Transcription
INTRODUCTION TOCOGNITIVENEUROPSYCHOLOGYRaffaella Ida RumiatiCognitive Neuroscience SectorScuola Internazionale Superiore diStudi AvanzatiTrieste, Italy
WHAT IS NEUROPSYCHOLOGY? Neuropsychology is the study of the effectsof lesions or dysfunctions of the CentralNervous System (CNS) on cognition andbehaviour. The regions of interest are the cortex of thetwo brain hemispheres, the sub-corticalstructures (such as thalamus, basalganglia, hypothalamus, and amygdala) andthe main connecting white matter fibres.
THE AIMS OF NP Neuropsychology is useful for bothresearch and clinical purposes:1. It explores the functional architecture of themind and its neural correlates;2. It provides patients with a diagnosis andpossibly with rehabilitative recommendations. No research is possible without a clearunderstanding of the nature of the deficit.
LOCALIZATION The history of neuropsychology is linked to thechanging of concepts of functions’ localization. By localization we mean that different parts of thebrain are specialized in such a way so as tocontribute to behaviour at various levels. The most fundamental fact was established inancient times when the Greeks first determinedthat the brain was the physical seat of the mind. The one credited with making this basic advancein the V century B.C. is Alcmaeon of Croton, whocame to this conclusion after observing braindamaged patients.
THE CARDIOCENTRIC VIEW The alternative hypothesis held the heart to bethe organ responsible for sensation andthought. This was the accepted view among ancientEgyptian writers and continued to attractadherents in ancient Greece. Among them, Aristotle (ca 384-322 BC)maintained the cardiocentric view, andsuggested that the brain served to cool theblood.
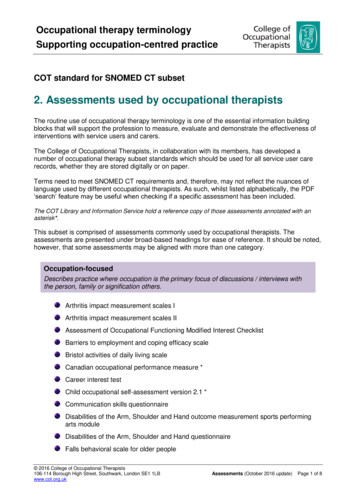
THE THEORY OF THE VENTRICLES Among cerebrocentrics, however, thenature of the mind-brain relation waspoorly understood. In fact, for centuries, the most importantanatomical features of the brain wereconsidered to be the ventricles. Why ventricles? Because they containedthe real substance of the mind, i.e. thecerebrospinal fluid.
VENTRICLES2: 3rd ventricle3: 4th ventricle164: Monro’s foramen5: aqueduct6-9: lateral ventricles (1-2)15: Luschka’s foramen & (16) Magendie’s foramen
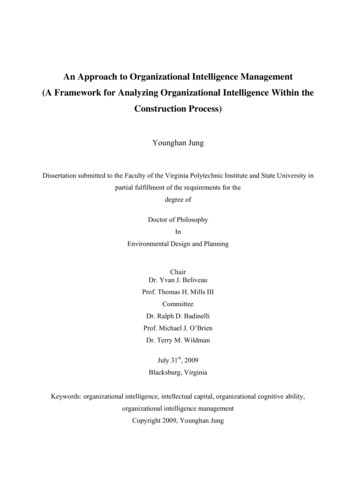
LOCALIZATION AND THE VENTRICLESHerophilus of Alexandria (ca 335-280 BC) placed the mind in the posterior (fourth) ventricle.Galen (130-200 AD) distinguished three basic components of the intellect:imagination, reason and memory. Although he thought that each function could be affectedseparately by brain damage, he did not propose to localizethem within the ventricular system.Nemesius Bishop of Emesia (ca. 390 AD) proposed that perception imagination were localized inthe 2 lateral ventricles (treated as a single, anterior cavity); reason in the middle ventricle (3 ); memory in the most posterior ventricle (4 ).
2nd VentricleReason3rd Ventricle1st VentricleMemoryPerceptionImaginationAlbertus Magnus, Philosophia naturalis, 1506
DECLINE OF THE THEORY OF THE VENTRICLES After many centuries, the ventricular doctrine slowlystarted to decline and the forebrain began its rise toprominence as the source of things intellectual.WHITE MATTER After the XVI century, it was accepted that theencephalon was the site of mental functions but thecritical structure was held to be the white matter,whereas the gray matter was considered as theexternal, protecting layer. Schenck (XVI) Wepfer (1727, book published posthumously)
RISE OF THE THEORY OF PHRENOLOGYFRANZ JOSEPH GALL (1757-1828) He proposed an explicit theory of the mind-brainrelationship whose main ideas are:– the mind is made up of 27 distinctive components(faculties)– these are localized in specific regions (organs) ofthe cerebral cortex– the amount of a given faculty determines the size ofthe organ: the more highly a faculty is developed,the larger the organ.– by measuring the skull of an individual, one caninfer the dimension of single faculties.
The theory of phrenology was dismissedbecause it could not be proved scientifically:– too many faculties which were non-cognitive– impossible to find their localization. Although the method employed by Gall was farfrom being satisfactory, the theory had the meritof drawing the attention to the correlationbetween the cortex (i.e. grey matter) andcognitive functions. Importantly, Gall and his followers wereconvinced that speech was housed in the frontpart of the cerebral cortex.
IS LANGUAGE IN THE FRONTAL LOBES?JEAN-BAPTISTE BOUILLAUD (1796-1881) examined a large number of patients with braindamage and language disorders (collected byothers); confirmed the localization of speech in the frontalcortex, without distinguishing between left andright hemisphere, in all the cases considered. However Luzzatti & Whitaker (2001) demonstratedthat Bouillaud’s localization was inconsistent withthe observation of many patients with injuries tothe frontal lobes without aphasia (and patients withaphasia without frontal lesions).
IS THE LEFT HEMISPHERESPECIALIZED FOR LANGUAGE?Marc Dax (1770-1837) In 1836, he presented at a conference ofmedicine in Montpellier, more than 40cases of patients with left-hemispherelesions and aphasia, suggesting thatlanguage is a lateralized function. Dax’s report was published by his sononly in 1865, after his death.
PAUL BROCA In 1861, he presented hiscelebrated case ofMonsieur Leborgne,nicknamed “Tan”because this was his onlyutterance, along with afew obscenities. This 51-yr-old man was along-term resident in aninstitution, who had losthis capacity for voluntarylanguage 21 yrs. earlier,and had not been able touse his right arm for 10yrs.
Tan died soon after Broca saw him and his autopsy revealeda lesion centered in the foot of the third frontal convolution ofthe left hemisphere.“Tan’s” brain,now at theMusèeDupuytren In 1865, Broca suggested that language was afunction lateralized in the left hemisphere.
WernickeHe proposed ageneral model(1874) of languagethat could explain anumber of differentaphasic syndromesby means of lesionsto different centersand connections tocenters.Unlike Gall’s model, a relativelysmall number of basic centersand connections allow one toexplain a wide variety of higherfunctions.
Localizing motor functions Fritsch & Hitzig (1870) found that,depending on what part of thedog’s cortex they stimulatedelectrically, a different part of thebody contracted. They also found that if theydestroyed this same small area ofthe cortex, the corresponding partof the body became paralyzed. They thus established that everypart of the body has a particularregion of the primary motor cortexthat controls its movement. Body parts that can make thefinest movements take up muchmore space than others (Penfield,in man).
David Ferrier (1843-1928)performed electric stimulationon the monkey brain.
APRAXIA: LIEPMANN (1920)1. Motor Apraxia2. IdeomotorApraxia3. IdeationalApraxia
PSYCHIC BLINDNESS Munk ablated bilaterally the occipital lobesof dogs and monkeys (1878, 1881). The ablation produced an impairment ofthe animals’ ability to recognize objects,although they were still able to navigate inthe environment. These findings established an associationbetween vision and occipital cortex.
Seelenblindheit or Soul-blindness Lissauer (1890) described the case of apatient with a lesion of the left temporooccipital junction, who was not able to identifyfamiliar objects though he could copydrawings and was not confused. He suggested a distinction between anapperceptive and an associative deficit, aclinical dichotomy still in use today. The term agnosia was introduced by SigmundFreud (1891).
THE RIGHT HEMISPHERE The first to recognize that the righthemisphere might have specializedfunctions of its own was Hughlings Jackson(1876). Based on the clinical observation of a singlepatient, he argued that whilst the lefthemisphere might be “dominant” forlanguage, the right hemisphere was criticalfor visuo-perceptual abilities.
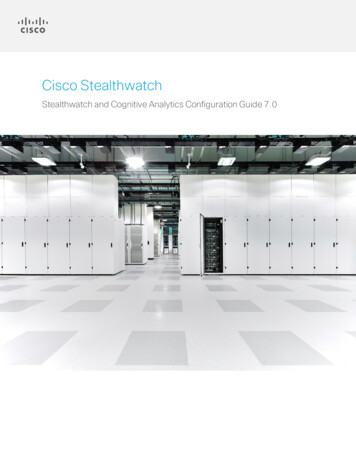
INTELLECT & FRONTAL LOBES Damage to prefrontal cortex leads to more complexphenomena. The first description of the consequences of lesion tothese regions in man is that of Phineas Gage, givenby Harlow in 1848. Gage was a rail-road foreman who accidentallydropped his tamping iron on a rock, igniting someblasting powder. The explosion caused the iron to shoot through the leftside of Gage’s jaw and up through the front of hiscranium.
Harlow (1868)
CLINICAL REMARKS“He was no longer Gage” Gage’s recovery over the next few monthsafter the accident was far better than anyoneexpected. However, it was clear that his personality andintellect had been altered:– he now exhibited poor judgment, impulsivity, andlack of restraint;– he had become childish. This was the beginning of the associationbetween frontal lobes and more abstractintellectual functions.
LIMITS OF TRADITIONAL NP With a few exceptions, individual patientswere poorly described. They often suffered from multiple deficits. Patients were grouped into syndromesbecause they shared symptoms (patientswith Broca’s aphasia, Wernicke’s aphasia,etc.). The psychological concepts and testsavailable were inadequate. The techniques were too few.
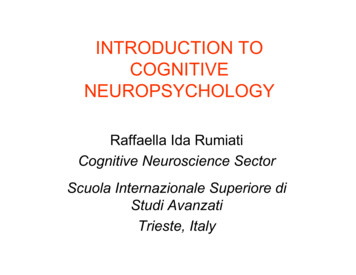
DIAGRAMS Traditional neuropsychologists made agreat use of diagrams between 1870 and1910. These diagrams were used to explaindifferent forms of language disorder in termsof damage either to the centres themselvesor to the pathways connecting them. The best known is that put forward byLichtheim (1885).
Lichtheim’s ModelA centre of auditoryrepresentations of wordsCB centre of auditoryrepresentations of wordsOa auditory analysisb articulatory programmingC conceptual knowledgeO visual engrams (reading)E hand motor engrams (spelling)EBAba
LIMITS OF DIAGRAMS They were only of real use in interpreting disordersthat affected comprehension, production, repetitionof single words. They had little to say about:–disorders affecting, for example, grammatical processesinvolved in sentence construction;–or about how the centres might actually work. They were constrained only by neuropsychologicalevidence and often changed to fit new patterns. Diagrams were super-imposed upon the leftcerebral hemisphere of the brain:–they incorporated both a cognitive theory of what centresand connections are, and where they were located.
COGNITIVE NEUROPSYCHOLOGY A revolution occurred when patient-basedneuropsychology and cognitive psychologyeventually came together. The main tenet of cognitive psychology is thatmental activity (i.e. cognition) is informationprocessing. By varying stimuli and instructions to thesubjects, and by measuring their responses,cognitive psychologists make inferencesabout the information processing thatintervenes between stimulus and response(the black box).
COGNITIVENEUROPSYCHOLOGISTS seek to explain the patterns of impaired andintact cognitive performance seen in braininjured patients in terms of damage to one ormore of the components of a theory of normalcognitive functioning and, on the other hand, to draw conclusionsabout normal, intact cognitive processes fromobserved disorders.
the main connecting white matter fibres. . –the mind is made up of 27distinctive components (faculties ) . neuropsychologyand cognitive psychology eventually came together. The main tenet of cognitive psychology