Transcription
*VNUP[P]L )LOH]PVYHS ;OLYHW MVY LWYLZZPVU PU L[LYHUZ HUK 4PSP[HY :LY]PJLTLTILYZ;OLYHWPZ[ 4HU\HS(T LUaLS 7O .YLNVY 2 )YV U 7O )YHKSL , 2HYSPU 7O
Cognitive Behavioral Therapy for Depressionin Veterans and Military ServicemembersTherapist ManualAmy Wenzel, Ph.D.Gregory K. Brown, Ph.D.Bradley E. Karlin, Ph.D.Suggested Citation: Wenzel, A., Brown, G. K., & Karlin, B. E. (2011). Cognitive BehavioralTherapy for Depression in Veterans and Military Servicemembers: Therapist Manual.Washington, DC: U.S. Department of Veterans Affairs.
TABLE OF CONTENTSTABLE OF FIGURES AND EXHIBITS .iiiACKNOWLEDGEMENTS .ivPREFACE .1INTRODUCTION .3What Is Cognitive Behavioral Therapy? .3Organization of This Manual .3Cases .4PART I: COGNITIVE BEHAVIORAL MODEL .7Underlying Theory of CBT .7Cognitive Theory .7Basic Cognitive Model .8Characteristics of Automatic Thoughts .8Expanded Cognitive Model .10Behavioral Theory.13Integration of Cognitive and Behavioral Theory .16CBT Case Conceptualization .16PART II: GENERAL SESSION STRUCTURE .37Brief Mood Check .37Bridge from Previous Session .41Agenda Setting .43Review of Previous Session Homework .47Discussion of Agenda Items .50Periodic Summaries .51Homework Assignment .52Final Summary and Feedback .57Implementing the Session Structure .58PART III: INITIAL PHASE OF TREATMENT.61Initial Clinical Assessment.62Motivational Enhancement .62Short-Term Goals .63Consequences of Psychological Symptoms .65Benefits of Reducing Psychological Symptoms .67Attitudes and Expectations Toward Treatment .67Obstacles to Participating in Treatment .70Socialization into CBT .72Setting Treatment Goals .75Suicide Risk Assessment and Safety Planning .76PART IV: MIDDLE PHASE OF TREATMENT .79Behavioral Strategies .79Activity Monitoring.79Activity Scheduling .87Pleasant Events Schedule .93Alternative Activity Scheduling Strategies .95Behavioral Activation .99Graded Task Assignment .100Relaxation Training and Controlled Breathing .101CBT for Depression in Veterans and Military Servicemembers: Therapist Manuali
Cognitive Strategies .103Working with Automatic Thoughts .104Identifying Automatic Thoughts .104Evaluating Automatic Thoughts .110Coping Cards.120The 3Cs Approach: Catch It, Check It, Change It .123Working with Core Beliefs .124Core Belief Identification .124Core Belief Modification .126Problem-Solving Strategies .134Evaluating Pros and Cons .140PART V: LATER PHASE OF TREATMENT .143Reviewing Progress Toward Treatment Goals .143Review and Consolidation of Skills .144Additional Treatment Planning .145Continuation of Treatment .145Tapering Treatment Sessions .145Referring for Additional Treatment .146Termination of Treatment .146CONCLUSION .148REFERENCES .151GLOSSARY .155APPENDIX .159CBT for Depression in Veterans and Military Servicemembers: Therapist Manualii
TABLE OF FIGURES AND EXHIBITSFigure 1.1: General CBT Approach .7Figure 1.2. Basic Cognitive Model .8Figure 1.3. Negative Cognitive Triad .10Figure 1.4. Expanded Cognitive Model .11Figure 1.5. Levels of Cognitive Processing .12Figure 1.6. Vicious Cycle of Depression .14Figure 1.7. General CBT Paradigm .16Figure 1.8. Cognitive Conceptualization Diagram .18Exhibit 1.1. Cognitive Conceptualization Diagram for Jack .22Exhibit 1.2. Cognitive Conceptualization Diagram for Kate .26Exhibit 1.3. Cognitive Conceptualization Diagram for Michael .29Exhibit 1.4. Cognitive Conceptualization Diagram for Claire .33Figure 1.9. Timeline of CBT.35Figure 3.1. Balance Between Relationship-Enhancing and CBT Strategies .62Exhibit 3.1. Treatment Goals for Sample Cases .76Exhibit 4.1. Kate’s Activity Monitoring Form .84Exhibit 4.2. Excerpt from Kate’s Activity Schedule Form .93Exhibit 4.3 Claire’s Modified Activity Schedule .96Figure 4.1. Three-Column Thought Record .107Exhibit 4.4. Jack’s Three-Column Thought Record: Step #1 .108Exhibit 4.5. Jack’s Three-Column Thought Record: Step #2 .108Exhibit 4.6. Jack’s Three-Column Thought Record: Step #3 .109Figure 4.2. The Link Between Situations, Emotions, and Thoughts .110Figure 4.3. Five-Column Thought Record .114Exhibit 4.7. Kate’s Five-Column Thought Record: Step #4.116Exhibit 4.8. Kate’s Five-Column Thought Record: Step #5.117Exhibit 4.9. Claire’s Coping Card.122Figure 4.4. Catch It, Check It, Change It. .123Exhibit 4.10. Claire’s Pros and Cons . 141CBT for Depression in Veterans and Military Servicemembers: Therapist Manualiii
ACKNOWLEDGMENTSSupport for this manual was provided by the Office of Mental Health Services, VACentral Office, U.S. Department of Veterans Affairs.CBT for Depression in Veterans and Military Servicemembers: Therapist Manualiv
PREFACEIn an effort to bring evidence-based psychotherapies from the laboratory to thetherapy room and realize the full potential of these treatments for Veterans, theDepartment of Veterans Affairs (VA) has developed national initiatives todisseminate and implement evidence-based psychotherapies for depression,posttraumatic stress disorder (PTSD), serious mental illness, and other conditionsthroughout the Veterans Health Administration (VHA), the health care arm of VA. Aspart of this effort, VA has developed a national staff training program in CognitiveBehavioral Therapy (CBT) for depression. This training in CBT represents the largestCBT training initiative in the nation. The overall goal of the CBT for DepressionTraining Program is to provide competency-based training to VA mental health staff,which includes experientially based workshop training followed by ongoing, weeklyconsultation with an expert in the treatment. The training focuses on both the theoryand application of CBT for the treatment of depression on the basis of the protocoldescribed in this manual, which has been adapted specifically for the treatment ofdepressed Veterans and Military Servicemembers. Initial program evaluation resultshave shown that the training and implementation of this therapy protocol by VAmental health therapists have significantly enhanced therapist skills and patientoutcomes (Karlin, 2009; Karlin et al., 2010). This manual is designed to serve as atraining resource for therapists completing the VA CBT for Depression TrainingProgram, as well as for others inside and outside of VHA and the military who areinterested in further developing their CBT skills.Although the focus of this manual is on the application of CBT for depression, themanual and treatment protocol are based on core CBT competencies that can beadapted and applied to treat other mental health and behavioral health conditions. Inthis protocol, cognitive and behavioral theory and strategies are incorporated in anintegrated fashion and guided by a careful case conceptualization, which is animportant component of this treatment. In addition, the protocol placessignificant emphasis on the therapeutic relationship, which is a critical We believe that CBT done wellcontextual variable in CBT. We believe that CBT done well requires a requires a very strong andvery strong and supportive therapeutic alliance. In this way, CBT for supportive therapeutic alliance.Depression in Veterans and Military Servicemembers stronglyemphasizes the therapy in Cognitive Behavioral Therapy and differs from morepsychoeducational or primarily skills-based approaches to CBT. In our experience,case conceptualization-driven treatment and the focus on the therapeutic relationshipare especially important therapy ingredients when working with depressed Veterans.Included throughout this manual are fictitious cases that represent composites ofdepressed Veterans and Military Servicemembers we have treated. These cases aredesigned to illustrate and make concrete the application of CBT skills with “real-life”patients. In addition to this manual, we have developed a companion therapist trainingvideo (U.S. Department of Veterans Affairs, 2010) that demonstrates many CBTstrategies with the case examples presented in this manual. Key therapist and patientworksheets and forms for use in implementing this protocol are referenced throughoutthis manual and are provided in the Appendix.CBT for Depression in Veterans and Military Servicemembers: Therapist Manual1
Whether you are new to CBT or are seeking to expand your CBT skills, our hope isthat this manual will be a useful resource to you and will help promote the deliveryand fidelity of CBT with depressed Veterans and Military Servicemembers.CBT for Depression in Veterans and Military Servicemembers: Therapist Manual2
INTRODUCTION
INTRODUCTIONWhat Is Cognitive Behavioral Therapy?Cognitive Behavioral Therapy (CBT) is a structured, time-limited, present-focusedapproach to psychotherapy that helps patients develop strategies to modifydysfunctional thinking patterns or cognitions (i.e., the “C” in CBT) and maladaptiveemotions and behaviors (i.e., the “B” in CBT) in order to assist them in resolvingcurrent problems. A typical course of CBT is approximately 16 sessions, in whichpatients are seen on a weekly or biweekly basis. CBT was originally developed totreat depression (A. T. Beck, 1967; A. T. Beck, Rush, Shaw, & Emery, 1979), and ithas since been adapted to the treatment of anxiety disorders (A. T. Beck & Emery,1985), substance use disorders (A. T. Beck, Wright, Newman, & Liese, 1993),personality disorders (A. T. Beck, Freeman, Davis, & Associates, 2004), eatingdisorders (Fairburn, 2000), bipolar disorder (Basco & Rush, 1996), and evenschizophrenia (A. T. Beck, Rector, Stolar, & Grant, 2009)! Many patients showsubstantial improvement after 4 to 18 sessions of CBT (Hirsch, Jolley, & Williams,2000). Contemporary research shows that CBT is efficacious in treating mild,moderate, and severe mental health symptoms (e.g., DeRubeis et al., 2005; Elkin etal., 1989), that it is equally as efficacious as psychotropic medications in the shortterm, and that it is more efficacious than psychotropic medications in the long term(see Hollon, Stewart, & Strunk, 2006, for a review). There is a great deal of researchsupporting CBT’s efficacy for treating an array of mental disorders using bothindividual (Butler, Chapman, Forman, & Beck, 2006) and group (Craigie & Nathan,2009) formats. CognitiveBehavioralTherapyOrganization of This ManualThis manual is organized into five main parts: (a) cognitive behavioral theory and themanner in which the theory translates to treatment, (b) CBT session structure, (c)interventions that take place in the initial phase of treatment, (d) interventions thattake place in the middle phase of treatment, and (e) interventions that take place in thelater phase of treatment.Throughout these five main parts, case examples created on the basis of actualclinical experience are provided to illustrate the application of cognitive andbehavioral strategies. Moreover, specific pointers for implementing the strategies, aswell as common obstacles that therapists experience and ways to overcome them, aresummarized. This manual was written specifically for implementing CBT withVeterans and Military Servicemembers. The content of the protocol, as well asspecific issues in the application of CBT, are presented with this particular populationin mind. In addition, certain therapy components and processes are given emphasis inthis protocol to address commonly observed issues in the delivery of CBT withdepressed Veterans and Military Servicemembers. For simplicity, we primarily usethe terms patients and Veterans. These terms are used interchangeably and areinclusive of active duty Military Servicemembers (including members of all branchesof the military and reserve forces).CBT for Depression in Veterans and Military Servicemembers: Therapist Manual3
CasesIn the pages that follow, we present descriptions of four fictitious cases throughoutthis manual to illustrate the strategies that have been described.JACKJack is a 63-year-old Vietnam Veteran who has been in and out of mental healthtreatment for the past 20 years. He has a history of depression, anger, and significantimpairment in his relationships with his wife, children, and co-workers. Recently, Jackwas let go from his job as a manager at a car dealership; although he was told that hewas laid off because the company was downsizing, he believes that the regionalmanager has “had it out” for him for many years. Jack had expected to work for anotherfive years, but he has been unable to find a new job that is acceptable to him. As aresult, he reports significant financial concerns. In addition, Jack’s relationships with hiswife and children continue to deteriorate. His children live out of town, and when theycall they want only to speak with his wife. He and his wife barely speak, and they sleepin separate rooms. Jack has a few “buddies” with whom he plays poker, but he claimsthat he does not feel comfortable “crying to them” about his problems. Finally, Jack hasbeen experiencing medical problems that have increasingly been of concern to him. Hehas recently developed diabetes that is secondary to chronic pancreatitis, and he hasexpressed frustration at the strict diet and medical regimen that he must maintain.MICHAELMichael is a 24-year-old, African American, Operation Enduring Freedom/OperationIraqi Freedom (OEF/OIF) Veteran who was referred to treatment for depression andsuicide ideation. He recently returned from Iraq after serving in the Army for two years.He joined the military as a means of paying for school, and, unexpectedly, he wasmobilized for an OIF deployment in his senior year of college. He left a girlfriend, hisschooling, and a promising part-time job for a 12-month deployment that ultimately wasextended to almost 18 months. During his time in Iraq, Michael survived the force of anIED explosion, after which he was unconscious for two days. In the time since he hasreturned from Iraq, he has become increasing isolated from others and is estranginghimself from his family and loved ones. Michael tried to return to his part-time job, buthe left after two weeks because he found it difficult to concentrate and made manyerrors. He states that he has no plan for the future and wonders whether his life isworth living. Neuropsychological testing at his local VA Medical Center revealed mildbrain injury. He has significant concern about his current abilities and his perceivedreliance on others.KATEKate is a 40-year-old National Guard nurse who recently returned from deployment tofind that her husband had left her and moved with her kids to another state. In addition,despite thinking that she was going to retain her job upon her return, she found that thehospital where she worked replaced her, given that her deployment was a voluntaryextension of her original tour. In theatre, the option of extending was not presented toher as a choice and, thus, she assumed that her previous position would be protected.Kate’s efforts to find a job in her small town have been unsuccessful, and her husbandhas not been cooperative with arranging times for visitation. Her depression hasbecome increasingly severe, and for the past three weeks, she has stayed in bed most ofeach day. Kate also reports significant symptoms of anxiety and has had four panicattacks in the past week.CBT for Depression in Veterans and Military Servicemembers: Therapist Manual 4
CLAIREClaire is a 28-year-old Army CPT rotary wing pilot (Blackhawks) who experienced severeinjuries from a crash in Afghanistan. While flying a low-level search-and-rescue mission,her rotary system was hit by a rocket-propelled grenade, and the helicopter losthydraulic power and ultimately crashed into a mountain side. Two soldiers were killed inaction, and most on board were severely injured. Claire endured significant leg injuries,and she is unable to walk without assistance. Claire reports that she has beenexperiencing a great deal of tension and apprehension over the past few months. She iseager to return to flying, but she is encountering major obstacles from her commandand from the military more generally. She is waiting for her medical board to becomplete so that she may return to flying and perceives that they are putting her offbecause they do not believe that an amputee can fly. She has few outside interests andclose relationships to keep her occupied as she is waiting for this decision. In addition,Claire becomes extremely irritable when she perceives that she is treated differentlybecause of her injury.This manual illustrates the manner in which all four of these individuals are treatedwith CBT. The next part describes cognitive behavioral theory and the manner inwhich the theory can be applied to understanding their clinical presentations.CBT for Depression in Veterans and Military Servicemembers: Therapist Manual5
PART I: COGNITIVEBEHAVIORAL MODEL
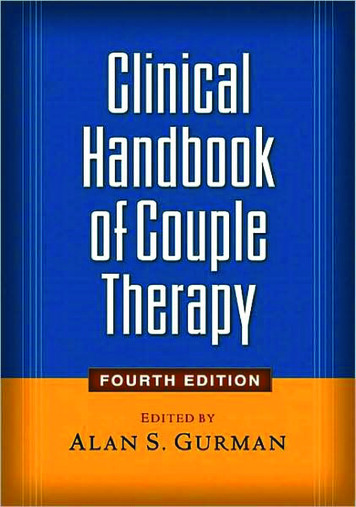
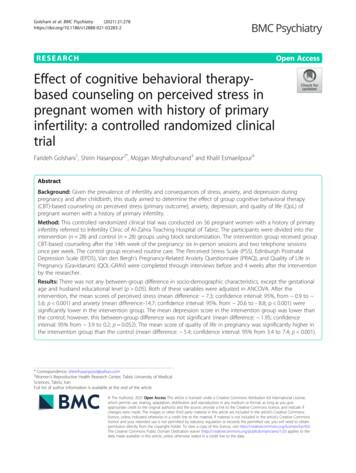
PART I: COGNITIVE BEHAVIORAL MODELUnderlying Theory of CBTFor any type of psychotherapy, it is important to understand the underlying theory sothat patients’ symptoms can be integrated into a coherent conceptualization, andtreatment strategies that follow logically can be identified. CBT is no different.According to the cognitive behavioral model, emotional experiences are influencedby our thoughts and behaviors. Mental health problems arise when people exhibitmaladaptive and extreme patterns of thinking and behavior, and these often interactwith each other to escalate patients’ symptoms and problems. The following is avisual description of the general CBT approach.Figure 1.1: General CBT ApproachSituation General CBTapproachThoughtBehaviorEmotionAs is illustrated in Figure 1.1, there is no one cause of mental health problems.Instead, the interplay between stressful life situations, dysfunctional or unhelpfulthoughts, highly charged emotions, and maladaptive behaviors causes andexacerbates patients’ symptoms. There are two theoretical approaches that contributeto CBT—cognitive theory and behavioral theory. Both of these theories are describedbriefly in the following sections.Cognitive Theory CognitivetheoryThe word cognition refers to the process of knowing or perceiving. Thus, the centralfocus of cognitive theory is on thinking and the manner in which ourthought content and styles of information processing are associated with According to cognitive theory,our mood, physiological responses, and behaviors. According to the manner in which we thinkcognitive theory, the manner in which we think about, perceive, about, perceive, interpret,interpret, and/or assign judgment to particular situations in our lives and/or assign judgment toaffects our emotional experiences. Two people can be faced with similar particular situations in our livessituations, but because they think about those situations in different affects our emotionalways, they have very different reactions to them.experiences.CBT for Depression in Veterans and Military Servicemembers: Therapist Manual7
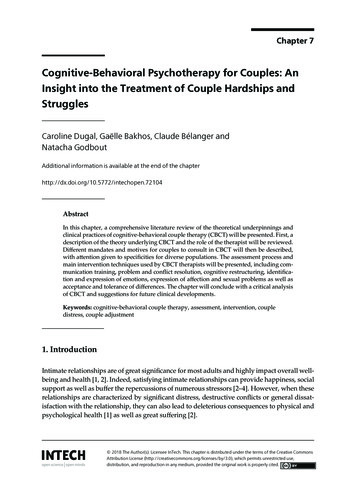
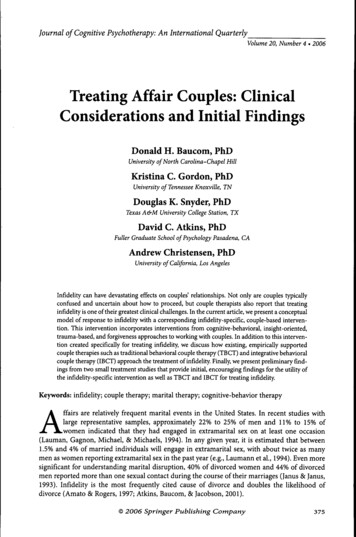
CASE EXAMPLES: JACK AND KATEBoth Jack and Kate recently lost their jobs, both continue to be unemployed, and bothhave impaired relationships with their spouses and children. When Jack thinks aboutthese problems, he thinks, The world has screwed me over. Everyone I know makes mylife difficult. I’m better off without them. Kate, in contrast, thinks, My life means nothingnow. I’m a horrible person because I cannot do what I wish to do. Not surprisingly, Jackand Kate report two different emotional experiences—Jack’s primary emotionalexperience is anger, whereas Kate’s primary emotional experience is depression. Jack’ssubsequent behavioral response is to ignore his wife and children and complain abouthis life, whereas Kate’s behavioral response is to cry and stay in bed most of the day.Basic Cognitive ModelWe refer to the thoughts that arise in response to particular situations or events asautomatic thoughts. The term automatic is used because these thoughts occur soquickly that they are often not recognized by the patient and, more importantly, thesignificant impact these thoughts have on subsequent emotional and behavioralreactions goes unnoticed. Despite the fact that these thoughts emerge very quickly,they often have profound effects on our mood because they offer some sort ofevaluation or judgment of our current circumstance. We refer to this sequence as thebasic cognitive model. Figure 1.2 is a visual description of the basic cognitive model. AutomaticthoughtsFigure 1.2. Basic Cognitive ional,Physiological,Behavioral) BasiccognitivemodelCharacteristics of Automatic ThoughtsThere are some additional important points to keep in mind about the basic cognitivemodel and the nature of automatic thoughts. First, the situation need not always be anexternal event in one’s environment. In fact, memories, thoughts, emotions, andphysiological sensations can prompt additional automatic thoughts.CASE EXAMPLE: JACKJack often thinks back to an argument he had with his supervisor over a year ago. As herecalls their conversation, he thinks to himself, My supervisor never respected the yearsof hard work that I put into the company. He subsequently becomes angry all over againdespite the fact that he has not spoken to his supervisor since he was laid off. Thebehavioral consequences of this include moping around, watching television instead ofactively looking for another job, and being short with his wife.CBT for Depression in Ve
Cognitive Behavioral Therapy (CBT) is a structured, time-limited, present-focused approach to psychotherapy that helps patients develop strategies to modify dysfunctional thinking pat