Transcription
http://ebook2book.ir/
USMLE STEP 2 CK SURGERYLecture Noteshttp://ebook2book.ir/
2019http://ebook2book.ir/
Table of ContentsUSMLE Step 2 CK Lecture Notes 2018: SurgeryCoverTitle PageCopyrightEditorsFeedback PagePart I: SurgeryChapter 1: TraumaPrimary Survey: The ABCsA Review from Head to ToeBurnsBites and StingsChapter 2: OrthopedicsPediatric OrthopedicsAdult OrthopedicsTumorsChapter 3: Pre-Op and Post-Op CarePreoperative AssessmentPostoperative ComplicationsChapter 4: General SurgeryDiseases of the Gastrointestinal SystemDiseases of the BreastDiseases of the Endocrine SystemSurgical HypertensionChapter 5: Pediatric SurgeryBirth—First 24 HoursA Few Days Old—First 2 Months of LifeLater in InfancyChapter 6: Cardiothoracic SurgeryCongenital Heart ProblemsAcquired Heart DiseaseLungChapter 7: Vascular SurgeryChapter 8: Skin Surgeryhttp://ebook2book.ir/
Chapter 9: OphthalmologyChildrenAdultsChapter 10: Otolaryngology (ENT)Neck MassesOther TumorsPediatric ENTENT Emergencies and MiscellaneousChapter 11: NeurosurgeryDifferential Diagnosis Based on Patient HistoryVascular Occlusive DiseaseBrain TumorPain SyndromesChapter 12: UrologyUrologic EmergenciesCongenital Urologic DiseaseTumorsRetention and IncontinenceStonesMiscellaneousChapter 13: Organ TransplantationPart II: Surgical VignettesChapter 1: TraumaPrimary Survey: The ABCsA Review from Head to ToeBurnsBites and StingsChapter 2: OrthopedicsPediatric OrthopedicsAdult OrthopedicsTumorsChapter 3: Pre-Op and Post-Op CarePreoperative AssessmentPostoperative ComplicationsChapter 4: General SurgeryDiseases of the Gastrointestinal SystemDiseases of the BreastDiseases of the Endocrine SystemSurgical Hypertensionhttp://ebook2book.ir/
Chapter 5: Pediatric SurgeryAt Birth—The First 24 HoursA Few Days Old—The First 2 Months of LifeLater in InfancyChapter 6: Cardiothoracic SurgeryCongenital Heart ProblemsAcquired Heart DiseaseLungChapter 7: Vascular SurgeryChapter 8: Skin SurgeryChapter 9: OphthalmologyChildrenAdultsChapter 10: Otolaryngology (ENT)Neck MassesOther TumorsPediatric ENTENT Emergencies and MiscellaneousChapter 11: NeurosurgeryVascular Occlusive DiseaseBrain TumorSpinal CordPain SyndromesChapter 12: UrologyUrologic EmergenciesCongenital Urologic DiseaseTumorsRetention and IncontinenceStonesMiscellaneousChapter 13: Organ Transplantationhttp://ebook2book.ir/
USMLE is a joint program of the Federation of State Medical Boards (FSMB) and the National Board ofMedical Examiners (NBME), neither of which sponsors or endorses this product.This publication is designed to provide accurate information in regard to the subject matter covered as of itspublication date, with the understanding that knowledge and best practice constantly evolve. The publisheris not engaged in rendering medical, legal, accounting, or other professional service. If medical or legaladvice or other expert assistance is required, the services of a competent professional should be sought. Thispublication is not intended for use in clinical practice or the delivery of medical care. To the fullest extent ofthe law, neither the Publisher nor the Editors assume any liability for any injury and/or damage to personsor property arising out of or related to any use of the material contained in this book. 2018 by Kaplan, Inc.Published by Kaplan Medical, a division of Kaplan, Inc.750 Third AvenueNew York, NY 10017All rights reserved under International and Pan-American Copyright Conventions. By payment of therequired fees, you have been granted the non-exclusive, non-transferable right to access and read the text ofthis eBook on screen. No part of this text may be reproduced, transmitted, downloaded, decompiled, reverseengineered, or stored in or introduced into any information storage and retrieval system, in any form or byany means, whether electronic or mechanical, now known or hereinafter invented, without the expresswritten permission of the publisher.ISBN-13: 978-1-5062-3633-9http://ebook2book.ir/
EDITORSCarlos Pestana, MD, PhDEmeritus Professor of SurgeryUniversity of Texas Medical School at San AntonioSan Antonio, TXAdil Farooqui, MD, FRCSClinical Assistant Professor of SurgeryKeck School of Medicine, University of Southern CaliforniaKaiser Permanente, West Los Angeles Medical CenterLos Angeles, CAMark Nolan Hill, MD, FACSProfessor of SurgeryChicago Medical SchoolChicago, ILhttp://ebook2book.ir/
CONTRIBUTORTed A. James, MD, MS, FACSChief, Breast Surgical OncologyVice Chair, Academic AffairsDepartment of SurgeryBeth Israel Deaconess Medical CenterHarvard Medical SchoolBoston, MAThe editors would like to acknowledgeMichaela West, MD, PhD, FACS, North Memorial Health/University ofMinnesota and Gary Schwartz, MD, Baylor University Medical Center.http://ebook2book.ir/
We want to hear what you think. What do you like or not like about the Notes?Please email us at medfeedback@kaplan.com.http://ebook2book.ir/
Part Ihttp://ebook2book.ir/
SURGERYhttp://ebook2book.ir/
TRAUMAhttp://ebook2book.ir/
LEARNING OBJECTIVESDescribe the ABCs of evaluating a trauma patientDiscuss the importance of the Secondary Survey and a complete head-totoe review of a trauma patientProvide basic information about treatment of burns, bites, and stingshttp://ebook2book.ir/
PRIMARY SURVEY: THE ABCsThe initial evaluation of a trauma patient requires a systematic approach toidentify life threatening and potentially life-threating injuries. This typicallyinvolves a brief “Primary Survey” to assess airway (A), breathing (B),circulation (C), disability (D, neuro exam), and exposure (E) of the patient, sothat all potential injuries can be seen (ABCDE mnemonic). Needed interventionsshould be immediately addressed as the examiner proceeds through ABCDE.After the Primary Survey is complete, and if the patient is stable, then aSecondary Survey, involving a complete head to toe examination and evaluationof all organ systems should be performed.http://ebook2book.ir/
AIRWAY (A)The first step in the evaluation of trauma is airway assessment and protection.The airway is considered intact if the patient is conscious and speaking in anormal tone of voice.An airway is considered unprotected and/or compromised if there is anexpanding hematoma or subcutaneous emphysema in the neck, noisy or“gurgly” breathing, or a Glasgow Coma Scale 8.An airway should be secured before the situation becomes critical. In the fieldor in the ED, a definitive airway can be secured by intubation orcricothyroidotomy. Emergent airway control is best done by rapid sequenceinduction and orotracheal intubation, monitoring oxygen saturation with pulseoximetry. In the presence of a cervical spine injury, orotracheal intubation canstill be done if the head is secured and in-line stabilization is maintained duringthe procedure. If severe maxillofacial injuries preclude the use of intubation orintubation is unsuccessful, cricothyroidotomy may become necessary.In the pediatric patient population (age 8), tracheostomy is preferred overcricothyroidotomy due to the high risk of airway stenosis, as the cricoid is muchsmaller than in the adult.http://ebook2book.ir/
BREATHING (B)The presence of symmetrical breath sounds indicate satisfactory ventilation;an absence or decrease of breath sounds may indicate a pneumothorax and/orhemothorax and necessitate chest tube placement. Pulse oximetry can be used todetermine if oxygenation is satisfactory (O2 saturation 90-95%); hypoxiamay be secondary to airway compromise, pulmonary contusion, or neurologicalinjury impairing respiratory drive and necessitate intubation. Measurement ofend tidal CO2 (capnography) is also very useful.http://ebook2book.ir/
CIRCULATION (C) AND SHOCKClinical signs of shock are seen only if 25% of blood volume ( 1500-2000mL) has been lost and include the following:Low BP ( 90 mm Hg systolic)Tachycardia (heart rate 100 bpm)Low urinary output ( 0.5 ml/kg/h)Patients in shock will be pale, cold, shivering, sweating, thirsty, andapprehensive. In the most severe cases, impaired perfusion of the brain mayrender patients unconscious.In the trauma setting, shock is generally hypovolemic (secondary tohemorrhage and the most common scenario) or rarely cardiogenic (secondary topericardial tamponade or tension pneumothorax due to chest trauma).http://ebook2book.ir/
NOTEMany consider the chest x-ray and pelvis to be part of Primary Survey, along with FAST, lookingfor abdominal or pericardial fluid.Hemorrhagic shock is accompanied by collapsed neck veins due to low centralvenous pressure (CVP), while cardiogenic shock tends to cause elevated CVPwith jugular venous distention. Both processes may occur simultaneously, thatis, a patient could be hemorrhaging (hypovolemic) and have a tensionpneumothorax (with distended neck veins).In pericardial tamponade, there is shock without respiratory distress. Withtension pneumothorax, there is significant dyspnea, absent breath sounds andhyperresonance on the side of the tension pneumothorax, diminished breathsounds on the opposite side (due to mediastinal shift and compression of thelung), accompanied by, tracheal deviation.Treatment of hemorrhagic shock includes volume resuscitation and control ofbleeding, in the OR or ED depending on the injury and available resources.Volume resuscitation is initially with 2L of lactated Ringer’s solution unlessblood products are immediately available.In the setting of trauma, transfusion of blood products should be in a 1:1:1 ratiobetween packed RBCs, fresh frozen plasma, and platelets. Resuscitation shouldbe continued until BP and heart rate normalize and urine output reaches 0.5–1.0ml/kg/hr. In the setting of uncontrolled hemorrhage, permissive hypotension isrecommended to prevent further blood loss while awaiting definitive surgicalhttp://ebook2book.ir/
repair, but a mean arterial pressure 60 mm Hg should be maintained to ensureadequate cerebral perfusion.The preferred route of fluid resuscitation in the trauma setting is 2 large boreperipheral IV lines, 16-gauge or greater. If this cannot be obtained, percutaneousfemoral vein catheters should be inserted; saphenous vein cutdown andplacement of 1 intraosseous cannulas are acceptable alternatives. In childrenage 6, intraosseous cannulation of the proximal tibia or femur is the alternateroute.Pericardial tamponade is generally a clinical diagnosis that can be confirmedwith U/S. Management requires evacuation of the pericardial space bypericardiocentesis, subxiphoid pericardial window, or thoracotomy. Fluid andblood administration while evacuation is being set up is helpful to maintain anadequate cardiac output.Tension pneumothorax is a clinical diagnosis based on physical exam. Signsinclude absent breath sounds, tracheal deviation, “hyperresonance,” anddistended neck veins. May also be hypotension and shock. Management requiresimmediate decompression of the pleural space, initially with a large-bore needle(needle thoracostomy) which converts the tension to a simple pneumothorax andfollowed by chest tube placement.In the non-trauma setting, hypovolemic shock can also arise because ofmassive fluid loss such as bleeding, burns, peritonitis, pancreatitis, or massivediarrhea. The clinical picture is similar to trauma, with hypotension, tachycardia,and oliguria with a low CVP. Stop the bleeding and replace the blood volume.Non-traumatic (intrinsic) cardiogenic shock is caused by myocardial damage(e.g. myocardial infarction or fulminant myocarditis). The clinical picture ishttp://ebook2book.ir/
hypotension, tachycardia, and oliguria with a high CVP (presenting as distendedneck veins). Treat ment acutely consists of pharmacologic circulatory support,followed by attempts to restore perfusion and/or cardiac function. Differentialdiagnosis is essential, because additional fluid and blood administration in thissetting could be lethal, as the failing heart becomes easily overloaded.Neurogenic/spinal shock is often associated with low BP and bradycardia. It canalso result in circulatory collapse. Patients are flushed, “pink and warm” with alow CVP. Treatment with phenylephrine and fluids is aimed at filling dilatedveins and restoring peripheral resistance.http://ebook2book.ir/
DISABILITY (D)Neurologic evaluation (disability) is also an important component of the PrimarySurvey. Key points include assessing for the patient's ability to move allextremities, looking for gross defects. Level of consciousness, usually graded bythe Glasgow Coma Score (GCS) is also performed and documented.http://ebook2book.ir/
EXPOSURE (E)Staying aware of modesty at all times, remove the patient's clothing to allow fora thorough physical examination. Check for signs of trauma, bleeding, skinirritations, needle marks, and warm body temperature.http://ebook2book.ir/
SECONDARY SURVEYAfter the ABCs have been evaluated and any immediate life-threateningemergencies addressed, trauma evaluation continues with the secondary surveywhich is composed of a complete physical exam to evaluate for occult injuriesfollowed by chest x-ray and pelvic x-ray (although many include chest x-ray,pelvis x-ray, and FAST as part of the primary survey under “C,” to identifylocation of hemorrhage). The secondary survey may be augmented with furtherimaging studies depending on the mechanism of injury and findings onexamination. Any change that occurs requires complete re-evaluation, includingrechecking that there has not been a change in the ABCs.http://ebook2book.ir/
A REVIEW FROM HEAD TO TOEHEAD TRAUMAPenetrating head trauma as a rule requires surgical intervention and repair ofthe damage, although brain gunshot wound (especially transcranial gunshotwounds) are frequently lethal.Linear skull fractures are left alone if they are closed (no overlying wound).Open fractures require wound closure. If comminuted or depressed, treat inthe OR.The threshold for obtaining a brain CT should be very low. Almost anyonewho has lost consciousness or has GCS 13-14 should undergo CT imaging.Those with positive findings should get a neurosurgical consult, while thosewith normal findings who are neurologically intact (GCS 15) can beconsidered for discharge if they are able to be accompanied by family/friendsfor the next 24 hours.Basilar skull fractures can be difficult to diagnose. Signs of a fracture affectingthe base of the skull include raccoon eyes, rhinorrhea, otorrhea or ecchymosisbehind the ear (Battle’s sign). CT scan of the head is required to rule outintracranial bleeding and should be extended to include the neck (withreconstruction) to evaluate for a cervical spinal injury. Expectant management isthe rule and antibiotics are not usually indicated.Traumatic brain injury (TBI) from trauma can be caused by 3 components:Initial blow/direct injuryhttp://ebook2book.ir/
Intra-cranial bleeding resulting in a hematoma that displaces the brainstructures (e.g., compression of brain parenchyma, midline shift)Development of increased intracranial pressure (ICP) due to cerebral edemaThere is no treatment for the first (other than prevention), surgery can relieve thesecond, and medical measures can prevent or minimize the third.Acute epidural hematoma occurs with modest trauma to the side of the head,and has a classic sequence of trauma, unconsciousness, followed by a lucidinterval (a completely asymptomatic patient who returns to his previousactivity), gradual lapsing into coma again, fixed dilated pupil (90% of the timeon the side of the hematoma), and contralateral hemiparesis with decerebrateposturing. CT scan shows a biconvex, lens-shaped hematoma, typically in thefronto-temporal area. Emergency craniotomy produces a dramatic cure. Becausemost patients with a history of having been unconscious get a CT scan, the fullblown picture with a fixed pupil and contralateral hemiparesis is seldom seen.Acute subdural hematoma (SDH) also arises from a blow to the head, but theforce of the trauma is typically much larger and the patient is usually muchsicker (not fully awake and asymptomatic at any point), due to more severeneurologic damage. CT scan will show semilunar, crescent-shaped hematoma. Ifmidline structures are deviated, craniotomy to evacuate the blood is indicated,but the prognosis is frequently poor. If there is no deviation, therapy is centeredon preventing further damage from subsequent increased ICP.Invasive ICP monitoring, head elevation, modest hyperventilation, avoidance offluid overload, and diuretics such as mannitol or furosemide can decrease ICP.However, do not diurese to the point of lowering systemic arterial pressure, ascerebral perfusion pressure mean arterial pressure minus intracranialpressure. Hyperventilation is recommended when there are signs of herniation,http://ebook2book.ir/
and the goal is PCO2 35 mm Hg. Sedation is used to decrease brain activity andoxygen demand. Moderate hypothermia is currently recommended to furtherreduce cerebral oxygen demand.Diffuse axonal injury occurs in more severe trauma secondary to anoxia ordecreased cerebral perfusion. CT scan shows diffuse blurring of the gray-whitematter interface and multiple small punctate hemorrhages. Since there is not adiscrete hematoma, there is no role for surgery. Therapy is directed at preventingfurther damage from increased ICP.Chronic subdural hematoma (SDH) may be seen in the setting ofunrecognized subdural or expansion of acute SDH that was not drained. Chronicsubdural hematoma may develop from minor trauma, often in older individualswith underlying brain atrophy, from a tear of the venous sinuses. Over severaldays or weeks, mental function deteriorates as hematoma forms. Neurologicsymptoms may arise from a sub-clinical hematoma as the red blood cells lyseleading to osmotic expansion of the fluid collection. CT scan is diagnostic, andsurgical evacuation provides dramatic improvement.Hypovolemic shock cannot happen from intracranial bleeding: there isn’tenough space inside the head for the amount of blood loss needed to produceshock. Look for another source.http://ebook2book.ir/
NECK TRAUMAFor the purpose of evaluating penetrating neck trauma, the neck has beendivided into 3 zones.Zone 1 begins at the clavicles and extends to the level of the cricoid cartilageZone 2 is located between the cricoid cartilage and the angle of the mandibleZone 3 runs from the angle of the mandible to the base of the skullSurgical exploration for penetrating trauma to the neck is indicated in caseswhere there is an expanding hematoma, deteriorating vital signs, and signs ofesophageal or tracheal injury such as coughing or spitting up blood.For injuries to zone 1, evaluate with CTA and neck CT esophagogram (watersoluble, followed by barium if negative), esophagoscopy, and bronchoscopyto help decide if surgical exploration is indicated and to determine the idealsurgical approach.Historically, all penetrating injuries to zone 2 mandated surgical exploration,with a recent trend toward selective exploration based on physical exam andimaging studies.If the patient is stable with low index of suspicion of a significant injury,use CTA and neck CT to potentially avoid unnecessary surgicalexploration.If the patient’s condition changes or deteriorates urgent surgicalexploration is indicated.For injuries to zone 3, evaluate with CT angiography to identify any vascularinjury.http://ebook2book.ir/
In all patients with severe blunt trauma to the neck, the integrity of the cervicalspine has to be ascertained. Unconscious patients and conscious patients withmidline tenderness to palpation should be evaluated initially with CT scan,potentially followed with MRI depending on findings. Conscious patients withno symptoms (are not intoxicated, have not used drugs, or have no ‘distracting’injury) can be clinically evaluated for a cervical spinal injury; however if CTscan of the head is being obtained, it is generally accepted to extend the study toinclude the cervical spine.http://ebook2book.ir/
SPINAL CORD INJURYThe level and mechanism determine the impact of quality of life and thepotential for recovery. Transection of the spinal cord results in irreversiblecomplete loss of motor and sensory neurologic function below the level of theinjury. With high spinal cord injury, loss of sympathetic innervation and theresulting vasodilation (and in many cases, loss of sympathetic cardiac drive) canresult in neurogenic/spinal shock. Spinal shock should be considered in the acutetrauma setting if there is hypotension and paralysis, often accompanied bybradycardia.A few specific conditions related to spinal cord injury follow.Complete transection is unlikely to be on the exam because it is too easy:nothing works, sensory, or motor, below the level of the injury.Hemisection (Brown-Sequard) is typically caused by a clean-cut injury such asa knife blade, and results in ipsilateral paralysis and loss of proprioception alongwith contralateral loss of pain perception below the level of the injury.Anterior cord syndrome is typically seen with burst fractures of the vertebralbodies. There is loss of motor function, pain and temperature sensationbilaterally below the injury, but vibratory and positional sense are preserved.Central cord syndrome occurs in the elderly with forced hyperextension of theneck, such as a rear-end collision. There is paralysis and burning pain in theupper extremities, with preservation of most functions in the lower extremities.http://ebook2book.ir/
Management necessitates precise diagnosis of a cord injury, best done with MRI.There is some evidence that high-dose corticosteroids immediately after theinjury may help, but that concept is still controversial. Further surgicalmanagement is too specialized for the exam.http://ebook2book.ir/
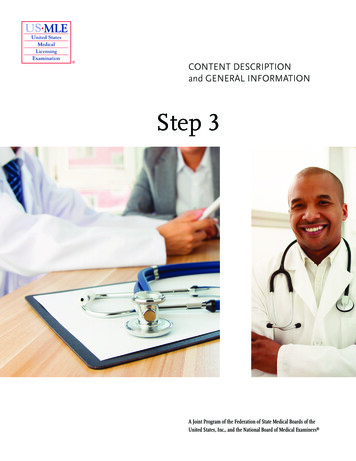
CHEST TRAUMARib fractures can be deadly in the elderly, because pain impairs respiratoryeffort, which leads to hypoventilation, atelectasis, and ultimately, pneumonia. Toavoid this cycle, treat pain from rib fractures with a local nerve block or epiduralcatheter, in addition to oral and IV analgesics.http://ebook2book.ir/
Figure I-1-1. X-ray of Multiple Rib Fractures due to TraumaCopyright 2007 Shout Pictures - Custom Medical Stock Photo. All rights reserved.Simple pneumothorax results from collapse of the lung. Mechanisms includepenetrating injury, rib fracture with puncture of lung, and secondary iatrogeniccauses (e.g., CVC placement). There is typically moderate shortness of breathwith absence of unilateral breath sounds and hyperresonance to percussion.Diagnosis is confirmed with chest x-ray, and management consists of chest tubeplacement.Hemothorax occurs when blunt or penetrating injury results in bleeding into thechest cavity. The blood can originate directly from the lung parenchyma or fromthe chest wall, such as an intercostal artery. Physical examination revealsdecreased breath sounds on the affected side, accompanied by dullness topercussion. Diagnosis is confirmed with chest x-ray. Chest tube placement isnecessary to enable evacuation of the accumulated blood to prevent latedevelopment of a fibrothorax or empyema, but surgery to stop the bleeding issometimes required. If the lung is the source of bleeding, it usually stopsspontaneously as it is a low pressure system.In some cases where a systemic vessel such as an intercostal artery is the sourceof bleeding, thoracotomy is needed to stop the hemorrhage. Indications forthoracotomy include:Evacuation of 1,500 mL when the chest tube is insertedCollecting drainage of 1 L of blood over 4 hours, i.e., 200mL/hrhttp://ebook2book.ir/
Severe blunt trauma to the chest may cause obvious injuries such as ribfractures with a flail chest or sucking chest wound, as well as less apparentinjuries such as pulmonary contusion, blunt cardiac injury, diaphragmatic injury,and aortic injury.Sucking chest wounds are obvious from physical exam. If there is a flap thatsucks air with inspiration and closes during expiration it could lead to a tensionpneumothorax. A sucking chest wound can also arise from an openpneumothorax, where a larger open wound leads to the inability to exchange airon the side of the injury. Initial management is with a partially occlusivedressing secured on 3 sides, with one open side acting as a one-way valve. Thisallows air to escape but not to enter the pleural cavity (to prevent iatrogenictension pneumothorax).Flail chest involves fracture 3 ribs with 2 segments broken. This allows asegment of the chest wall to retract during inspiration and bulge out duringexpiration (so-called, “paradoxical breathing”). The real problem is theunderlying pulmonary contusion. A contused lung is very sensitive to fluidoverload, thus treatment includes fluid restriction and aggressive painmanagement. Pulmonary dysfunction may develop, thus serial chest x-rays andarterial blood gases have to be monitored.Pulmonary contusion may be detected immediately after chest trauma with“white-out” of the affected lung(s) or can be delayed up to 48 hours. Significantforce is necessary to result in a flail chest, so traumatic dissection or transectionof the aorta should be evaluated for using a CT angiogram. Finally, ARDS maydevelop in this scenario.Blunt cardiac injury should be suspected with the presence of sternal fractures.ECG monitoring will detect any abnormalities. Although serum troponin levelhttp://ebook2book.ir/
was historically obtained, elevations do not generally change management andare therefore not indicated, and treatment is focused on the complications of theinjury such as arrhythmias.Traumatic rupture of the diaphragm shows up with the bowel in the chest (byphysical exam and x-rays), almost always on the left side (the liver protects theright hemidiaphragm). If diaphragmatic injury is suspected it should beevaluated with laparoscopy, although gas insufflation of the peritoneum maycomplicate anesthetic care. Surgical repair is typically done from the abdomen.Traumatic rupture of the aorta is the ultimate “hidden injury.” It mostcommonly occurs at the junction of the arch and the descending aorta where therelatively mobile aorta is tethered by the ligamentum arteriosum. Such an injurycan occur in the setting of a significant deceleration injury and may be totallyasymptomatic until the hematoma contained by the adventitia ruptures resultingin rapid death. Aortic injury should be suspected if:Mechanism of injury, high energy deceleration mechanismWidened mediastinum on chest x-ray or mediastinal hematoma on chest CTPresence of atypical fractures such as the first or second rib, scapula, orsternum, all of which require great force to fractureDiagnosis is made with CT angiogram. Surgical repair is indicated once thepatient has been stabilized and more immediate live-threatening injuries havebeen managed. Repair of aortic injury can be done in an open or endovascularfashion.Traumatic rupture of the trachea or major bronchus is suggested by thepresence of subcutaneous emphysema in the upper chest and lower neck, or by alarge “air leak” from a chest tube. Chest x-ray and CT scan confirm the presencehttp://ebook2book.ir/
of air outside the bronchopulmonary tree, and fiberoptic bronchoscopy mayidentify the injury and allow intubation past the injury to secure an airway.Surgical repair is indicated.Differential diagnosis of subcutaneous emphysema also includes rupture of theesophagus and tension pneumothorax.Air embolism can produce sudden cardiovascular collapse and cardiac arrest. Itshould be suspected when sudden death occurs in a chest trauma patient who isintubated and on a respirator. It also can occur in a spontaneously breathingpatient if the subclavian vein is opened to the air (e.g. supraclavicular nodebiopsies, central venous line placement or lines that becomedisconnected). Immediate management includes cardiac massage, with thepatient positioned in Trendelenburg with the left side down to “trap” air in theatria until it can be absorbed or aspirated. Prevention of air embolism includesuse of the Trendelenburg position when the great veins at the base of the neckare to be accessed.Fat embolism may also produce respiratory distress in a trauma patient who iswithout direct chest trauma. The typical setting is the following:Patient with multiple traumatic injuries (including several long bonefractures) develops petechial rashes in the axillae and neck; fever,tachycardia, and low platelet countAt some point patient develops a full-blown picture of respiratory distress,with hypoxemia and bilateral patchy infiltrates on chest x-rayThe mainstay of therapy for fat embolism is respiratory support. Other therapiesfor this syndrome including heparin, steroids, alcohol, or low-molecular-weightdextran have been discredited.http://ebook2book.ir/
ABDOMINAL TRAUMAFor the sake of evaluation and management, abdominal trauma is divided intopenetrating and blunt trauma based on the mechanism of injury. Penetratingtrauma is further differentiated into gunshot wounds and stab wounds as thepattern of injury based on mechanism is quite different.Gunshot wounds to the abdomen require exploratory laparotomy forevaluation and possible repair of intra-abdominal injuries, not to “remove thebullet.” Any entrance or exit wound below the level of the nipple line isconsidered to involve the abdomen.Stab wounds allow a more individualized approach. “Selective management”with close observation of hemodynamically stable patients can avoid nontherapeutic laparotomy. However, the presence of protruding viscera or thedevelopment of peritoneal signs/evidence of ongoing bleeding requiresexploratory laparotomy.In the absence of the conditions above, local wound exploration may beperformed in the ED to assess whether or not the anterior rectus fascia has beenpenetrated.If the fascia is not violated, the intra-abdominal cavity likely has
USMLE is a joint program of the Federation of State Medical Boards (FSMB) and the National Board of Medical Examiners (NBME), neither of which sponsors or endorses this product. This