Transcription
THE VETERANS AFFAIRS (VA) CONTIUUM OF FAMILY SERVICES TOMEET THE NEEDS OF VETERANS AND THEIR FAMILIESSusan J. McCutcheon, RN, EdDNational Mental Health Director, Family Services, Women’s Mental Healthand Military Sexual TraumaShirley M. Glynn, PhDClinical Research Psychologist, Mental Health Services and VA Greater LosAngeles Healthcare SystemResearch Psychologist, David Geffen School of Medicine, UCLASeptember 21, 20121
Overview of Presentation Evolution of Family Services in the VA The Continuum of VA Family Services Preventive Interventions to Develop FamilyResilience Initiatives to Provide Family Education Veteran Centered Brief Family Consultation Marriage and Family Counseling in VA Staff Training Overview and Outcomes New Initiatives and ProgramsVETERANS HEALTH ADMINISTRATION2
Evolution of Family ServicesVETERANS HEALTH ADMINISTRATION3
Development of Family Servicesin VA Mental Health President’s New Freedom Commission on Mental Health Report(2003) - Mental Health Care is Consumer and Family Driven VA Secretary’s Mental Health Strategic Plan (FY 2005) – Based onRecommendations that were relevant to Veterans and families VHA Handbook – Uniform Mental Health Services in VA MedicalCenters and Clinics (FY 2008)– Section on Family Services Office of Mental Health Services emphasis on Recovery-OrientedProgramming which included Family Services Office of Mental Health Services emphasis on Evidence-BasedPractices (EBPs) which included EBPs for Veterans and FamiliesVETERANS HEALTH ADMINISTRATION4
38 USC § 1782. Counseling, Training, and MentalHealth Services for Immediate Family Membersand CaregiversServices provided include: Training/Education, Consultation, Marriage and FamilyCounseling as are necessary in connection with thattreatmentEligible individuals who may be provided services: Members of immediate family or legal guardian of a Veteran Family caregiver of eligible Veteran or a caregiver of acovered Veteran (those terms are defined in PL 111-163) Individual in whose household such Veteran certifies anintention to liveVETERANS HEALTH ADMINISTRATION5
Uniform Mental Health Services inVA Medical Centers and ClinicsFamily ServicesMinimum clinical requirements for VHA Mental HealthServices: Providers discuss family involvement with patient atleast yearly and at inpatient discharge Treatment plan to identify family contact or reason forlack of contact Providers must seek consent from Veterans to contactfamilies in the future, as necessaryVETERANS HEALTH ADMINISTRATION6
Uniform Mental Health Services inVA Medical Centers and Clinics Family consultation, family education or familypsychoeducation for Veterans with serious mentalillness must be provided at VA Medical Centers andvery large CBOCs Opportunities for these family services must beavailable to all Veterans with serious mental illness onsite, by telemental health, or with communityproviders through sharing arrangements, contracting,or non-VA fee basis careVETERANS HEALTH ADMINISTRATION7
CONTINUUM OF VA FAMILYSERVICESVETERANS HEALTH ADMINISTRATION8
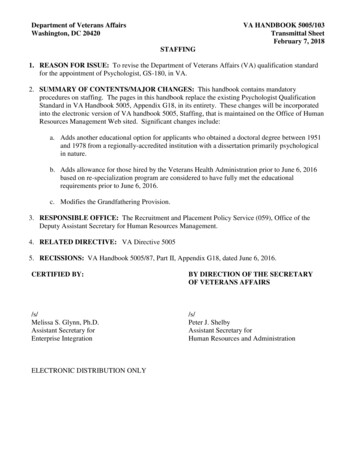
Continuum of VA Family Services Consistent with a recovery philosophy agraduated continuum of services is necessary tomeet the varied needs of our Veterans. The full continuum ranges from:—Prevention/ Resiliency Training—Family Education / Training—Brief Problem-Focused Consultations—More Intensive Marriage and FamilyCounseling and Family PsychoeducationVETERANS HEALTH ADMINISTRATION9
Continuum of VA Services for FamiliesPrevention/EducationFamily land Family CounselingMoving Forward/Power Of TwoVeteran Centered BriefFamily ConsultationIntegrative Behavioral CouplesTherapy with attention toInterpersonal Violence,Parenting, and Same Sex CouplesNAMI Family toFamilySupport andFamily Education(SAFE)OperationEnduring FamiliesTalk, ListenConnect SesameStreet ProgramVETERANS HEALTH ADMINISTRATIONBehavioral Couples Therapy forSubstance Use with attention toInterpersonal Violence andParentingCognitive-behavioral CouplesTherapy for PTSD (first trainingscheduled 2/13)Behavioral Family Therapy forSerious Psychiatric Disorders10
Principles Guiding Implementation ofFamily Interventions in VAInterventions in the VA continuum of family services:1. Seek to identify and develop strengths andprotective factors, rather than focusing only onremediating weaknesses2. Involve professionals developing collaborativepartnerships with families, rather than institutinghierarchical relationships3. Explicitly acknowledge the importance of thenatural environment and context (in this case, thefamily) in influencing Veteran behaviorVETERANS HEALTH ADMINISTRATION11
Enhancing FamilyResilience within VAthrough PreventionProgramsVETERANS HEALTH ADMINISTRATION12
Understanding Family Resilience Psychological resiliency can be understood as the process ofmanaging successfully with adversity, resulting in positiveadaptation. . . resilience reflects the ability to maintain astable equilibrium in the context of significant stressors(Bonanno, 2004) The concept of personal resiliency has recently beenexpanded to include the notion of family resiliency (Palmer,2008)13VETERANS HEALTH ADMINISTRATION
Family Resilience in VA Moving Forward—Evidence-based problem-solving training(Nezu and Nezu)– disseminated as a resiliency program by mental healthprofessionals in primary care settings– Usually four manualized group sessions– Emphasis on OIF/OEF/OND Veterans though all cohorts canattend– Goal is to enhance effective problem-solving orientations andstrategies across a range of issues– In VA pilot, a fifth session (The Power of Two) in which familymembers learn to “coach” the Veteran to use the MovingForward strategies has been addedVETERANS HEALTH ADMINISTRATION14
Family EducationVETERANS HEALTH ADMINISTRATION15
Family Education/Training Family Education: A set of techniques that provide familieswith the information necessary to partner with thetreatment team and support Veterans’ recovery Topics include: Symptoms, Prognosis, Treatments, Identifyingand managing sources of stress and Factors associated withgood outcomes May be offered via written and video materials, one-dayworkshops, and/or regularly scheduled meetings conductedby professionals (e.g., the SAFE program or the NAMI Familyto Family program.)– Veterans may or may not be present for these trainingsVETERANS HEALTH ADMINISTRATION16
The Support And Family Education(SAFE) Program 18 session workshop for families of Veterans livingwith PTSD and/or serious mental illness Developed by Michelle Sherman Ph.D. at theOklahoma VA / VISN 16 MIRECC Families attend as many sessions as needed – eachsession can stand alone SAFE is not appropriate for– Dementia– Substance abuse as the primary problem areaVETERANS HEALTH ADMINISTRATION17
Workshop Content18 sessions – organized in four sections: Information about the Disorders– Example - PTSD and its impact on the family Skills for Family Members– Example - Problem-solving skills for families The Experience of Caring about Someone Living withSMI/PTSD– Example - Skills for managing stress effectively as a family member Dealing with Family, Friends and Professionals– Example - Coping with the stigma surrounding mental illnessVETERANS HEALTH ADMINISTRATION18
Operation Enduring FamiliesA five session family education and support program for Veteranswho have recently returned from a combat theatre and theirfamily members developed by Michelle Sherman and the ViSN 16MIRECC Session topics— Family Relationships— Communication and Intimacy— Anger— Posttraumatic Stress Disorder— DepressionVETERANS HEALTH ADMINISTRATION19
NAMI Family-To-Family EducationProgram (FFEP) Developed by National Alliance on Mental Illness 12 week program for family members of individualswith mental illness Taught by trained family members (i.e., peers) using ahighly structured/scripted manual Families receive information on mental illness,treatment, medications, recovery, communication andproblem-solving skillsVETERANS HEALTH ADMINISTRATION20
An Example: NAMI’s Family to FamilyApplications21
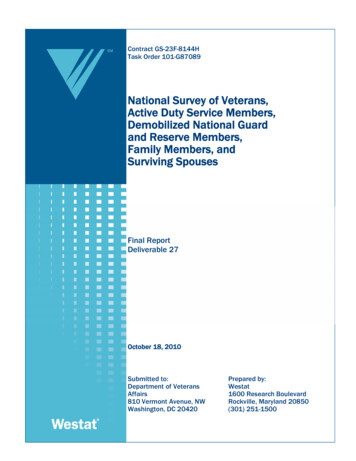
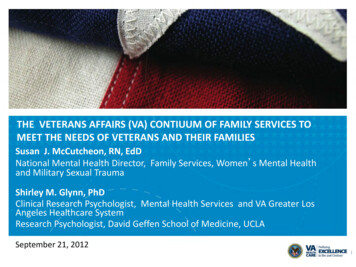
VHA-NAMI Memorandum ofUnderstanding Offer NAMI Family-to-Family Education Program (FFEP) in:- At least one VHA facility in each state- During a two year period June 2008 – June 2010 Collaborative effort between the VA and NAMI on national,state and local levels Developed second MOU to reinforce the inclusion of thispeer-led training into the continuum of VHA family servicesand serve as a model to continue the implementation of FFEPthroughout each state after the MOU three-year time period(December 2010 – December 2013) has expiredVETERANS HEALTH ADMINISTRATION22
Veteran Family Responses toFFEP “The course provided very essential informationabout mental illness not available anywhere else. Ifeel less guilty about what I have done to cause hisproblems. I better understand the illness” “I have benefited greatly by meeting otherparticipants of the class and listening to theirpersonal struggles. The sharing of information byclass participants provided some sense that I amnot alone and there is help available”VETERANS HEALTH ADMINISTRATION23
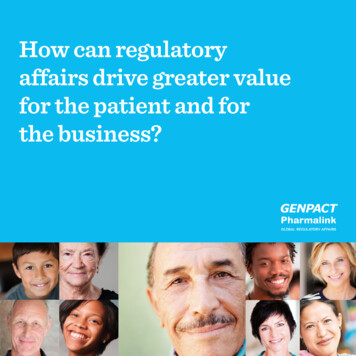
NAMI/VA FFEP Phase2NAMI/VAFFEP Phase 2Sites,by State - total113ParticipatingParticipatingSites,by State1Total : 113313111212222211412223226244332321Delaware: 1Washington, DC: 1Maryland: 1226Connecticut: 1Rhode Island: 1531 Massachusetts: 3223Hawaii: 113Puerto Rico: 124
Talk, Listen, Connect:Deployment, Homecoming, Changes Joint VHA, DoD, and SesameWorkshop bilingual educationaloutreach initiative designed forMilitary/Veteran families andtheir young children VA distributed 200,000 outreachkits to the VA Medical Centers andVet CentersVETERANS HEALTH ADMINISTRATION25
Talk, Listen, Connect: Deployment,Homecoming, ChangesToolkits include: Two Sesame Street DVDsMagazine for parents and caregiversChildren’s activity posterSesame postcardsSuggestions for further resourcesDownload materials, S HEALTH ADMINISTRATION26
Talk, Listen, Connect:Deployment, Homecoming, Changes“Changes “ - deals with sensitive subject ofan injured parent Rosita’s family adjust to the new realityof her father’s disability. Also includes footage of real life injuredfathers (amputations, head injury,depression) Parent should view DVD first Co-viewing is then recommended to talkabout “new ways to a new normal”VETERANS HEALTH ADMINISTRATION27
Veteran–Centered Brief FamilyConsultationVETERANS HEALTH ADMINISTRATION28
Family ConsultationVeteran-Centered Brief Family Consultation (VCBFC) Family meets with mental health professional asneeded to resolve specific issues related to theVeteran’s treatment and recovery Intervention is brief; typically one to five sessionsfor each consultation Provided on as needed or intermittent basis If more intensive ongoing effort is required, familycan be referred to Marriage and Family CounselingVETERANS HEALTH ADMINISTRATION29
Marriage and FamilyCounselingVETERANS HEALTH ADMINISTRATION30
Overview of Marriage and FamilyCounseling Program Roll-Out Program funded and supported by Mental Health Services at VACentral Office Part of effort to increase availability of psychosocial EBPs toVeterans Provides training, support, consultation to VA practitioners andMental Health leaders working with Veterans with relationshipdistress Current focus on Integrative Behavioral Couples Therapy (IBCT),Behavioral Couples Therapy for Substance Abuse Disorders(BCT), and Behavioral Family Therapy (BFT) for SeriousPsychiatric Disorders Will conduct pilot training in Cognitive-behavioral CouplesTreatment in PTSD in Feb, 2013VETERANS HEALTH ADMINISTRATION31
Description of Marriage andFamily Counseling ProgramsBeing DisseminatedNationally in VAVETERANS HEALTH ADMINISTRATION32
Integrative Behavioral Couples Therapy (IBCT;Jacobson and Christensen) Manualized intervention with strong supporting datafrom a large randomized trial Integrates goals of acceptance and change withbehavioral treatment strategies Overarching goals are to reduce couples distress andstrengthen family relationships Includes a four session assessment/feedback phaseand four to twelve session intervention phaseVETERANS HEALTH ADMINISTRATION33
Integrative Behavioral Couple Therapy (IBCT)Demographic Data on Training CasesDescriptionVeteran (Partner 1)Partner 2Number of Couples270270Age44.542.8Employed Full-Time (%)38.3%41.8%PTSD (%)50%5%Children living in the home (%)54.7%54.7%VETERANS HEALTH ADMINISTRATION34
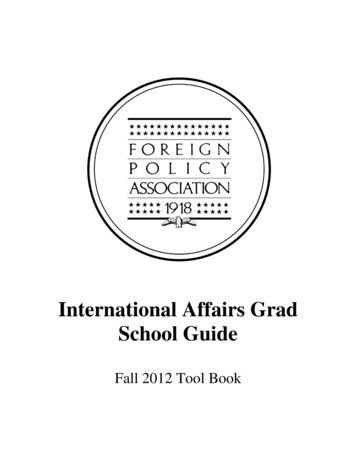
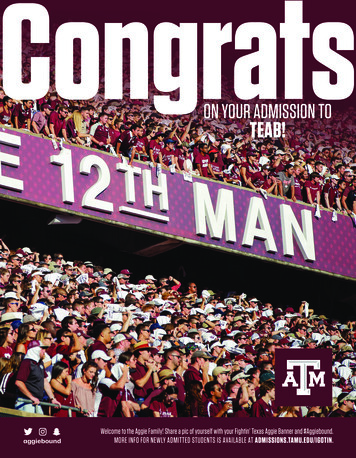
IBCT OutcomeCouple Satisfactory Index—4VETERANS HEALTH ADMINISTRATIONFirst session: n 236; Partner1 10.3; Partner2 8.87Last session: n 204; Partner1 12.03 ; Partner2 11.42Change differences are significant at .0135
Behavioral Couples Therapy for Substance UseDisorders (BCT; O’Farrell and Fals-Stewart) BCT goal is to support abstinence and improverelationship satisfaction BCT was designed for married or cohabitingpatients seeking help for substance abuse BCT sees patient with spouse or live-in partner for12-20 couple sessions over three to six months BCT fits well with self-help group BCT is a well-manualized intervention shown toreduce substance use in several controlled trialsVETERANS HEALTH ADMINISTRATION36
Parenting Issues Instruction Three hour presentation added to couples therapy training Readings, demonstrations, and lectures are used Goal is to assist VA clinicians, who may not have expertise inparenting issues, to become knowledgeable as a resource toVeterans parenting children Topics Covered:– Common parenting issues– Assessment, engaging parents, and red flags– Parenting fundamentals and child development– Resources and referralVETERANS HEALTH ADMINISTRATION37
Instruction on Addressing IntimatePersonal Violence (IPV) Veteran rates of IPV increase with co-occurringPTSD, SUD, and combat exposure (33% to 42%) Three hour training added to couples therapytraining to address IPV Readings, demonstrations, and lectures are used Goal is to help clinicians to recognize IPV and helpcouples address it while keeping them safeVETERANS HEALTH ADMINISTRATION38
Instruction on Addressing IntimatePersonal Violence (IPV) con’tTopics Covered in Training–Types of IPV, prevalence rates, and implications fortreatment–Assessment of IPV and determining appropriateness ofcouples therapy when a couple reports recent IPV–Use of safety planning strategies, appropriate referralsources, and documentation–Treatment considerations and general principlesVETERANS HEALTH ADMINISTRATION39
Family Psychoeducation (FPE) FPE: A collection of manualized interventions to equip familieswith the scoping skills and attitudes which have been shown toreduce relapse in serious psychiatric illnesses such asschizophrenia, severe depression, and bipolar illness (Fallon,Boyd, & McGill, 1984; Mueser & Glynn, 1999) Interventions share a number of components:– Careful assessment– Provision of education– Problem solving– Emphasis on improving current functioningVETERANS HEALTH ADMINISTRATION40
Family Psychoeducation (FPE)(cont) Relapse reductions associated with a minimum of ninemonths of intervention; most programs recommend one totwo years Treatment usually offered on a declining contact basis Veterans are typically present during FPE sessions. Can be offered to just one family (behavioral family therapy)or groups of families (multiple family group therapy)VETERANS HEALTH ADMINISTRATION41
Staff Training Overview and OutcomesStaff Training Overview andOutcomesVETERANS HEALTH ADMINISTRATION41
Marriage and Family CounselingStaff Training Program Goal is to assure a diverse group of mental health cliniciansgain expertise in helping relatives of Veterans Three to four day in-person experiential small workshop(around 30) with master trainers followed by 24 weeks ofsmall group weekly telephone consultation (may be extendeda few weeks for case finding) Program includes an evaluation– Veteran participant attendance– Veteran participant satisfaction– Veteran improvements in marital satisfaction– Veteran reductions in substance use (for BCT)VETERANS HEALTH ADMINISTRATION43
Marriage and Family Counseling andConsultation TrainingVA clinicians attending training workshops from FY 2007 – FY2012 Behavioral Family Therapy – 385Multiple Family Group Therapy –194Integrative Behavioral Couples Therapy –200Behavioral Couples Therapy for Substance Use Disorders-23Veteran-Centered Brief Family Consultation -441To support clinicians, also have a monthly advanced family topics calland an internal family services website to share informationVETERANS HEALTH ADMINISTRATION44
New Developments in VAFamily ServicesVETERANS HEALTH ADMINISTRATION44
Coaching Into Care Provides concerned family and friends with a place to calland get information about how to help loved ones— Targets Veterans reluctant to seek help, through theirconcerned family members— Goal is engagement in care which is often facilitated byfamily members– Optimize family involvement in getting Veteran into careby helping family members support Veteran in a positiveway— Coordinates with other VA telephone care linesVETERANS HEALTH ADMINISTRATION46
Coaching Into CareVETERANS HEALTH ADMINISTRATION47
Coaching Into CareCoaching involves:CoachingAvariableinvolves:number of telephone calls 25 min. eachProvidessupportivehelp A variablenumberof telephone calls 25 min.Informationeach and referralsOpportunities to problem solve Provides supportivehelpCommunicationrecommendations Information and referrals Opportunities to problem solve Communication recommendationsVETERANS HEALTH ADMINISTRATION48
Coaching Into Care - Statistics Since inception: 3508 calls (initial, follow-up, coaching),plus 1646 other actions (messages, inquiries toresources) Callers are Significant Others (26%), Self (Veteran)(23%), other family members (19%), parents (17%),friends (3%), other (12%); callers are 65% and Women,35% Men Most common issue concerns psychosocial issues(mental health, substance use problems) Outcomes: approximately 10% increase in Veteranmental health treatment engagement after workingwith callersVETERANS HEALTH ADMINISTRATION
New Initiatives for FY 2013 Small pilot of DoD Family Overcoming UnderStress (FOCUS) family resilience parentingprogram First staff training in Cognitive-behavioral CouplesTherapy for PTSD as part of the evidence-basedpsychotherapy dissemination program planned inFeb, 2013 Development of guidance and training on usingtelehealth in the provision of VA family serviceswork Production of video materials to use in stafftraining for engagement/family consultation andintegrative behavioral couples therapyVETERANS HEALTH ADMINISTRATION48
Thank you for your interest!QUESTIONS?susan.mccutcheon@va.gov51
Sep 21, 2012 · Current focus on Integrative Behavioral Couples Therapy (IBCT), Behavioral Couples Therapy for Substance Abuse Disorders (BCT), and Behavioral Family Therapy (BFT) for Serious Psychiatric Disorders Will conduct pilot training in Cognitive -behavi