Transcription
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O NThe Effectiveness of Cognitive-Existential Group Therapy onReducing Demoralization in the ElderlyRoya Marsa (1)Bahman Bahmani (2)Maede Naghiyaee (3)Somayeh Barekati (4)(1) MA, Department of Counseling, University of Social Welfare and Rehabilitation Sciences,Tehran, Iran(2) Associate Professor, Department of Counseling, University of Social Welfare and RehabilitationSciences, Tehran, Iran(3) PHD, Department of Counseling, University of Social Welfare and Rehabilitation Sciences,Tehran, Iran(4)MA, Department of Counseling, University of Social Welfare and Rehabilitation Sciences,Tehran, IranCorresponding author:Bahman BahmaniAssociate Professor, Department of Counseling,University of Social Welfare and Rehabilitation Sciences,Tehran, IranEmail: ba.bahmani@uswr.ac.irAbstractIntroduction and Objective: Elderly people faceexistential issues such as death, loss of meaningin life, fear of death, lack of life and last chances.If people, cannot effectively confront it, this lossof meaning in life, will form the main core of a setof syndromes that are called “demoralization”. Thisstudy aims to investigate the effectiveness of cognitive-existential therapy on reducing demoralizationin the elderly.Method: The present study was carried out usinga pretest-posttest semi-experimental design withcontrol group and random assignment. The statistical population included all the elderly women in YasDaily Rehabilitation Center. In this study, 22 peoplewere selected through non-random sampling andafter answering the demoralization scale (Kissane,2004) and Cognitive Distortions Questionnaire(Abdollahzade et al. 2010 quoted from FarmaniShahreza et al. 2016) they were randomly assigned to experimental and control groups (eachgroup included 11 people). The experimental groupparticipated in 12 cognitive-emotional grouptherapy sessions (each session 90 minutes) oncea week, but the control group did not receive anyintervention. The collected data were processedusing SPSS-20 software to calculate covarianceanalysis.42Results: The results showed a significant reduction in the demoralization and cognitive distortions compared to the pretest. Also, in a two monthfollow-up session, demoralization andcognitivedistortion scores were significantly reduced compared to pretest.Conclusion: Cognitive existential group therapy onthe one hand, due to addressing the existential issues of the elderly, and, on the other hand, workingwith their irrational beliefs and replacing rational beliefs, can have an effect on reducing of the demoralization syndrome in the elderly.Key words: cognitive-existential group therapy,demoralization, cognitive distortions, the elderlyPlease cite this article as: Marsa R. et al.The Effectiveness of Cognitive-Existential GroupTherapy on Reducing Demoralization in the Elderly inIran World Family Medicine. 2017; 15(10):42-49DOI: 10.5742/MEWFM.2017.93136WORLD FAMILY MEDICINE/MIDDLE EAST JOURNAL OF FAMILY MEDICINE VOLUME 15 ISSUE10, DECEMBER 2017M I D D L E E A S T J O U R N A L O F FA M I LY M E D I C I N E V O LU M E 7 , I S S U E 1 0
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O NIntroductionElderly refers to a stage of life which occurs followingbiological, biochemical and anatomical changes in bodycells. The changes generally begin after age 60 and affectgradually body cell functions. Being elderly isn’t an illnessbut a natural evolution which can’t be stopped or reversed(World Health Organization, 2001).Iran is a country with a large aging population. About 8.3percent of population was over 60 in 2012 (Iran, 2012.According to statistics, nearly 10 million elderly peopleare expected by 2022, which means approximately 10percent of Iran’s population in that time (Darani, Abedi, &Riji, 2009).Elderly people may confront difficulties in differentdimensions such as severe financial constraints, physicaldisabilities or existential conflicts. In the physical dimensionthey may face problems such as: 1- chronic illnesses(blood pressure, cardiovascular disease and diabetes)2- progressive vision and hearing loss 3- neurologicaland psychiatric disorders such as Dementia, Alzheimersand Depression (Duberstein, Pálsson, Waern, & Skoog,2008).Socio-economic problems which old age people sufferfrom, include financial problems, losing job and socialstatus, death and loss of friends, peers and loved ones(Wurtman, 1993). Isolation due to physical weakness anddiminished mobility is also reported (Mussen, Conger,Kagan, & Houston, 2002).The other dimension, with regard to psychological problemsthat older people suffer from include: loneliness (Alpass& Neville, 2003; Heravi Karimloo et al., 2008; Wurtman,1993), impatience, anger, absurdity, anxiety, insomnia andfatigue (Kaldi, Ali Akbari, & Foroghan, 2004).Aging can trigger existential distress which recalls fearof death. Seeing friends and peer groups getting canceror cardiovascular disease reminds them that they havestepped into the final stages of life. Elderly people areaware of their limited time but they have much unfinishedbusiness. This makes them change their life style but alsocan give rise to conscious feelings of fear and anxiety(Vincent, 2003).According to existential approach, we face existentialconcerns such as death, isolation, meaninglessness,responsibility and freedom during our lives. The humansearch for foundational supporting structures for existencedeals with deeper levels of anxiety. Although every humanbeing needs to be immortal , stable and have a role modelto follow, all of us confront existential concerns such asdeath, absurdness and isolation (Yalom, 1980).Even though existential distress is a normal reaction to theconcept of inexistency as a consequence of consciousness,if the person fails in coping efficiently with existential crisis,it may cause distress and demoralization (Blinderman &Cherny, 2005; Leung & Esplen, 2010).The starting point of demoralization syndrome is a sense ofincompetency and inefficiency in dealing with a debilitatingsituation which leads to some fundamental questions. If theperson fails in finding proper answers to these questions,he/she might end up with demoralization syndrome.Therefore, the most specific feature of demoralizationsyndrome is failure in adding value and meaning to life (D.W. Kissane, Clarke, & Street, 2001).Kissane and Clarke (2001) considered demoralization as apsychiatric diagnosis for existential suffering and suggesteddiagnostic criteria as following: 1- hopelessness, loss ofmeaning and purpose in life 2- pessimistic attitudes andthoughts, helplessness, feeling trapped and failed, lackof a worthwhile future 3-lack of motivation for copingdifferently 4- social isolation and feelings of losing support5- symptoms persistence for more than two weeks 6- Thesymptoms are not attributable to major depression oranother psychiatric disorders.Kissane(2011) believes that despite some phenomenologicalsimilarities between depression and demoralizationsyndrome, these two concepts are basically different.A depressed person is not satisfied with his past, notpleased with his present and also disappointed aboutthe future and even when the course of action is clear hemay not be able to experience overall pleasure and is notmotivated enough to persist steadfastly in pursuing thetask and experience pervasive anhedonia. While a personwith demoralization syndrome does not have seriousproblem with his past. Although he’she might be able toexperience pleasure at the moment, due to the confusion(not knowing what to do and what he can do), practically hefeels helpless, inadequate, suppressed and experiencesanticipatory anhedonia and he sees future as worthless(Clarke & Kissane, 2002).Beside aging hardships, elderly people might faceexistential concerns such as death, loss, absurdness,meaninglessness and regret of missed opportunities.They might face challenges to make meaning in their lives(Yalom, 1980). If they cannot find a genuine answer to theirexistential issues they will suffer pathological anxiety.One of the important dimensions of demoralizationsyndrome is cognitive distortion in finding meaning. Thedemoralized have negative and black and white thoughtsabout events and have self-contempt, exaggeration, andlow self-confidence (Watson & Kissane, 2011). Sincedemoralization syndrome consists of emotional, cognitiveand behavioral components, it seems that any interventionto decreasing its symptoms should cover cognitivecomponents which are effective in forming new thoughtsand meaning.A range of psychological interventions have been used toreduce the psychological problems of the elderly, whichindicates the need for psychological services for theseelderly people. This range includes: cognitive-behavioraltherapies (Hedayat, 2015; Barghi Irani, 2015), existentialgroup therapy (Mooziri, 2013), spirituality-based cognitivetherapy (Rahimi, 2014), group logo therapy (Poorebrahim,WORLD FAMILY MEDICINE/MIDDLE EAST JOURNAL OF FAMILY MEDICINE VOLUME 15 ISSUE 10, DECEMBER 2017M I D D L E E A S T J O U R N A L O F FA M I LY M E D I C I N E V O LU M E 7 , I S S U E 1 043
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O N2006; Fakhar, 2007, Yazdan Bakhsh, 2015); memory telling(Majzoobi, 2012), hope therapy (Parvaneh, 2015) andcognitive-existential therapy (Barekati & Bahmani, 2017).The literature indicates that existential group therapyand group logo therapy were not effective on the elderly(Mooziri, 2013; Poorebrahim, 2007; Fakhar, 2007).Furthermore, the focus of most interventions for the elderlyhas been on the treatment of death anxiety, feelingsof loneliness, depression, and enhancement of lifeexpectancy, happiness, self-efficacy, mental health, qualityof life and quality of sleep in the elderly. It seems essentialto address the anxieties because of their prevalencewhile less attention has been paid to demoralization in theelderly.It would be beneficial to find the most effective andpractical intervention method to reduce the demoralizationsubsequent to aging due to the need to respect thehuman rights of the elderly and also to save time, effortand facilities. In cognitive-existential group therapy, it aimsto use techniques of “cognitive therapy” to refine someschemas, negative automatic thoughts, and to correctthe cognitive errors that contribute to the formation ofpsychological distress caused by the non-genuine responseto existential anxiety. Moreover, this method pays attentionto existential concerns such as death anxiety, uncertainty,meaninglessness, loneliness, and uncontrollability of theworld that are intensified by the death threat in patients. Inmost intervention methods such concerns do not receivesystematic attention. Therefore, it is expected that throughthis intervention, individuals will find their own unknownfears and conflicts over the issues of existence and willbe able to cope with them in a genuine and effective way(Bahmani, 2010). Previous studies indicate that cognitiveexistential therapy plays an effective role in reducingpsychological distress in different populations (Bahmani,2010; Naghyiaee, 2014, Farmani Shahreza, 2014; Paknia,2015). In this regard, we seek to investigate the impact ofthis intervention on the elderly and to answer the questionof “whether cognitive-existential group therapy can reducedemoralization in the elderly?”MethodThe study was carried out using a pretest-post-test semiexperimental design with control group and randomassignment. The statistical population included all theelderly women in Yas Daily Rehabilitation Center. Thesample included 22 people selected through a nonrandom sampling from among the elderly present in thecenter during the sampling period (spring 2017) who wereprepared to participate in the group therapy and who wereeligible for inclusion criteria. The sample was divided intoexperimental and control groups in a random assignment(11 individuals in each group).In this research, the dependent variable is measuredbefore and after the presentation of the independentvariable, and its design graph is as follows:44T1 and T 4 represent the pretest, T2 and T5 the posttest,T3 and T6 show the follow-up and X is the CognitiveExistential Group Therapy.InstrumentsIn this research, Demoralization scale syndrome wasused to measure demoralization. Demoralization Scale(DS) is a 24-item scale and contains 5 subscalesincluding meaninglessness, helplessness, feeling failure,disheartened and dysphoria. An alpha coefficient for theDS scale was reported as 94%. The Persian version ofthe scale was translated and administered by Bahmaniand Naghiyaee (2014) among women with breast cancerand its alpha coefficient was reported as 86%. In orderto measure cognitive distortions, the 20-item scale ofCognitive Distortions developed by Hassan Abdollahzadehand Maryam Salar (2010) was used. The standardizedCronbach’s alpha was 80%.ProcedureAfter preliminary studies and preparation of the protocol,and receiving a referral letter from the University of Welfareand Rehabilitation Sciences to the Welfare Organizationof Tehran province, we got the necessary permissionsand referred to the Yas Daily Rehabilitation Center. Theresearch process began after permission was gainedfrom the head of the Center. First, through broadcastingannouncements and talks with the elderly in the Yas DailyRehabilitation Center, they were informed of the study.Subsequently, after describing the research goals andobtaining consent from the elderly and observing the ethicalrules, the conditions for the participation in the researchwere prepared. After interviewing from the individualscompleting demoralization and Cognitive Distortionsquestionnaires, 22 elderly were selected according toinclusion and exclusion criteria and randomly assignedto the control and experimental groups. The inclusioncriteria were: age of 60 and over, having the ability tospeak, having no cognitive problems and a score of over30 in the Demoralization scale. Exclusion criteria included:having mind and brain disorders such as Parkinson’s anddementia, having any psychiatric disorders based on thewritten contents of their file in the center and use of anypsychotherapy and counseling services at the time of theresearch.Subsequently, cognitive-existential group therapy wasperformed for 12 sessions of 90 minutes and once a weekfor the experimental group (Table 1), while the controlgroup received no intervention. In order to observe ethicalissues, after group treatment with the experimental group,group therapy was also performed for the control group.At the last session, the mentioned questionnaires wererepeated on the participants of both groups. In order toensure the durability of the therapeutic results, two monthsafter the completion of the group therapy in the followWORLD FAMILY MEDICINE/MIDDLE EAST JOURNAL OF FAMILY MEDICINE VOLUME 15 ISSUE 10, DECEMBER 2017M I D D L E E A S T J O U R N A L O F FA M I LY M E D I C I N E V O LU M E 7 , I S S U E 1 0
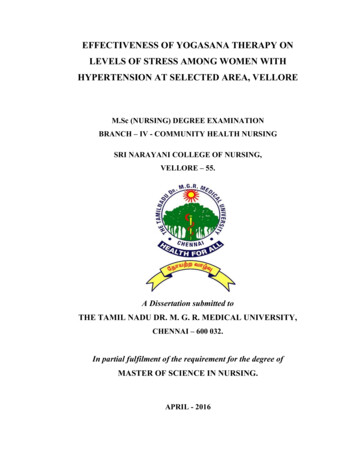
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O NTable 1: the protocol for cognitive-existential group therapyup phase, the participants again were assessed usingquestionnaires.Data from pretest and posttest was entered in version20 of SPSS software. After analyzing the assumptions ofcovariance analysis, this statistical method was used toanalyze the data. Covariance analysis limits or eliminatesthe effect of the pretest variable and measures it using theregression equation. Among the important assumptions ofthis statistical method was the homogeneity of variancesusing Levene’s test and Normality test by Kolmogorov–Smirnov test. These assumptions were checked andverified in the study.The ethical considerations of this study included thefollowing topics: 1) the participants in the research wereassured that the information received would be confidential;2) scores were given to those who would like to knowtheir scores; 3) the planning of group counseling sessionswas carried out in a way that would not interfere with theprograms of the Yas Daily Rehabilitation Center; 4) Thecontrol group was assured that they would participate ineight sessions of Cognitive-Existential group therapy afterthe end of the research; 5) Any of the participants couldfreely leave the program at any time during the research.ResultsThe sample consisted of 22 elderly women with an averageage of 69 who were randomly assigned into two groupsof 11 in experimental and control groups (waiting list).According to the results of the Mann-Whitney U test, thetwo groups were homogeneous in demographic variablesof age and education. In addition, the assumptions of thecovariance test for the normality of the data distributionwere confirmed by Kolmogorov-Smirnov test andhomogeneity of variances were confirmed by Levin’s testof two groups in dependent variables of demoralizationand cognitive distortions.In Table 2, the comparison of mean scores in the pretest,posttest and the two-month follow up of the experimentalgroup showed that the scores in the posttest and follow-upwere reduced compared to the pretest.WORLD FAMILY MEDICINE/MIDDLE EAST JOURNAL OF FAMILY MEDICINE VOLUME 15 ISSUE 10, DECEMBER 2017M I D D L E E A S T J O U R N A L O F FA M I LY M E D I C I N E V O LU M E 7 , I S S U E 1 045
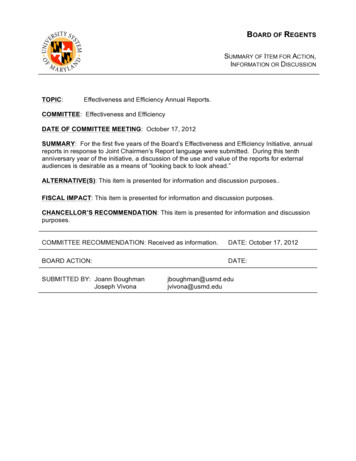
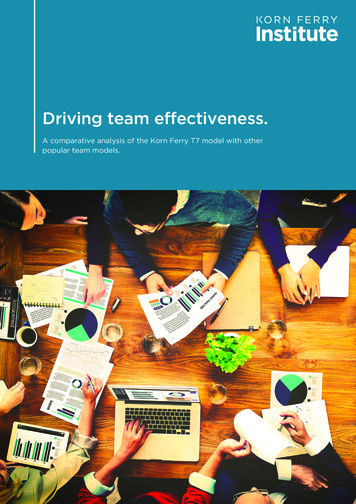
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O NTable 3: Mean and standard deviation of cognitive distortion scores in pretest, posttest and follow upIn Table 3, the comparison of mean scores of cognitive distortions in the pretest, posttest and follow-up tests showedthat scores in post-test and follow-up were increased in comparison with the pretest. Considering that the higher thenumber of scores, the more positive the thinking is; the increase in scores shows that the cognitive distortions havebeen decreased.Table 4: The results of covariance analysis of the comparison of the experimental group and control group indemoralization and its subscales’ post-test scoresAs shown in Table 4, participation in the cognitive- existential group therapy has significantly decreased the demoralizationand its subscales in the elderly. Also in the follow-up phase, a significant decrease was continued.Table 5: The results of covariance analysis of the comparison of the experimental group and control group incognitive distortion post-test scores46WORLD FAMILY MEDICINE/MIDDLE EAST JOURNAL OF FAMILY MEDICINE VOLUME 15 ISSUE 10, DECEMBER 2017M I D D L E E A S T J O U R N A L O F FA M I LY M E D I C I N E V O LU M E 7 , I S S U E 1 0
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O NAs shown in Table 5, participation in the cognitiveexistential group therapy has significantly decreased thecognitive distortion in the elderly. Also in the follow-upphase, a significant decrease was continued.DiscussionThe present study was performed to investigate the generalassumption that “cognitive-existential group therapyreduces demoralization of the elderly”.The demoralization total mean score were declared asfollowing: pretest (40.27), posttest (27.36) and Follow up(28.54). The results revealed that cognitive-existentialgroup therapy reduces demoralization of the elderly.Although previous research didn’t mention a direct link onthe effectiveness of cognitive-existential group therapy inreducing demoralization in the elderly we considered thepresent results consistent with cognitive-existential grouptherapy on reducing demoralization in various populationssuch as people who have: cancer (Kissan et al,1997.,Kissan et al, 2003., Breitbart, 2001., Bahmani et al,2010.,Naghiay & Bahmani,2014), AIDS (Farmani Shahreza &Bahmani,2016) and MS (Paknia & Bahmani,2015), whichshowed the effectiveness of cognitive-existential grouptherapy on reducing demoralization.As the findings in Table 4 show, the findings confirmthe mentioned hypothesis. It seems that the cognitiveexistential group therapy and the elements proposed in thetreatment protocol, as well as the special way of relationsin the sessions have been able to create a positive andsignificant change in reducing demoralization and itssubscales. It should be considered that the treatmentatmosphere in the cognitive-existential group therapyis based on listening to the subject’s stories consideringthe here and now, familiarity with the sufferings of others,the use of emotional support and receiving feedback fromdifferent people to reduce the feeling of being a victim, theuniqueness of the problem, loneliness and helplessness,discrimination and oppression, feeling of security, secrecy,reflection and empathy, emotional release, self-disclosure,exposure, feedback, affection, acceptance and humour;this can be mentioned as a positive factor for this approach.In this method, the group continued the sessions assumingthat the confidence and sympathy between the groupmembers persists and the psychological refinement wasdone every session.Part of the content of the cognitive-existential grouptherapy helps understanding the phenomenological worldof individuals using the prepared existential concepts.Using such concepts helps individuals to encounter theirexistential anxiety and to communicate with their originalselves with all the inevitable existential anxieties and insteadof denying and reprimanding their unpleasant feelings andemotions, experience them and take responsibility for theirfeelings, and most importantly, express these feelings andemotions. According to Kissane it is a useful interventionmethod that can deal with these fears fast and clear enoughand can help reduce mental health problems (Kissane, etal., 2002; quoted from Bahmani et al., 2010).During the treatment process, the elderly were involvedwith their existential questions. These questions causedthem to activate and discharge their existential anxieties.In general, during the sessions, it became clear that thefeeling of lack of a worthwhile future and lack of selfefficacy to achieve it, inevitability and fear of death, lack offaith in the future, feeling of hopelessness, lack of meaningand purpose, and loneliness deprives the elderly from themotivation to try. Existential crisis and disturbances aredeveloped as a result of fear of confrontation with existentialanxieties. So during the group process, we tried to helpthe elderly understand the unpredictability of the worldand the uncertainty of the universe, assess their thoughtsand assumptions about the uncontrollability of death andloss of opportunities in the past and the resulting anxieties,identify and challenge their cognitive distortions aboutthe meaning of death anxiety (seeing death as the endof everything, unwillingness to track down their illnesses,fear of being forgotten after death, fear of painful death,disqualifying their efforts in their lives, fear of disability) andend their fears by accepting the anxiety of unpredictabilityand death. We also tried to introduce the concept offundamental loneliness anxiety and help them identify andchallenge their cognitive distortions about the meaningof loneliness (not being understood by close people,especially their spouse and children, the feeling of failing tounderstand others, the feeling of separation from children,attachment to other individuals to escape loneliness) andaccept loneliness as a genuine experience to increase thedesire and motivation to be with others and family members.They were also helped to challenge the meaning of theirlives created by psychological disturbances and existentialanxieties, and find a meaningful term for their lives, andchange their attitudes toward problems and tolerance ofdifficulties, and through giving meaning to the sufferingsand pains, change their focus from what has been lost,because the sense of the new meaning and purpose inlife during the aging period (which includes the ability tocombine and integrate the experiences and achieve anunderstanding of themselves and the world) is a protectivefactor against meaninglessness. Also, in the process ofgroup therapy, elderly people tried to accept responsibilityand freedom of choice, to identify and challenge theircognitive distortions about the anxiety of responsibility andfreedom of choice (assigning responsibility for life eventsto others or social, cultural, economic, etc. circumstances,leaving the choice to others, believing in luck, trying toshow oneself as victim ) and to evaluate their prioritiesand decisions, and accept their own responsibility for theirown destiny. In general, the group therapist tried to helpthe elderly to accept cognitive distortions that preventedthem from experiencing demoralization and activated theirdefense mechanisms.In general, according to previous studies cognitiveexistential group therapy can be considered as a suitablefactor in reducing different types of mental disorders.Bahmani et al. (2010) in their research showed thatWORLD FAMILY MEDICINE/MIDDLE EAST JOURNAL OF FAMILY MEDICINE VOLUME 15 ISSUE 10, DECEMBER 2017M I D D L E E A S T J O U R N A L O F FA M I LY M E D I C I N E V O LU M E 7 , I S S U E 1 047
O R I G I N A L CO N T R I B U T I O N / C L I N I C A L I N V E S T I G AT I O Ncognitive-existential group therapy was more effectivethan cognitive therapy in reducing the mean of depressionand increasing the mean of hopefulness.Previous studies, consistent with the present study, ofKissane et al. (1997) showed that using this method oftreatment is helpful to reduce the amount of sadness andgrief in patients with cancer, increase their problem solvingability and also create cognitive strategies. Breitbart (2001)suggested that existential therapies are one of the mostappropriate approaches to reduce depression and increasehope in cancer patients. In addition Kissane et al. (2003)concluded that cognitive-existential therapy has a positiveeffect in reducing overall symptoms of psychologicaldistress in women with non-metastatic breast cancer. Inanother study, Kissane et al. (2004) concluded that thismethod would greatly reduce psychological distress andanxiety, and improve family relationships.Therefore, according to the findings, the cognitiveexistential therapy has been able to affect people withchronic conditions such as cancers, breast cancer, humanimmunodeficiency virus, and the elderly. This should bedue to the main distinguishing feature of this interventionmethod, namely, paying attention to the existential anxietiesand considering here and now during the treatmentsessions as compared to other methods.Also, the results of the two-month follow-up showed thatcognitive-existential group therapy has a lasting and stableeffect on the improvement of demoralization. In explainingthis finding, it can be said that Cognitive-Existentialpsychotherapy can lead to long-term changes in terms ofcreating philosophical insights and changing attitudes inindividuals.ConclusionsIn general, cognitive-existential group therapy due toaddressing the existential concepts, especially for theelderly and dealing with these concepts and working withthe unreasonable beliefs of individuals and substitutinglogical beliefs can lead to the reduction of psychologicalfactors and existential anxieties. Therefore, this method ofintervention can be used in the treatment of the elderly,since the elderly need to continue their lives with meaningand purpose without fear of confrontation with death,loneliness, and existential concerns.LimitationsThe most important limitation of this study was researchin the only daily rehabilitation center, which reduced thegeneralization power of the research.SuggestionsGiven that existential anxiety is activated in the elderly andaddressing these anxieties in counseling and psychotherapysessions can help to improve the existential crisis of theelderly, it is suggested that counselors of care centers,48rehabilitation centers for the elderly and counseling andpsychology clinics be trained based on the treatment planpresented in this study and take advantage of it to help theelderly. In addition, the results of this study can be usedto improve the design of educational programs for healthcare and rehabilitation providers, as well as to plan forprevention of existential crises and to improve the health ofthe elderly and to prevent serious problems such as suicidein the elderly. Also, it is suggested that the effect of thistherapeutic approach on other psychological variables beexamined and the effectiveness of this treatment methodbe compared with other types of cognitive therapies inorder to reduce the psychological problems of the elderlyin order to achieve the most effective treatment methodfor this group.AcknowledgmentsThanks to my distinguished professors and the respectablestaff of Yas Daily Rehabilitation Center and all the elderlywho helped us with this research. In addition, the presentarticle uses master’s thesis results that were supportedby the University of Social Welfare and RehabilitationSciences.References- Alpass, F. M., & Neville, S. (2003). Loneliness, health anddepression in older males. Aging & mental health, 7(3),212-216.- Bahmani B, Etemadi A, Shafieabadi A, Delavari A,Ghanbari M. (2010) Cognitive-existential group therapy andcognitive instructional therapy for breast cancer patients.Developmental Psychology: Iranian Psychologists;6(23):201-14.- Barekati, S., Bahmani, B., Naghiyaaee, M., Afrasiabi,M., & Marsa, R. The Effectiveness of Cognitive-ExistentialGroup Therapy on Reducing Existential Anxiety in theElderly. Middle East Journal Of Family Medicine, 7(10),75- Barghi, I.Z., Dehkhoda, A. M., Begian, K. M., (2015).Effectiveness of cognitive behavioral therapy on the statusof memory and sleep in the elderly, Aging Psychology,1(1), 19-30.- Blinderman, C. D., & Cherny, N. I. (2005). Existentialissues do not necessarily resul
Conclusion: Cognitive existential group therapy on the one hand, due to addressing the existential is-sues of the elderly, and, on the other hand, working with their irrational beliefs and replacing rational be-liefs, can have an effect on reducing of the demor-alization syndrome in the elderly. Key wor