treatment for the different types of diabetes differ. Ideally,all types of diabetes would be defined by defining features that are specific and exclusive to that typeof diabetes (3). However, some types of diabetes are difficult to classify.Classification systems can broadly be used for three primary aims:»» Guide clinical care decisions»» Stimulate research into aetio-pathology»» Provide a basis for epidemiological studiesAny classification system should be able to help with all three of these key activities, but at presentthere are so many gaps in understanding the causes of diabetes that the current classification cannotfulfil this triple role.Clinical care decisionsSubtyping diabetes is important in clinical care for diagnosis, to guide treatment choices, and whenmaking treatment decisions for a person whose glycaemic control is unsatisfactory. An incorrecttreatment decision could risk a person developing diabetic ketoacidosis (DKA) or lead to unnecessaryinsulin therapy in the case of some forms of monogenic diabetes. The phenotype of both T1DM(overweight or obese) and T2DM (younger, normal weight) have changed over time and contributesto clinicians’ increasing difficulty classifying types of diabetes.Aetio-pathologyThe aetiology and pathogenesis of diabetes can be described simplistically as problems withinsulin sensitivity and insulin secretion, but the underlying specific defects are complex and not wellunderstood. While some specific defects have been identified (e.g. genetic abnormalities resulting ininsulin secretory problems), defining the mechanisms underlying common forms of diabetes remainschallenging as they are increasingly recognized to involve a complex interplay of genetic, epigenetic,proteomic and metabolomic processes. Identifying these abnormalities will improve our understandingof the underlying mechanisms of diabetes and its treatment, but at present, our limited knowledge ofthese complex abnormalities hinders the development of a practical and clinically useful classificationsystem for diabetes.This problem also currently applies to the field of pharmacogenomics. A systematic review commissionedby WHO has examined the association between specific genetic variants and response to bloodglucose lowering therapies (14). While it is well known in clinical practice that some people respondbetter than others to a specific blood glucose-lowering treatment, studies of genetic variants and drugresponse in a person with diabetes have to date demonstrated only small and inconsistent effects8
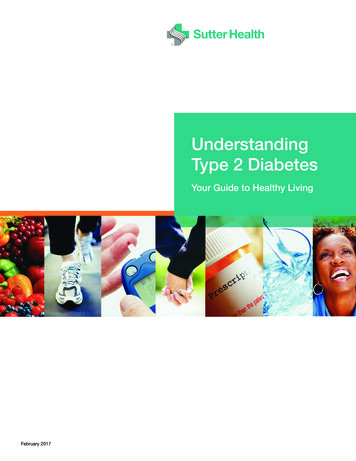
Classification of diabetes mellitusacross studies. While pharmacogenomics holds promise to more precisely target therapy for T2DM,it is not currently clinically helpful.Epidemiological studiesMost epidemiological studies report overall prevalence of diabetes without distinguishing betweensubtypes, despite the value of subtyping for such studies. Subtyping T1DM and T2DM in populationstudies is feasible using frequently available clinical information (15, 16). Some studies have reportedthe population prevalence of other forms of diabetes, e.g. monogenic diabetes (17, 18) and diabetesdue to pancreatic disease (19). Classification of diabetes type is particularly important for incidencestudies and studies on diabetes-related complications.2.2 Previous WHO classifications of diabetesDiabetes has been known about for many centuries. The 5th century physician Aretaeus first used theterm “diabetes” (meaning “a siphon” in Greek) to describe the disease as a “melting down of flesh andlimbs into urine”. Indian physicians during the 5th century BC described the sweet, honey-like taste ofurine in polyuric patients (madhu meha, meaning “honey urine”) that attracted ants and other insects,but the word “mellitus” (Latin for “honey”) was added in the 17th century. As early as the 5th centuryAD descriptions of diabetes mentioned two forms, one in older, fatter people and the other in thinnerpeople with short survival (20).WHO published its first classification system for diabetes in 1965 using four age of diagnosis categories:infantile or childhood (with onset between the ages of 0–14); young (with onset between the agesof 15–24 years); adult (with onset between the ages of 25–64 years); and elderly (with onset at theage of 65 years or older). In addition to classifying diabetes by age, WHO recognized other forms ofdiabetes: juvenile-type; brittle; insulin-resistant; gestational; pancreatic; endocrine and iatrogenic (1).WHO published its first widely accepted and globally adopted classification of diabetes in 1980 (21)and an updated version of this in 1985 (22). These classifications included two major classes ofdiabetes: insulin dependent diabetes mellitus (IDDM), or type 1; and non-insulin dependent diabetesmellitus (NIDDM), or type 2 (21). The 1985 report omitted the terms “type 1” and “type 2”, but retainedthe classes IDDM and NIDDM, and introduced a class of malnutrition-related diabetes mellitus(MRDM) (22). Both the 1980 and 1985 reports included two other classes of diabetes: “other types”and “gestational diabetes mellitus” (GDM). These were reflected in the International nomenclature ofdiseases (IND) in 1991, and the tenth revision of the International Classification of Diseases (ICD–10)in 1992. These reports represented a compromise between clinical and aetiological classificationand allowed clinicians to classify individual subjects even when the specific cause or aetiology wasunknown.In 1999 WHO recommended that the classification should encompass not only the different aetiologicaltypes of diabetes, but also the clinical stages of the disease (2) (see Figure 1). The clinical staging reflectsthat people with diabetes, regardless of type, can progress through several stages, from normoglycaemiato severe hyperglycaemia with ketosis. However, not everyone will go through all stages. Moreover,individuals with T2DM may move from stage to stage in either direction. People who have, or who9
are developing, diabetes can be categorized by stage according to clinical characteristics, in theabsence of information concerning the underlying aetiology. In 1999, WHO reintroduced the termstype 1 and type 2 diabetes and dropped MRDM because of lack of evidence to support its existenceas a distinct type.Figure 1 : Disorders of glycaemia: aetiological types and clinical stages(WHO, 1999)StagesNormoglycaemiaNormal glucosetoleranceTypesHyperglycaemiaImpaired glucoseregulationIGT and/or IFGDiabetes MellitusNot insulinrequiringInsulinrequiring forcontrolInsulin requiringfor survivalType 1 Autoimmune IdiopathicType 2* Predominantlyinsulinresistance PredominantlyinsulinsecretorydefectsOther specific types*Gestationaldiabetes**In rare instances patients in these categories (e.g. Vacor Toxicity, Type 1 presenting in pregnancy, etc.) may require insulin for survival.Source: reproduced from the World Health Organization’s 1999 classification (2).10
Classification of diabetes mellitus2.3 Recent calls to update the WHO classification of diabetesThere have been recent calls to review and update the classification system for diabetes. This isbecause many people with diabetes do not fit into any single category; there have been recent advancesin knowledge of pathophysiological pathways and emerging technologies to examine pathology andtreatments that act on specific pathways; and there is a trend towards individualized treatment.There is well-established acceptance of the overlap of diabetes subtypes, especially in relation toT1DM, T2DM and so-called latent autoimmune diabetes of adults (LADA) (3). Laboratory tests couldin some instances improve disease classification and potentially improve the efficacy of treatmentfor diabetes, but many of these tests are beyond the reach or affordability of most clinical settingsthroughout the world.A recent proposal suggested a classification system centred on the β-cell (10). Proponents for thismodel note that all forms of diabetes have abnormal pancreatic β–cell function and that individually orin concert, 11 distinct pathways contribute to β–cell stress, dysfunction, or loss. In this way treatmentscould be targeted to specific mediating pathways of hyperglycaemia in a given patient. This proposalexpands on an earlier model which described eight core defects of diabetes (23). While the β–cellcentric model is a conceptual framework to help optimize diabetes care and precision treatment, it ispredicated on additional diagnostic tests that are either not standardized or not routinely availablein most clinical settings, e.g. measurement of C-peptide, β-cell-specific autoantibodies, markers oflow-grade inflammation, measures of insulin resistance, and assays for β-cell mass.2.4 WHO classification of diabetes 2019Ideally a single classification system for diabetes would facilitate three primary purposes: clinical care,aetio-pathology and epidemiology. However, this is not possible with our current state of knowledgeand the resources available in most countries throughout the world.With this in mind, the Expert group considered it best to define a classification system that prioritizesclinical care and helps health professionals choose appropriate treatments, and whether or not tostart treatment with insulin, particularly at the time of diagnosis.The group considered that the prerequisites of a clinically based classification system include beinginternationally applicable and using easy and readily available clinical parameters and resources;being reliable and equitable; and feasible to implement.The only classification system which could currently go some way towards achieving this is onebased on clinical parameters to identify diabetes subtypes. Some countries and clinical or researchcentres can supplement this approach with specific additional investigations, but these are notuniversally available and a classification system which relied on these measures would have limitedglobal applicability.Clinically, genotyping is relevant to monogenic diabetes but not T1DM or T2DM which are polygenic(genome-wide association studies have identified over 100 associated genetic markers (9)). At this time,11
genotyping for diabetes subtyping is only relevant to patients in whom clinicians suspect monogenicdiabetes and may be useful in a research setting in relation to other types of diabetes.Autoantibodies against a variety of β-cell components including glutamic acid decarboxylase (GAD65),islet antigen-2 (IA-2), zinc transporter 8 (ZnT8) and insulin are commonly found in people with classicalT1DM but
Diabetes comprises many disorders characterized by hyperglycaemia. According to the current classification there are two major types: type 1 diabetes (T1DM) and type 2 diabetes (T2DM). The distincti