Transcription
Wound Care inthe Home:Current Best PracticeClay E CollinsMSN, APRN, FNP-BC, CWOCN, CFCN, CWS, FACCWSObjectives Discuss the financial aspects of managing wound care patients inhome healthDiscuss the benefits of a product formulary and standardizedwound guidelines for controlling costs and improving patientoutcomes.Describe a systematic approach to identifying and managingchronic woundsIdentify and Differentiate Pressure vs Moisture Associated SkinDamageDescribe the DIMES model of wound bed preparation andproduct selectionDiscuss the current evidence regarding the use of honey and silverdressings.Wound Statistics 6.5 million patients with chronic wounds in U.S. 25 billion estimated annual costs14% of home care populationSen, C. , et al. (2009). Human Skin Wounds: A Major and Snowballing Threat to Public Health and the Economy. Wound RepairRegen. 2009 Nov–Dec; 17(6): 763–771. doi: 10.1111/j.1524-475X.2009.00543.x. Retrieved 10192/pdf/nihms165224.pdfJones AL, Harris-Kojetin L, Valverde R. Characteristics and use of home health care by men and women aged 65 and over. Nationalhealth statistics reports; no. 52. Hyattsville, MD: National Center for Health Statistics. 2012. Retrieved fromhttp://www.cdc.gov/nchs/data/nhsr/nhsr052.pdf1
Increasing Wound PatientDischarges to Home HealthWound Care Patients Can BreakYou!Supply management is crucial to handlingpatients with chronic wounds One of the Top 5 least profitable Diagnosis Average profit margin of 3.4% per episode Mismanagement of a wound can result in: Loss of RevenueAdverse Events InfectionsHospitalizationsLoss of ReferralsWound Care Patients Can BreakYou!Screen your patient referralsNot every admission is a good admission! Seek out a Certified Wound Care Professional Establish a Program of education and training Stick to your guns when it comes to formularycompliance. You don’t have to provide specificbrand name products. 2
Wound Care Patients Can BreakYou!Daily dressing changes Non-effective dressing regimens Brand specific demands Pt Non-adherence Who is supervising your wound patients? Do they have expertise?Do they understand how to manage woundpatients in the HH environment? Multidisciplinary Wound Team? Are you getting the outcomes? Formulary ManagementToday we must track supply costs per patient andunderstand how to analyze trends and look atbenchmarks based on diagnosis Understand that Medical Supplies are a revenuesource Requires Accurate Clinical Assessment Partnership with supply vendors Review and update your formulary regularly Benefits of a Product FormularyStandardizationEliminating waste in product duplication Creating an efficient clinical tool for product sourcing Building a time saving cross reference for productswith similar function Removing the confusion from similar products andtheir applications Cost reduction Optimal service levels Quality control MacInnes S, Falconio-West M, 20083
Benefits of Standardized WoundProtocols/GuidelinesCompliance - Increased compliance with productformulary Consistency – Every one doing the same thing the sameway Competency – Increased competency of clinical staff Confidence - Increased confidence of clinical staff leadsto increased patient confidence Confusion - Decreased confusion over product selection Cost controls – Decreased visit frequencies and supplycosts Clinical outcomes – Improved healing rates, painreduction, improved patient satisfaction Do you have a ComprehensiveWound Care Program? Comprehensive Wound Care Guidelines Requires Certified Wound ProfessionalBest Practice Interventions (EBP)Interdisciplinary ApproachImproves outcomesTreating Wounds and Preventing Pressure Ulcers nowpublicly reported on Home Health Compare Prevents Unplanned ER visits and Hospitalizations Improves Patient Satisfaction (HHCAHPS) Cost EffectiveReducing Costs and ImprovingOutcomes Comparison of Clinical Outcomes and Cost of Care between SNFresidents with chronic wounds receiving structured, comprehensivewound management protocol vs SNF residents receiving range ofwound care treatments (non-structured).Study group guided by Wound Care Specialist under contract Results: Interdisciplinary approach included: Nutrition, Support services, Wound off-loading,PT, Pain control, Vascular Compromise, Diabetes management, Functionalexpectations.47% lower cost in study group vs compare group ( 21,449.64 vs 40,678.83)35.3% lower total Medicare episode cost per day over the entire wound care episode( 229.07 vs 354.26)21 day shorter length of episode (94 days vs 115 days)Conclusion: Standardized treatments provided by a trained multidisciplinarywound care team significantly improved healing outcomes andreduced treatment costs.4
Evidence Based Practice(EBP)EBP acknowledges thatcare provided to patientsshould not be based inhabit/tradition but rathersupported by the bestpossible evidence ofeffectivenessBTTWWADIBryant R and Nix D, 2011Do You Have Wound ESP?WOUND ESPE - EtiologyS - Systemic SupportP - Prevention/Preparation/Product SelectionA Systematic Approach to Identifying andAddressing Barriers to Wound Healing*Credit for Wound ESP goes to Doughty, Dorothy, Program Director, Emory WOCN Education ProgramWound ESPPerson with Chronic WoundEtiologyIdentify and Treat Causative Factors:Pressure, Venous Insufficiency, Arterial Insufficiency, Moisture (MASD), etc.Systemic SupportAddress Systemic Factors that affect wound healingPerfusion/Oxygenation, Nutrition, Diabetes, Anemia, etc.Prevention – First and Foremost!Wound Bed Preparation/Product sture BalanceEdge/EnvironmentStalled, Non-Healing WoundsSupportive Products, Services, and Education5
EtiologyThe first step in clinically effective and cost effectivedressing selection is accurate identification of the woundetiology Etiology must be determined before treatment plan canbe developed and realistic goals established. Clues to Etiology: History and Physical re to improve is most commonly due to factors such as:Persistence of Causative Factors or Systemic Factors such as Ischemia,Infection, or Malnutrition – NOT THE DRESSING!*For wounds failing to show improvement within 2 weeks, Reassess Etiological andSystemic Factors before changing Topical TherapyBryant, Ruth A, Nix, D.P. Acute and Chronic Wounds 4th Ed. p. 83Pressure vs Moisture Associated Skin DamageAn Important Distinction Accurate Assessment and Identification of theEtiology is critical Staging skin damage that is not related topressure fails to address the etiology and alsoaffects your quality data. Failure to treat the cause results in poor healingoutcomes, and misuse of valuable resources.Pressure vs Moisture Associated Skin DamageOngoing DifferentiationPressure vs Moisture: What’s the difference? Pressure ulcers are ischemic injuries that may result in fullthickness tissue damage usually located over bony prominencesand/or under medical devices/objectsPartial thickness lesions due to moisture and/or friction do notinvolve ischemic changes and should not be classified aspressure ulcersSkin damage cause by moisture with or without friction shouldbe classified as moisture-associated skin damage (MASD)Incontinence-associated dermatitis (IAD) lesions are typicallycharacterized by partial thickness skin loss and irregular edgesLinear lesions (fissures) in the intergluteal cleft are caused bymoisture with or without friction and should be classified asintertriginous dermatitis (ITD)WOCN Consensus Statements: 2011 & 2012Mahoney, M., Rozenboom, B., & Doughty, D. (2013). Challenges in classification of gluteal cleft and buttocks wounds: consensus sessionreports. Journal Of Wound, Ostomy & Continence Nursing, 40(3), 239-245. doi:10.1097/WON.0b013e31828f1a2e6
Incontinence AssociatedDermatitis (IAD)Often misdiagnosed as apressure ulcer Prolonged contact withurine and/or feces Skin more susceptible todamage from pathogens Exacerbated by: Soaps and detergentsOcclusive containmentdevicesGray et al., 2012Intertrigo/IntertriginousDermatitis (ITD) Skin touching skinunder breastsabdominal folds groin, scrotum Intergluteal Cleft Caused by trapped moistureheatfrictionMay be complicated by fungusbacteriavirusBlack, J., Gray, M., Bliss, D., Kennedy-Evans, K., Logan, S., Baharestani, M., & . Ratliff, C. (2011). MASD part 2: incontinenceassociated dermatitis and intertriginous dermatitis: a consensus. Journal Of Wound, Ostomy & Continence Nursing, 38(4), 359-370.ISTAP Skin Tear Classification Type 1: No Skin Loss Type 2: Partial Flap Loss Linear or flap tear that can be repositioned to cover the woundbedPartial flap loss that cannot be repositioned to cover the woundbedType 3: Total flap loss Total flap loss exposing entire wound bedLeblanc, K., Baranoski, S., Holloway, S., & Langemo, D. D. (2013). Validation of a New ClassificationSystem for Skin Tears. Advances In Skin & Wound Care, 26(6), 263-265.doi:10.1097/01.ASW.0000430393.04763.c77
Traditional Treatment of Skin Tears(No longer considered evidence-based treatment) Traditional dressings: Transparent Films Do not handle fluid wellPooling and leaking of fluid onto surrounding skinAdhesive - can cause epidermal stripping or tearing of the skinupon removal“Non-adherent” pads with topical antibiotics Adhere to skin and wound and can cause damage with removalDo not provide an optimal moist environment for healingRequire more frequent changesMore costly and labor intensiveNeomycin is a very common sensitizing agentIndiscriminate use of antibiotics promotes resistanceTreatment of Skin Tears Experts generally discourage use oftransparent films, closure strips, andhydrocolloid dressings because theirremoval can cause more skin damageand pain Alternatives include: Hydrogel/Hydrogel Sheet dressingsNon-adherent mesh contact layerdressingsAlginate/Gelling fiber dressingsNon-adherent Foam dressingsCyanoacrylate liquid skin protectantPetroleum based dressings (Xeroform,Vaseline Gauze, etc.) – Poor moisturebalance properties, may dry and adhereto wound bed causing trauma uponremovalDon’t Do This!!!Systemic Support Provide Systemic Support for wound healing Address underlying co-morbidities Diabetes – Tight Glucose ControlMeasures to support perfusion/oxygenation Nutritional Support Hydration Identify and Treat infection (local & systemic) Other barriers to wound healing Address potential enzyme imbalances within thewound8
Wound ESPPerson with Chronic WoundEtiologyIdentify and Treat Causative Factors:Pressure, Venous Insufficiency, Arterial Insufficiency, Moisture (MASD), etc.Systemic SupportAddress Systemic Factors that affect wound healingPerfusion/Oxygenation, Nutrition, Diabetes, Anemia, etc.Prevention – First and Foremost!Wound Bed Preparation/Product sture BalanceEdge/EnvironmentStalled, Non-Healing WoundsSupportive Products, Services, and EducationWound BedPreparation/Product SelectionDIMESD – Debridement I – Infection/Inflammation M – Moisture Balance E – Edge/Environment S – Support Products, Services and Education *But first, you must determine your goal for this wound.Goals for Wound Care HealableIndividual whose body can support the phasesof healing within expected lifetime Aggressive wound treatment Maintenance An attempt to keep a wound from deterioratingby providing comprehensive careNon-healable (Palliative)Individual who cannot support the phases ofwound healing within the expected lifetime Comfort rather than cure Sibbald, R., Goodman, L., Woo, K., Krasner, D., Smart, H., Tariq, G., & . Salcido, R. (2011).Special considerations in wound bed preparation 2011: an update. Advances In Skin & WoundCare, 24(9), 415-436. doi:10.1097/01.ASW.0000405216.27050.979
Wound Cleansing Prior to dressing change & assessmentRemove surface contaminantsBioburden, debris, toxins Minimize chemical and mechanical trauma Protect the healing wound Wound Cleansing Agents Skin cleansers and soaps should only beused on intact skin Do not clean ulcer wounds with skin cleansers orantiseptic agents (e.g., povidone iodine, iodophor,sodium hypochlorite solution [Dakin's solution],hydrogen peroxide, acetic acid).Skin cleansers contain chemicals that are cytotoxic towound tissue and should not be used as woundcleansers.(AHCPR Pressure Ulcer Treatment Guidelines, 1994)Normal Saline May be sufficient for clean woundsIn the majority of cases, water or saline is sufficient for cleansinga proliferative or granulating wound. Avoid wound cleansersthat may be cytotoxic to the granulating wound tissue. (WOCNPressure Ulcer Guidelines, 2010)Agency for Health Care Policy and Research, U.S. Department of Health and Human Services. (1994). Treatment of pressure ulcers in adults (AHCPRPublication No. 95-0652). Rockville, MD: Author.Rodeheaver G ,1999; WOCN, 2010Wound Cleansing Agents Commercial Cleanser withsurfactants Antimicrobial Cleansers Reduces surface tensionReleases debris from the wound bedBenzethonium chlorideCHG irrigantAntiseptic Cleansers Sodium hypochloriteAcetic acidHypochlorous acid(should only be used in limitedcircumstance for short periods of time)Rodeheaver G ,1999; WOCN, 201010
“D” -- DebridementRemove Non-Viable or Deficient TissueTypes of Debridement Surgical/sharp Mechanical (Wet-to-Dry) Enzymatic (Collagenase) Maggot Hydrosurgery Autolytic Advanced Wound Care DressingsPolyacrylateMedical Grade HoneyHypertonic drosurgeryPolyacrylate – Gentle AND EffectiveRinses & debrides for up to 24 hoursCreates a moist wound healing environment More effective than wet gauze therapy – greatalternative to wet-to-dry dressings Will not stick to wound, gentle for patient Easy to apply, easy to teach to patients and caregivers Can reduce microorganisms and binds MMPs Offers rapid debridement Average rate of debridement 38.11% of the wound surface area perwk11. (Paustian, Stegman The use of polyacrylate-containing Dressings for Wound Debridement, September 2002)11
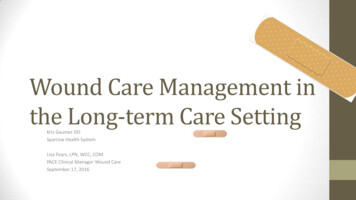
Medical Grade Honey Available in variety of carrier dressingsPromotes autolysis by Pulling fluid into the wound bed (Osmosis)Produces H2O2 - activating MMP’sMay have anti-inflammatoryproperties Change frequency: Can be left in the wound up to7 days. Depends on woundcondition and drainage levels. Canbe changed daily if necessary.Bryant and Nix, 2011Promotes Autolytic Debridement High sugar content (87%) leads to osmosis –fluid moving from high to low concentrations ofsugar1,2The osmotic action of honey pulls lymph fluid from tissue layersup through the wound. The fluid and enzymes actually preventslough or necrotic tissue from adhering and/or breaks theconnection from the wound bed.Fluid from deeper tissue clears debris (deadtissue and bacteria) while moving towards sugarat wound bed1,2,31. Molan, Peter C. “Debridement of wounds with honey”. Journal of Wound Technology (5) 12-15. 2009.2. Molan, P.C. “A brief review of the use of honey as a clinical dressing”. Primary Intention (The Australian Journal of WoundManagement) 6(4) 148-158. 1998.3. Molan, Peter. “Honey: A modern wound management product”. Wounds-UK Books. 2005.Promotes Autolytic Debridement12
Low pH pH: 3.2 to 4.5 (acidic)Lowering pH helps kick startdifficult, stalled wounds Research shows that for woundswith a pH 7.6, each reduction of0.1 pH units was associated with an8.1% reduction in wound size1Lowering the pH of the wound alsoinhibits bacterial growthMay result in transient stinging dueto lowering of pH1. Gethin, GT et al. “The impact of Manuka honey dressings on the surface pH of chronic wounds.”Int Wound J. 2008 Jun;5(2):185-94.Current EvidenceThe Cochrane Review Cochrane Collaboration meta-analysis was based onstudies of 14 different types of honey.Of the 25 studies included for review only one studyinvestigated an FDA-cleared Manuka honey product.The review did not review the use of Manuka Honeyfor debridementThe reviewers concluded that the evidence on honey’sefficacy in wound healing is inconclusiveThis position taken by the Cochrane reviewers is notunusual in the field of wound therapies, whether theybe drugs or devices.The current evidence is sufficient and clear thatManuka Honey based wound dressings are beneficialfor promoting wound healing and autolyticdebridement“I” -- Infection or InflammationReduce Microorganisms and Inflammatory Cells13
Identify and Treat Infection All open wounds are contaminated withmicroorganisms – low levels of bacteria actually seemto stimulate repair but high levels severely retard orprevent repair. The assessment of infection in a chronic wound is aclinical skill and the decision to prescribe antibiotics orapply topical antimicrobial agents should be basedprimarily on clinical presentations. Sibbald G, Woo K, Ayello E,2009WOCN Pressure UlcerGuidelines RecommendationsConsider a 2 week course of topicalantibiotics/antimicrobial dressing for cleanwounds that do not heal or continue toproduce purulent exudate after two to fourweeks of standard wound careAHCPR,1994;WOCN, 2010NPUAP/EPUAP Guidelines “Consider the use of topical antimicrobial silver ormedical-grade honey dressings for pressure ulcersinfected with multiple organisms, because thesedressings offer broad antimicrobial coverage.”“Limit theuse of topical antibiotics on infected pressureulcers, except in special situations.In general, topical antibiotics are not recommended forpressure ulcers. Reasons for this include inadequatepenetration for deep skin infections, development ofantibiotic resistance, hypersensitivity reactions, systemicabsorption when applied to large wounds, and localirritant effects, all of which can lead to further delay inwound healing.”European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel. Treatment of pressure ulcers: QuickReference Guide. Washington DC: National Pressure Ulcer Advisory Panel; 2009.14
How is the Antimicrobial Activity of Silver Dressings Affectedby the Presence of Medical Grade Honey Dressing?Yang QP, David KT , Schultz GS.Institute for Wound Research, University of Florida, Gainesville, FloridaConclusionsThe combination of a medicalhoney gel contact layer does notinterfere with the antibacterialeffects of the silver antibacterialbarrier ion dressings in vitro The combinations of the honeygel with the silver dressingsincreased the reduction ofbacterial levels compared toeither silver dressings ormedical honey alone. Antimicrobial DressingsBactericidal – an agentthat destroys bacteria SilverCadexomer iodineCHGCationic polymersBacteriostatic – an agent that iscapable of inhibiting growth ormultiplication of bacteria Gentian violet/methylene blue Hydrofera blue (Hollister)DACC (dialkylcarbamoyl chloride) Polyacrylate Glycerin based hydrogel Derma-Gel (Medline)Elasto-Gel (Southwest Technologies)Many others Sorbact (BSN Medical)TenderWet (Medline) SilverThe most common antimicrobial agent used inmodern advanced wound dressings Broad spectrum of antimicrobial action includingantibiotic resistant organisms Enough silver to kill microbes Aerobes/Anaerobes, Fungus, MRSA, VRE,Pseudomonas, E. ColiReduces proteases and inflammatory cytokinesReduces release of exotoxinsNo known medically significant resistanceNo known allergies to ionic silver15
The Use of Silver as an Antimicrobial Antiquity1000 BCVessels for water Ravelin1869Antimicrobial effect Crede1881Ophthalmic rinse von Behring1887Anthrax Burke1964Silver nitrate for burns Fox1968Silver Sulfadiazine Medline1995/96Arglaes Film Westaim1995/96Acticoat for burns Medline2002SilvaSorbThings to consider when selectinga Silver Dressing Ionic vs. metallic Ionic compatible with cleansers, saline or waterMetallic compatible with sterile water NOT NS(refer to manufacturer instructions)Continuously delivered vs. bolus Noncytotoxic to wound and host Silver release activated by: Moisture from skin, atmosphere or external sourceAppropriate Use of SilverDressings in WoundsInternational Consensus Panel The major roles for antimicrobialdressings such as silver dressings inthe management of wounds are to:Reduce bioburden in acute or chronicwounds that are infected or are beingprevented from healing bymicroorganisms - Treatment Act as an antimicrobial barrier for acute orchronic wounds at high risk of infection orre-infection - Prophylaxis Leaper, D. (2012). Appropriate use of silver dressings in wounds: International consensus document. International Wound Journal, 9(5),461-464. doi:10.1111/j.1742-481X.2012.01091.x16
Appropriate Use of SilverDressings in WoundsTreatment - THE TWO WEEK 'CHALLENGE' The two week “rule” for silver use should beconsidered a two week 'challenge' period during whichthe efficacy of the silver dressing can be assessed. If after two weeks: There is improvement in the wound, but continuing signsof infection – it may be clinically justifiable to continuethe silver dressing with further regular reviewsThe wound has improved and the signs and symptoms ofwound infection are no longer present – the silverdressing should be discontinuedThere is no improvement – the silver dressing should bediscontinued and consideration given to changing thedressing to one that contains a different antimicrobialagent and if the patient is unwell using a systemicantibiotic and re-evaluating possibly untreatedcomorbidities.Appropriate Use of SilverDressings in Wounds PROPHYLACTIC USE“Antimicrobial dressings such as silverdressings may be used as a barrier tomicroorganisms in wounds at high risk ofinfection or re-infection. Examples may include: burns, surgical wounds,pressure ulcers near the anus, wounds withexposed bone, or wounds in patients who areimmunocompromised, have poor circulation,unstable diabetes or neoplastic disease.Other Bactericidal Dressings Cadexomer Iodine Cationic Polymers Iodoflex / Iodosorb (Smith & Nephew) PHMB (polyhexamethylene biguanide) Biocides XCELL AM, Kerlix AMD (Covidien)BIOGARD (Derma Sciences/Medline)CHG (chlorhexidine gluconate) Biopatch (Systagenix)Hibiclens17
“M” -- Moisture BalanceAbsorb Excess Exudate, Prevent DessicationNot toowetNot toodryMaintain Moist Wound SurfaceDressings that provide a moist woundenvironment:Enhanced cell migrationDecreased cell death Decreased risk of infection Increased Leukocyte activityProvides a Bacterial Barrier“A dry cell is a dead cell”Moisture Balance DressingsDry to Minimal Drainage Transparent Films Opsite (Smith & Nephew Suresite (Medline)Moderate to Heavy DrainageAlginates/Gelling Fibers Tegaderm (3M) Hydrocolloids Foams Comfeel (Coloplast) DuoDerm (ConvaTec) Exuderm (Medline) Hydrogel Intrasite Gel (S & N) NormLgel (Molnlycke) Amophorous SilvaSorb (Medline) Derma-Gel (Medline) Elasto-Gel (Southwest Technologies) OptifoamAllevyn (S & N)Lyofoam (Convatec)Optifoam (Medline)Polymem (Ferris)Super Absorbent Polymer SheetsKaltostat (Convatec)Maxorb Extra (Medline)Melgisorb (Molnlycke)Aquacel (Convatec)Opticell (Medline)Optilock (Medline)Sorbion Sachet ( Sorbion AG)Xtrasorb (Derma Sciences)Super Absorbent Foams Optifoam Gentle(Medline)Xtrasorb Foam (Derma Sciences)Mepilex (Molnlycke)18
Polysaccharides in Wound Dressings Polysaccharide - a carbohydrate that can be decomposedby hydrolysis into two or more molecules ofmonosaccharides; especially : one (as cellulose, starch, orglycogen) containing many monosaccharide units andmarked by complexity. Popular polysaccharides in wound dressings: Cellulose - The major structural material of plants. (Wood islargely cellulose; Cotton is almost pure cellulose) i.e. Gauze carbohydrates2.htmlPolysaccharides in Wound Dressings Popular polysaccharides in wound dressings: Alginates – Extracted from seaweeds such as giant kelp. Consist ofrandom sequences of chains of β-D-mannuronic and α-L-guluronicacids attached with 1 4 linkages. Readily absorb fluid. Alginates are used in the manufacture of textiles, paper, and cosmetics.The sodium salt of alginic acid, sodium alginate, is used in the foodindustry to increase viscosity and as an emulsifier. Also found in foodproducts such as ice cream and in slimming aids where they serve asappetite suppressants. In dentistry, alginates are used to make dentalimpressions.Carboxymethylcellulose –. Hydroxyl groups (-OH) are substitutedwith carboxymethyl groups (-CH2COOH). Also referred to as Cellulose Gum which is used as a thickener for foodsand as an emulsion stabilizer in products like ice cream. Cellulose gum isalso used in personal lubricants, diet pills, water-based paints, detergentsand paper coatings.And now, ChitosanChitosan is the principle derivative ofchitin.Second most abundant naturalpolysaccharide after cellulose.Naturally abundant and renewable.19
What is Chitosan?Linear Polysaccharide Molecule consisting of a long chain of sugarmolecules Different from Glucose and SucroseDerived from Crustacean Shells Chemically modified Purified SterilizedBiological Properties of ChitosanBiocompatible Natural Polymer Biodegradable Safe, Non-toxicMedical Properties Hemostatic Fungistatic Immunoadjuvant Regenerative effect on connective gum tissue Accelerates bone formationDutta, P.K., Dutta, J., Tripathi. V. S., (2004). Chitis and chitosan: Chemistry, properties and applications. Journal of Scientific &Industrial research. 63 (20-31).Why Chitosan?Much Research Exists on Chitosan (more thanalginate or carboxymethyl cellulose in terms ofinteraction of the material with tissue)Used as a hemostat by the militaryTaken as a weight loss supplementUsed in water filtrationUsed in Cosmetics20
Why Chitosan? (cont.)The amino group has a pKa value of 6.5, so at aphysiological pH range of 5-7, the amino group isprotonated, meaning it has a positive charge.Chitosan becomes a polycationic supermolecule in bodyfluid. HWhat is a polycationic supermolecule? Ions are atoms or molecules which have gained or lost one or morevalence electrons giving the ion a net positive or negative charge. Cations are ions with a net positive charge.Examples: Silver: Ag , hydronium: H 3 O , and ammonium: NH 4 Anions are ions with a net negative charge.Examples: hydroxide anion: OH - , oxide anion: O 2- , and sulfateanion: SO 4 2- Cations bind to negatively charged bacterial cell wallsExamples: Silver, Chlorhexidine, etc Chitosan Based Dressings AbsorbentGel formingImproved conformability andcontact with wound bedInherit benefits of Chitosan21
Super Absorbent PolymerDressings Increased absorptive capacityFewer dressing changesDressings with non-adherentfacingLess disruption to the woundPromotes faster healingProtection from periwoundmacerationOdor control capabilityAppropriate for minimal toheavy exudateGreat secondary dressing whenusing honeyUse of a Superabsorbent Dressing to Control CopiousDrainage in Patients with Venous UlcerationsStudy Six patients with copious amounts of drainageand history of periwound adhesive related skininjury requiring three times a day using siliconebased foam dressings* Dressing regimen changed to superabsorbentnon-adhesive dressing for one monthResults: All patients had a reduction in wound dressingchanges to a maximum of once daily. (Mean 1.9days; range 1-3 days) Improved periwound maceration was observed intwo patients and resolved in four Three patients reported no wound pain onremoval with three reporting a 90% reduction No episodes of periwound adhesive denudationsMilne, C & Saucier, D. Use of a Superabsorbent Dressing to Control Copious Drainage in Patients with VenousUlcerations. Presented at The Symposium on Advanced Wound Care, Dallas, TX, April 2011Superabsorbent Foam DressingsFoam facingSuperabsorbentpolymer core Increased absorption Increase fluid retention With or withoutadhesive borders 22
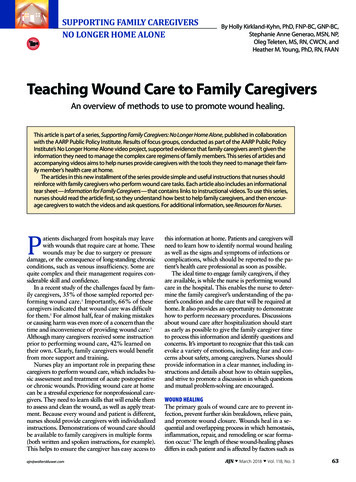
Wicking Fiber Dressings Wicking Fiber dressings Rapid transfer of exudateaway from woundenvironmentAids in removal of bacteria,MMP’s, sloughNon-adherentEffective moisturemanagement in heavilydraining wounds“E” – Edge/EnvironmentConvert Non-Advancing Edge to Advancing EdgeNon-advancing EdgeAdvancing EdgeFailure of the epidermal edge of a chronic wound to migrate over granulationtissue of a chronic wound is probably due to abnormal extracellular matrixcomponents that are damaged by excess proteases and senescent cells.Pictures by Dr. Falanga and Dr. WarrinerNon-Healing Wounds Stalled, Non-Healing Wounds require: Aggressive treatmentAdvanced technology dressings Collagen dressingsExtracellular Matrix DressingsGrowth FactorsMore expensive but worth the investment ifwound is not healing. Time is money! CMS expects wounds to healOutcomes Healing If the wound isn’t healing you are losing money! 23
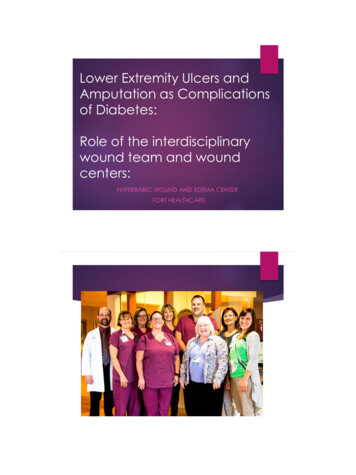
Imbalanced Molecular Environments OfHealing And Chronic WoundsHealing Wounds:LOW LEVEL OF MMPs,HIGH LEVELS OF ANTI MMPsChronic Wounds:HIGH LEVELS OF MMPs,LOW LEVELS OF ANTI MMPsB.A. Mast and G.S. Schultz. Wound Rep Reg 4:411-420, 1996.Protease Enzyme ImbalancesFailure of the epidermal edge of a chronic wound tomigrate over granulation tissue of a chronic wound isprobably due to abnormal extracellular matrixcomponents that are damaged by excess proteases andsenescent cells Matrix Metalloproteases (MMP’s) destroy collagen,extracellular matrix, and growth factors Elastase activates MMP’s and destroys anti-MMP’s Non-advancing Edge Advancing EdgePictures by Dr. Falanga and Dr. WarrinerProtease Enzyme Imbalances Wound healing can be improved by locallymanipulating growth factors, extracellularmatrix (ECM), and the signaling pathwaysthat regulate migration, proliferation,differentiation and metabolism of cells.Woo KY, Ayello EA, Sibbald RG. Using DIMES to your ad
the Home: Current Best Practice Clay E Collins MSN, APRN, FNP-BC, CWOCN, CFCN, CWS, FACCWS Objectives Discuss the financial aspects of managing wound care patients in home health Discuss the benefits of a product formulary and standardized wound guideli