Transcription
9/13/2011CARDIOVASCULAR SYSTEMCODING MADE EASYTeresa Marshall, CCSJacqueline Woeppel, MBA, RHIA, CCSAAPC Regional ConferenceSeptember 9, 20112Cardiovascular Agenda Billing and Coding Policy Modifiers and Medical Necessity Nuts and Bolts PET Stress Tests Nuclear Stress Tests Echo Cardiac Catheterization Cardiac Intervention ICD-9-CM Update and Revisions ICD-10-CMPhoto :http://www.bmhvt.org/services/card ST.sh1
9/13/20113CV-Medical Legal NCD vs. LCD CAHABA Government Benefit Administrator https://www.cahabagba.com/part b/policies medical review/lcd active.htm National Correct Coding Initiative Coding Policy Manualfor Medicare Services. /www.bing.com/images4Medicare, Modifiers, and Medical Necessity Introduced to provide additional information Resource: CMS Claims Processing Manual (PUB 100-04) Chapter 1, section 60.1.3.1 and 60.4.2 Cahaba Government Benefit Administration https://www.cahabagba.com/part b/education and outreach/general billing info/modifers.htm#52
9/13/20115Medicare, Modifiers and Medical Necessity GA Modifier When to use the GA modifier? Item or service expected to be denied as not reasonable and necessary ABN--Waiver of liability on file Required to be reported on claim when Signed ABN on file or Patient’s refusal with witnessed documentation Is the patient responsible if the claim is denied? Beneficiary is NOT liable if ABN was not signed prior to the servicebeing rendered Beneficiary is responsible with ABN (i.e. other insurance)6Medicare, Modifiers and Medical Necessity Modifier GY When to use modifier? When you expect a denial Excluded or definition Obtain Medicare denial for secondary payor No ABN requirements What happens if you use GY modifier? Create an automatic denial Patient is liable for charges Personally or via other insurances If you do not use GY Modifier Claim Reviewed Beneficiary may be liable Excluded service or definition3
9/13/20117Medicare, Modifiers and Medical Necessity Modifier GZ When to use GZ modifier? Item or service does not meet Medicare policy standards for medicalnecessity and no ABN was obtained Expect a service to be denied Patient refused an ABN, but service provided What happens when GZ modifier is used? Claim will be reviewed If claim denied Patient generally not liable Modifier is voluntary Reduce risk8Other Insurance ProvidersCarrier ManualMedical PolicyDiagnosis/CPT4
9/13/20119Cardiovascular Test PET Stress Test Advanced stress test utilizing small amounts of ―tracer‖ injected intoblood stream Ischemia CAD Nuclear Stress Test Radioactive exercise stress test SizePumping bloodDamaged or dead muscleArteries (narrowed or blocked) Echocardiogram (ECHO) Sound waves creates a motion picture of the heart Size and shape of the heart How well the heart is working (i.e. contracting, blood flow)10PET Perfusion TestIndication: Multiple cardiac risk factors and cardiomyopathy.Technique: Perfusion PET images were acquired at rest. Low-dose noncontrasted CTtransmission images were acquired for attenuation correction. Following an IV infusion ofinsulin and dextrose. F-18-FDG was administered intravenously and PET imagesrepresentative of myocardial glucose metabolism were acquired. The fasting blood glucosewas 99 mg/dl. Rest dose of Rubidium-82 (mCi): 42.4 and Rest dose of F-18 FDG (mCi): 13.5.Findings: Quality of the study was good. Rest LVEF was 29%. Wall motion abnormalities:global hypokinesis with severe hypokinesis of the inferior wall. The PET perfusion imagesdemonstrate a large zone of moderately decreased activity along the inferior wall. The FDGimages demonstrate a matched severe metabolic defect concordant with the perfusion defectwith no significant mismatch.Impression: 1) The fixed perfusion abnormality involving the inferior wall is most consistentwith myocardial scarring. The matching FDG metabolic defect is confirmatory of myocardialscarring with no evidence of hibernating for chronically ischemic myocardium. 2) The globalleft ventricular systolic function is severely compromised with a left ventricular ejection fractionof 29% and marked LV dilatation. There is global hypokinesis and severe hypokinesis of theinferior wall. 3) There is no prior study available for comparison. 4) The low-dose,noncontrasted, limited field-of-view CT demonstrates cardiomegaly, aortic valve calcifications,mild coronary artery calcifications.5
9/13/201111PET Perfusion TestIndication: Multiple cardiac risk factors andcardiomyopathy. Technique:Perfusion PET imageswere acquired at rest. Low-dose noncontrasted CT transmission images were acquired for attenuationcorrection. Following an IV infusion of insulin and dextrose. F-18-FDG was administered intravenously andPET images representative of myocardialglucose metabolism were acquired.Thefasting blood glucose was 99 mg/dl. Rest dose of Rubidium-82 (mCi): 42.4 and Rest dose of F-18 FDG (mCi):13.5. Findings: Quality of the study was good. Rest LVEF was 29%. Wall motion abnormalities: globalhypokinesis with severe hypokinesis of the inferior wall. The PET perfusion images demonstrate a large zoneof moderately decreased activity along the inferior wall. The FDG images demonstrate a matched severemetabolic defect concordant with the perfusion defect with no significant mismatch.Impression: 1) The fixed perfusion abnormality involving the inferior wall is most consistent with myocardialscarring. The matching FDG metabolic defect is confirmatory ofmyocardial scarring with noevidence of hibernating for chronically ischemic myocardium. 2) The global left ventricular systolic function isseverely compromised with a left ventricularejection fraction of 29%and marked LV dilatation.There is global hypokinesis and severe hypokinesis of the inferior wall. 3) There is no prior study available forcardiomegaly,aortic valve calcifications, mild coronary artery calcifications. .comparison. 4) The low-dose, noncontrasted, limited field-of-view CT demonstratesCODE(S): (1) 425.4 (2) 424.1 (3) 414.00 (4) 429.3(1) 78491-26 (2) 78459-2612Nuclear Stress Test6
9/13/201113Nuclear Perfusion Study-- ExampleINDICATION: Chest pain.LEXISCAN PORTION: Patient underwent a Lexiscan nuclear perfusionstudy for suspected coronary artery disease. During the Lexiscaninfusion, the patient was given 27 mCi of technetium-99m sestamibi forvisualization of myocardium in standard different planes. Resting EKGshows normal sinus rhythm, has been changed to sinus tachycardiawithout ischemic EKG changes toward the end of the test. Restingheart rate is 80 beats per minute, has been changed to 108 beats perminute towards the end of the test. Resting blood pressure is 170/100,has been changed to 172/98 towards the end of the test. No significantmalignant arrhythmias noted.CONCLUSION: 1) Test was negative for chest pain. 2) Test wasnegative for ischemic EKG changes. 3) Good hemodynamic responsenoted. 4) Myocardial nuclear perfusion study documented in thepatient’s chart was negative for ischemia.14Nuclear Perfusion Study-- ExampleINDICATION: ChestpainDX CODE: 786.50LEXISCAN PORTION: Patient underwent a Lexiscan nuclear perfusion study forsuspected coronary artery disease. During the Lexiscan infusion, the patientwas given 27 mCi of technetium-99m sestamibi for visualization of myocardium instandard different planes. Resting EKG shows normal sinus rhythm, has beenchanged to sinus tachycardia without ischemic EKG changes toward the end of thetest. Resting heart rate is 80 beats per minute, has been changed to 108beats per minute towards the end of the test. Resting blood pressure is 170/100,has been changed to 172/98 towards the end of the test. No significant malignantarrhythmias noted.CONCLUSION: 1) Test was negative for chest pain. 2) Test was negative forischemic EKG changes. 3) Good hemodynamic response noted. 4) MyocardialNuclear Perfusion study documented in the patient’s chart was negative forischemia.CPT CODE(S): (1) 78452-26, (2) 93016 (3) 930187
9/13/201115Treadmill and Myocardial NuclearPerfusion Study--ExampleINDICATION: Chest PainFINDINGS: Patient underwent treadmill nuclear perfusion study forsuspected coronary artery disease. The patient exercised on thetreadmill according to standard Bruce protocol for 8 minutes 1 secondand achieved 9 METs. Resting EKG shows normal sinus rhythm, hasbeen changed to sinus tachycardia without ischemic EKG changes.The patient achieved 9 METS. Resting heart rate is 75 beats perminute, has been changed to 156 beats per minute, which is 89% ofmaximum predicted heart rate. Resting blood pressure is 126/78, hasbeen changed to 178/83 toward the end of the test. No significantmalignant arrhythmias noted.CONCLUSION: 1) Test was negative for chest pain. 2) Test wasnegative for ischemic EKG changes. 3) Good hemodynamic responsenoted. 4) Myocardial perfusion study documented in the patient chartas negative for ischemia.16Treadmill and Myocardial NuclearPerfusion Study--ExampleINDICATION: Chest PainCODE(S): 786.50FINDINGS: Patient underwent treadmill nuclear perfusion study for suspectedcoronary artery disease. The patient exercised on the treadmillaccording to standard Bruce protocol for 8 minutes 1 second and achieved 9 METs.Resting EKG shows normal sinus rhythm, has been changed to sinus tachycardiawithout ischemic EKG changes. The patient achieved 9 METS. Resting heartrate is 75 beats per minute, has been changed to 156 beats per minute, which is89% of maximum predicted heart rate. Resting blood pressure is126/78, has been changed to 178/83 toward the end of the test. No significantmalignant arrhythmias noted.CONCLUSION: 1) Test was negative for chest pain. 2) Test was negativefor ischemic EKG changes. 3) Good hemodynamic response noted. 4) Myocardialperfusion study documented in the patient chart as negative for ischemia.CPT CODE(S): 78452-26, 93016, 930188
9/13/201117Echocardiogram Reasons Heart failure Damage to heart valves Congenital heart defects Aorta aneurysm Blood Clots Types Transthoracic Stress Transesophageal chocardiogram.html, 201118Transesophageal Echocardiogram -ExamplesINDICATION: 66 year old man with head and neck cancer referred for mitral valveabnormality on TTE.CONCLUSIONS: 1) Normal LV size and function. LVEF.55%. 2) Myxomatous changesof mitral valve leaflets with mild mitral valve prolapse. No MV mass or vegetation. 3)Mild mitral regurgitation. 4) PFO by agitated saline contrastFINDINGS: The procedure and risk were explained to the patient who consented to thestudy. The patient tolerated the procedure well without any apparent complications.Pulse wave, continuous wave, and color Doppler used to assess Valvular function,pulmonary veins, and interatrial septum. TEE probe was placed by the Cardiologist.Patient received conscious sedation which was administered by anesthesia. The leftventricular chamber size is normal. The wall thickness is normal. Normal left ventricularsystolic function. LVEF 55%. No thrombosis is visualized within the left ventricle.Normal LA chamber size. The left atrial appendage velocity is normal. No LA appendagethrombus. RV chamber size and systolic function within normal limits. RA appearsnormal. PFO seen. PFO by agitated saline contrast. AV is trileaflet. Leaflets are thinwith normal excursion. No aortic stenosis or regurgitation. No aortic regurgitation.Myxomatous changes of mitral valve leaflets. There is prolapse of the anterior leaflet ofthe mitral valve. Mild mitral regurgitation. Tricuspid valve normal in structure andfunction. The pulmonic valve appears normal. No pulmonic regurgitation. Normalpericardium. Normal aorta. Main pulmonary artery normal. Pulmonary veins normal .9
9/13/201119Patent Foramen Ovale (PFO) Small hole located in theatrial septum that is usedduring fetal circulation. Normally the foramen ovalcloses at birth. If the atrial septum doesnot close properly, it iscalled the patent foramenovale. Why is this important tocoding?Photo enital/pfo.aspx20Transesophageal Echocardiogram -ExamplesINDICATION: 66 year old man with head and neck cancer referred for mitral valve abnormality onTTE.CONCLUSIONS: 1) Normal LV size and function. LVEF.55%. 2) Myxomatous changes of mitral valveleaflets with mild mitral valve prolapse. No MV mass or vegetation. 3) Mild mitral regurgitation. 4)PFO by agitated saline contrast.FINDINGS: The procedure and risk were explained to the patient who consented to the study. Thepatient tolerated the procedure well without any apparent complications. Pulse wave, continuouswave, and color Doppler used to assess valvular function, pulmonary veins, and interatrial septum.TEE probe was placed by the Cardiologist. Patient received conscious sedation which wasadministered by anesthesia. The left ventricular chamber size is normal. The wall thickness is normal.Normal left ventricular systolic function. LVEF 55%. No thrombosis is visualized within the leftventricle. Normal LA chamber size. The left atrial appendage velocity is normal. No LA appendagethrombus. RV chamber size and systolic function within normal limits. RA appears normal. PFO seen.PFO by agitated saline contrast. AV is trileaflet. Leaflets are thin with normal excursion. No aorticstenosis or regurgitation. No aortic regurgitation. Myxomatous changes of mitral valve leaflets. Thereis prolapse of the anterior leaflet of the mitral valve. Mild mitral regurgitation. Tricuspid valve normalin structure and function. The pulmonic valve appears normal. No pulmonic regurgitation. Normalpericardium. Normal aorta. Main pulmonary artery normal. Pulmonary veins normal.CODE(S): 1) 424.0 2) 745.5(1) 93315-26, (2) 93320-26, (3) 93325-26References: CPT Assistant, December 1997 page 5-610
9/13/201121Echocardiogram - What’s Missing?22Transthoracic Echocardiogram - ExampleINDICATIONS (REASON FOR STUDY): follow-uppericardial effusion, device ASD closure 3/31/2011.CONCLUSIONS: Since prior echo 4/1/11, this limited echodone to follow-up pericardial effusion shows that the fairlysmall pericardial effusion seen yesterday is now slightlysmaller. Today there is 1mm of pericardial fluid anteriorlyand about 2mm of fluid posteriorly.MEASURMENTS: (See next Slide)Photo: cs/holes/types.html, 201111
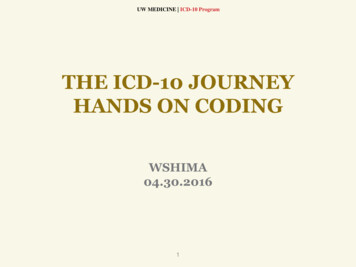
9/13/201123Transthoracic Echocardiogram – Example(continued)MeasurementsNameChamber measurementsRVIDd (2D)IVSd (2D)LVIDd (2D)LVIDs (2D)LVPWd (2D)ValueNormal Range4.4 cm0.9 cm4.1 cm2.8 cm0.9 cm(2.7-3.3)(0.6-1.1)(3.5-5.6)(2.1-3.7)(0.6-1.1)Ao Root Diam (2D)LA Diam (2D)2.6 cm4.1 cm(2.1-3.7)(1.9-4)LA Diam (2D) IndexTV/PV ValveTR Pk VelRAPRVSPMitral ValveMV Decal Time2.2 cm/m2(-2.3)3.34 m/sec3 mmHg47.62 mmHg195 msec24Transthoracic Echocardiogram - ExampleINDICATIONS (REASON FOR STUDY): follow-uppericardial effusion, device ASD closure 3/31/2011.CODE(S): 423.9CONCLUSIONS: Since prior echo 4/1/11, this limited echodone to follow-up pericardial effusion shows that the fairlysmall pericardial effusion seen yesterday is now slightlysmaller. Today there is 1mm of pericardial fluid anteriorlyand about 2mm of fluid posteriorly.CODE(S): 93308-26MEASURMENTS: (See previous Slide)12
9/13/201125Transthoracic Echocardiogram- ExamplesIndication: Unspecified Disease of PericardiumStudy Reason: Breast cancer, breast implants, h/o perimembranousventricular septal defect, s/p pericardiocentesis with 900 cc drained.Conclusions: Only a trivial amount of pericardial fluid is present. TheVSD was not assessed during this study. There is borderline significantrespiratory variation in the mitral valve inflow pattern of 25-30%- thismay be due to obesity, or suggest an element of constriction. Sinceprevious echo 4/31/10, the effusion has been drained.Findings: The study quality is fair. The left ventricular chamber size isnormal. Moderate concentric LVH. LVEF 55%. LA moderately dilated.RV size normal. RV wall thickness is normal. RV systolic functionnormal. RA size normal. The aortic valve leaflets are not wellvisualized. No aortic regurgitation. Mitral valve normal. No mitralregurgitation. Tricuspid valve leaflets normal. No TV regurgitation.Pulmonic valve not well seen. Trivial pericardial effusion. Normalaorta. Inferior vena cava very small, suggesting central hypovolemia.Measurements: (See next slide)26Transthoracic Echocardiogram- ExamplesMeasurementsNameValueChamber MeasurementsNormal RangeIVSd (2D)LVIDd (2D)LVIDs (2D)LVPWd (2D)Ao Root Diam (2D)LA Diam 1.9-4)1.8 cm4.4 cm4 cm1.3 cm3 cm5.2 cm13
9/13/201127Transthoracic Echocardiogram- ExamplesIndication: Unspecified Disease of PericardiumStudy Reason: Breast cancer, breast implants, h/o perimembranousventricular septal defect, s/p pericardiocentesis with 900 cc drained.CODE(S): 1) 423.9Conclusions: Only a trivial amount of pericardial fluid is present. TheVSD was not assessed during this study. There is borderline significantrespiratory variation in the mitral valve inflow pattern of 25-30%- this maybe due to obesity, or suggest an element of constriction. Since previousecho 4/31/10, the effusion has been drained.Findings: The study quality is fair. The left ventricular chamber size isnormal. Moderate concentric LVH. LVEF 55%. LA moderately dilated.RV size normal. RV wall thickness is normal. RV systolic function normal.RA size normal. The aortic valve leaflets are not well visualized. No aorticregurgitation. Mitral valve normal. No mitral regurgitation. Tricuspid valveleaflets normal. No TV regurgitation. Pulmonic valve not well seen. Trivialpericardial effusion. Normal aorta. Inferior vena cava very small,suggesting central hypovolemia.CODE(S): 93308-26CARDIOVASCULAR CATHETERIZATION&INTERVENTIONPhoto Google, 201114
9/13/201129Cardiac Anatomy Four Chambers Right and Left Atria Right and Left Ventricle Four Valves Aortic Situated between the LeftVentricle and Aorta Mitral Situated between the LeftAtrium and Left Ventricle Pulmonary Situated between the RightVentricle and PulmonaryArtery Tricuspid Situated between the RightAtrium and Right Ventricle30What should a coder be looking for?Right Catheter Placement andMeasurements Left Catheter Placement andRight Atrium-RA/Ventricle-RVPulmonary Artery-PAPulmonary Capillary Wedge-PCWArterial/Aortic –AO Resistance Systemic Vascular-SVR Peripheral Vascular - PVR Blood Gases Superior Vena Cave-SVC Main PA Cardiac Output Thermal Cardiac Output Thermal Cardiac Index Fick Cardiac Output Fick Cardiac Index Measurements Left Ventricular Wall Motion Chamber SizeVentricular Pressures Diastolic and Systolic FunctionEjection Fraction – LVEFValve Function Aortic, Mitral Regurgitation and InsufficiencyCardiac Output Femoral Artery15
9/13/201131Selective Coronary Artery (SCA) Catheter Placement in one of the following: Left Atrium, Ventricle Includes Ventricular injections Left Main Branches - LM Left Anterior Descending-LAD Ramus Intermedius Circumflex-LC Obtuse Marginal-OM Right Coronary Branches - RCA Posterior Descending Artery-PDA Posterior Lateral Branch-PLB32Cardiac Catheterization - Example (CC-1)Procedures Performed: Left Heart Catheterization and SelectiveCoronary AngiographyIndication for Procedure: Ischemic Heart Disease and DyspneaPatient History: 68 year old Caucasian female referred by Dr. K Smith fora R/LHC for continued chest pain at rest and with exertion and SOB withand without exertion worse in the last few months. She said that she washaving chest pain and numbness on the left side of her body 2-3 weeksago. She was admitted to a Jackson, TN hospital and, her report says thatshe was having TIA’s. She says there was no real treatment and shewould like a more definitive answer for her sx’s. I do not believe that sheunderwent stress testing recently or while hospitalized. Other PMHincludes, HTN, obesity, Type II DM now requires metformin and insulinpump, and PVD. She was placed on Plavix about one month ago andtaken off of her aspirin while recently hospitalized though she denies anyGIB, or clotting difficulty. Depression and anxiety. She says that she hadone LHC about 20 years ago that was negative.16
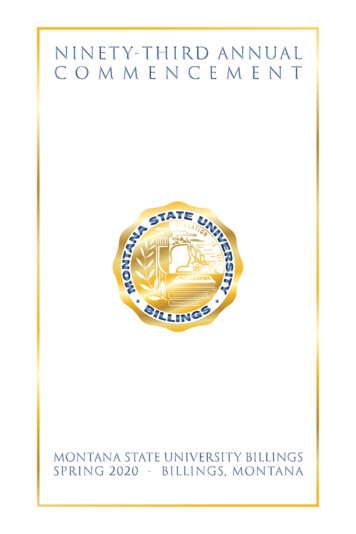
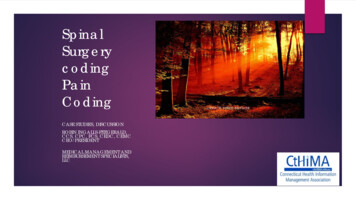
9/13/201133Cardiac Catheterization - Example (CC-2)Access/Catheter Placement: The area was prepped and draped inthe usual fashion and anesthetized with a local anesthetic. A 6FrTerumo Radial sheath was placed in the right radial artery. A 7 Frsheath was placed in the right internal jugular vein. Catheter waspositioned in the right heart system to record pressures and cardiacoutputs. A 6 Fr. pigtail catheter was used to perform left heartcatheterization, measure pressures, and perform pull back across theaortic valve. Selective coronary angiography was performed using a 6Fr Tiger catheter. Multiple injections of contrast were made into the leftand right coronary arteries with angiograms recorded in multipleprojections. Post-procedure, the arterial sheath was pulled and aclosure device was deployed. Hemostasis was attained using aTerumo TR-Band closure device. Post-procedure, the venous sheathwas pulled and pressure was applied to the site. At the completion ofthe study, the catheters were removed, hemostasis was maintained,and a dressing was applied.34Cardiac Catheterization and Intervention Example(Output) (CC-3)BaselineRight Heart PressuresRARVPAPCWArterial PressuresAOLVResistancesSVRRight Heart SatsSVCMain PAa wave 726/427/10a wave 9v wave 3mean 2v wave 6mean 17mean 5172/60139/8mean 10718 Wood units77%77%Left Hear SatsFemoral ArteryCardiac Outputs98%Thermal Cardiac Output6.11 L/minThermal Cardiac IndexFick Cardiac OutputFick Cardiac Index2.76 L/min/m29.36 L/min4.24 L/min/m217
9/13/201135Cardiac Catheterization - Example (CC-4)Diagnostic coronary Information: The coronary anatomy is right-dominant.LM is medium caliber. No angiographically significant. LAD is diffusely diseased. It has a veryproximal 70% proximal lesion just after the takeoff of high D1. LAD in the proximal and mid segmentsand moderate diffuse disease. Apical LAD has a 90% focal in a bend. The overall caliber of the LADis small due to the diffuse disease. Intracoronary nitro was given without significant change in lumensize. Circumflex is a medium caliber vessel and gives off a large OM1 and small caliber OM2. TheLCx has mild luminal irregularities diffusely. There is a mid OM1 hazy 90% stenosis prior to itsbifurcation. Moderate caliber RCA with mild diffuse proximal and mid disease. There is a 40% midRCA lesion. There is a 95% distal RCA lesion after the PDA takeoff. The PDA is small caliber withproximal diffuse 70-90% stenosis.Conclusions:Hemodynamics: The atrial pressure is normal. The pulmonary artery pressure is normal. Thepulmonary capillary wedge pressure is normal. The cardiac output was normal.Left Ventricular/Aortic Pressures and Angiography: The ejection fraction was estimated. The leftventricular overall contractility is hyperkinetic. The left ventricular end diastolic pressure is normal.The LVEDP measures 8 mmHg. LVEF is 70% with cavity obliteration with systolic contraction.Coronary Arteriography: Right dominant system with severe three vessels CAD.36Cardiac Catheterization and InterventionExample (CC-1)Procedures Performed: Left Heart Catheterization and SelectiveCoronary Angiography Indication for Procedure: Ischemic HeartDisease and DyspneaPatient History: 68 year old Caucasian female referred by Dr. K Smith fora R/LHC for continued chest pain at rest and with exertion and SOB withand without exertion worse in the last few months. She said that she washaving chest pain and numbness on the left side of her body 2-3 weeksago. She was admitted to a Jackson, TN hospital and her report, says thatshe was having TIA’s. She says there was no real treatment and shewould like a more definitive answer for her sx’s. I do not believe that sheunderwent stress testing recently or while hospitalized. Other PMHincludes, HTN, obesity, Type II DM now requires metformin and insulinpump, and PVD. She was placed on Plavix about one month ago andtaken off of her aspirin while recently hospitalized though she denies anyGIB, or clotting difficulty. Depression and anxiety. She says that she hadone LHC about 20 years ago that was negative.18
9/13/201137Cardiac Catheterization and InterventionExample (CC-2)Access/Catheter Placement: The area was prepped and draped in theusual fashion and anesthetized with a local anesthetic. A 6Fr TerumoRadial sheath was placed in the right radial artery. A 7 Fr sheath wasplaced in the right internal jugular vein. Catheter was positioned in theright heart system to record pressures and cardiac outputs. A 6 Fr.pigtail catheter was used to perform left heart catheterization, measurepressures, and perform pull back across the aortic valve. Selectivecoronary angiography was performed using a 6 Fr Tiger catheter.Multiple injections of contrast were made into the left and right coronaryarteries with angiograms recorded in multiple projections. Post-procedure,the arterial sheath was pulled and a closure device was deployed.Hemostasis was attained using a Terumo TR-Band closure device. Postprocedure, the venous sheath was pulled and pressure was applied to thesite. At the completion of the study, the catheters were removed,hemostasis was maintained, and a dressing was applied.CPT Code(s): (1) 93460-2638Cardiac Catheterization - Example (Output) (CC-3)RHCBaselineRight Heart PressuresRARVPAPCWa wave 726/427/10a wave 9Arterial PressuresAOLV172/60139/8ResistancesSVRv wave 3mean 2v wave 6mean 17mean 5mean 10718 Wood unitsRight Heart SatsSVCMain PA77%77%Left Heart SatsFemoral Artery98%Cardiac OutputsThermal Cardiac Output6.11 L/minThermal Cardiac IndexFick Cardiac OutputFick Cardiac Index2.76 L/min/m29.36 L/min4.24 L/min/m219
9/13/201139Cardiac Catheterization -Example (CC-4)Diagnostic coronary Information: The coronary anatomy is right-dominant.LM is medium caliber. No angiographically significant. LAD is diffusely diseased. It has a veryproximal 70% proximal lesion just after the takeoff of high D1. LAD in the proximal and mid segmentsand moderate diffuse disease. Apical LAD has a 90% focal in a bend. The overall caliber of the LADis small due to the diffuse disease. Intracoronary nitro was given without significant change in lumensize. Circumflex is a medium caliber vessel and gives off a large OM1 and small caliber OM2. TheLCx has mild luminal irregularities diffusely. There is a mid OM1 hazy 90% stenosis prior to itsbifurcation. Moderate caliber RCA with mild diffuse proximal and mid disease. There is a 40% midRCA lesion. There is a 95% distal RCA lesion after the PDA takeoff. The PDA is small caliber withproximal diffuse 70-90% stenosis.Conclusions: Hemodynamics: The atrial pressure is normal. The pulmonary artery pressure isnormal. The pulmonary capillary wedge pressure is normal. The cardiac output was normal.Left Ventricular/Aortic Pressures and Angiography: The ejection fraction was estimated. The leftventricular overall contractility is hyperkinetic. The left ventricular end diastolic pressure is normal.The LVEDP measures 8 mmHg. LVEF is 70% with cavity obliteration with systolic contraction.Coronary Arteriography: Right dominant system with severe three vessels CAD.Code(s): (1) 414.01 (2) 401.9, (3) 278.00 (4) 250.0040Right Heart Catheterization w/Biopsy ExampleRHC w/Biopsy- page 1Procedure Performed: Right Heart Catheterization. Endomyocardial biopsy.Patient History: 61 y/o female s/p OHT, postoperative course complicated byfungal pneumonia. Recently found to have mild rejection on biopsy 8/10/11presents for repeat biopsy.Access/Catheter Placement: The area was prepped and draped in the usualfashion and anesthetized with local anesthetic. A 0Fr sheath was placed in the rightfemoral vein. A catheter was positioned in the right heart system to recordpressures and cardiac outputs.Biopsies: A Cordis endocardial biotome was advanced to the right ventricle andmultiple biopsies were performed using standard technique. The pathology findingswill be reported separately. Biopsy Comments: Endomyocardial biopsies werecompleted without complications. The patient tolerated this procedure well.Conclusions: The right atrial pressure is normal. The right ventricular systolicpressure is normal. The pulmonary artery pressure is normal. There is elevatedpulmonary vascular resistance. The cardiac output was normal. Intervention:Successful endomyocardial biopsy.20
9/13/201141BaselineRight Heart PressuresRARVPAPCWArterial PressuresAOLVResistancesSVRPVRRight Heart SatsSVCMain PALeft Heart SatsFemoral ArteryCardiac OutputsThermal Cardiac OutputThermal Cardiac IndexFick Cardiac OutputFick Cardiac IndexLeft to Right Shunta wave 431/728/8a wave 5v wave 5mean 1v wave 5mean 17mean 2111/70139/8mean 8420.68Wood units3.34 Wood units70%73%98%4.57 L/min2.58 L/min/m24.01 L/min2.27 L/min/m20.48 L/min42Right Heart Catheterization w/Biopsy ExampleRHC w/Biopsy- page 1Procedure Performed: Right Heart Catheterization. Endomyocardial biopsy. PatientHistory: 61 y/o female s/p OHT, postoperative course complicated by fungal pneumonia.Recently found to have mild rejection on biopsy 8/10/11- presents for repeat biopsy.Access/Catheter Placement: The area was prepped and draped in the usual fashion andanesthetized with local anesthetic. A 0Fr sheath was placed in the right femoral vein. Acatheter was positioned in the right heart system to record pressures and cardiac outputs.Biopsies: A Cordis endocardial biotome was advanced to the right ventricle and multiplebiopsies were performed using standard technique. The pathology findings will be reportedseparately. Biopsy Comments: Endomyocardial biopsies were completed withoutcompli
9/13/2011 3 Medicare, Modifiers and Medical Necessity GA Modifier When to use the GA modifier? Item or service expected to be denied as not reasonable and necessary ABN--Waiver of liability on file Required to be reported on claim when Signed ABN on