Transcription
THE THERAPEUTIC CRISIS INTERVENTION SYSTEM, EDITION 7RESIDENTIAL CHILD CARE PROJECT BRONFENBRENNER CENTER FOR TRANSLATIONAL RESEARCH CORNELL UNIVERSITY
Therapeutic Crisis Intervention System, Edition 7Information BulletinResidential Child Care ProjectBronfenbrenner Center for Translational ResearchCollege of Human EcologyCornell University, Ithaca, NY USA Residential Child Care Project, 2021
Dear Colleague,Enclosed you will find information about our Therapeutic Crisis Intervention (TCI) system. Ourgoal is to research, develop, disseminate, and evaluate model techniques to improve the quality ofcare for children in out-of-home care. In addition, the TCI system is designed to help organizations prevent child retraumatization and injury by reducing the need for physical restraint.In 2020, we launched the 7th edition of our TCI system, celebrating 40 years of supporting residential organizations in their efforts to provide safe and quality care for children and young people.When implemented with fidelity, TCI has resulted in an increased ability on the part of staff tomanage and prevent crises. Implementation studies have also shown an increased knowledge andskill on the part of all staff to handle crisis episodes effectively and a change in attitude regardingthe use of physical restraint. If TCI is to be an effective crisis management system for your organization, you need to address six general criteria: (a) leadership and program support, (b) child andfamily inclusion, (c) clinical participation, (d) supervision and post crisis response, (e) training andcompetency standards, and (f) critical incident monitoring and feedback The description of thesecriteria and the TCI Theory of Change begins on page 17 of this brochure to help you decidewhether TCI is right for your organization.The Residential Child Care Project supports vigorous and ongoing in-house evaluation of TCItraining and implementation efforts through testing participants’ knowledge and skills, offeringa trainer certification program, conducting agency TCI quality improvement and fidelity assessments, and establishing a TCI agency registration process designed to formally recognize organizations that have implemented the TCI system at the highest standard.The RCCP seeks to maintaina leadership role in discovering new knowledge, establishing new approaches to knowledge dissemination, and developing innovative programs to enable child caring agencies to serve childrenand families more effectively by building strong linkages among research, outreach activities, andevaluation efforts.If you need any other additional information, please contact us at: Andrea Turnbull atajt78@cornell.eduSincerely,Martha J. HoldenDirector, Residential Child Care Project
ContentsPrefacePreface2Research Foundations of TCITCI Implementation Study8Learning From Tragedy: The Results of a National Study of Fatalities inOut-of-Home Care14TCI System Implementation18Implementation Criteria18The Therapeutic Crisis Intervention System: A Trauma-Informed Approach18The TCI System: The Six Domains21Questions for Implementation Assessment30Leadership and Program Support33Services Offered33Model Policy on the Use of Physical Intervention34Clinical Participation37Services Offered37Supervision and Post-Crisis Support39Services Offered39Training and Competency Standards41Services Offered41TCI Trainer Certification Process42Agenda: TCI Training of Trainers43Documentation, Incident Monitoring, and Feedback45Bibliography47TCI Faculty, Instructors, and Staff57THERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University1
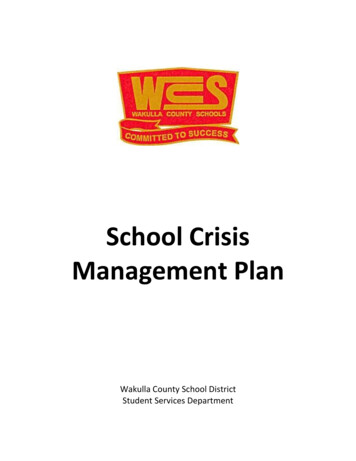
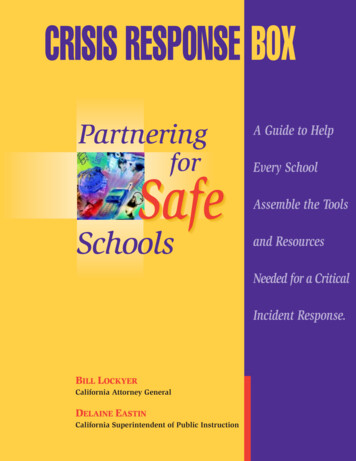
PrefacePrefaceThe Bronfenbrenner Center forTranslational ResearchThe Bronfenbrenner Center for TranslationalResearch, located within Cornell University’sCollege of Human Ecology, administers the Residential Child Care Project (RCCP).The BCTR’sorigins date to 1974, when its parent organization,the Family Life Development Center (FLDC),was established by New York State legislationunder the leadership of John Doris, professor ofhuman development in the College of HumanEcology at Cornell. FLDC’s mission was to studyand develop programs to prevent child abuse.On July 1, 2011, FLDC merged with the Bronfenbrenner Life Course Center to create theBronfenbrenner Center for Translational Research (BCTR). The BCTR is named after UrieBronfenbrenner, an American psychologist whois most known for his ecological systems theorythat called attention to the large number of environmental and societal influences on child development. A Cornell alumnus and Cornell professor, Urie Bronfenbrenner helped form the HeadStart Program in the United States in 1965.The BCTR’s mission is to improve professionaland public efforts to understand and deal withrisk and protective factors in the lives of children,youth, families, and communities that affect family strength, child wellbeing, and youth development. Translational research, as defined by theCollege and the BCTR, is the systematic application of research findings to the development ofinnovative interventions, practices, and policiesthat may ultimately improve health and wellbeing. Conversely, the use of knowledge derivedfrom interventions, practices, and policies helps toinform future research.Steve Hamilton, a faculty member of the BCTR,introduced a new model of translational researchWhat makesyouth tick?What’s happening? Demography Epidemiology Observation Basic ResearchPRACTICEHow do we usewhat works? DiffusionDisseminationScaling UpAdaptationWhat works? ntFigure 1. Hamilton Model of Translational Research for Youth Development2THERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University
Prefacefor his work in youth development.Hamilton’sMajor Programs of The Residential Child Care Projectmodel of translational research (Figure 1)1 includes Therapeutic Crisis Intervention (TCI) Systemfour quadrants, each witha different focus.2 Each Children and Residential Experiences (CARE): Creatingquadrant is differentiatedConditions for Changeby the types of questionsand the types of researchThe RCCP has delivered programs and consultation servicesmethods most commonlythroughout the United States, Canada, Puerto Rico, Russia,employed. Most imporIsrael, Australia, South Korea, Ireland, Bermuda, and the Unitedtantly, practice is deliberately placed in the centerKingdom. Used in hundreds of residential child care agencies,of the model with bi-diTCI has also been adapted for other residential care settingsrectional arrows between(e.g., mental health, juvenile justice) as well as foster, kinship,practice and each quadand adoptive families (TCIF) and for schools (TCIS).rant. Practice can informor inspire research andpractice can benefit fromresearch in any quadrant.A Center for Creating Trauma-InformedThe emphasis on evidence-based practices andtranslational research in human services, espe- Residential Settingscially Hamilton’s model, has the potential to havea significant and positive impact on therapeutic In 2018, the Residential Child Care Projectresidential services and all the organizations that (RCCP) received a grant from the U.S. Departserve the best interests of children and their fami- ment of Health and Human Services to establishthe Center for Creating Trauma-Informed Resilies.dential Settings. The grant is part of the NationalSince 1980 the Residential Child Care Project Child Traumatic Stress Network, a federal efforthas developed, evaluated, and disseminated two to develop a national network of services formajor programs: Therapeutic Crisis Intervention children and adolescents who have experienced(TCI) and Children and Residential Experiences: trauma. The goal of the grant is to share research,Creating Conditions for Change (CARE). Both strategies, and learning to assist residential setprograms have sought to translate the latest re- tings to use trauma-informed and evidence-basedsearch into practice and to increase the knowl- models and to share the RCCP’s Therapeuticedge and expertise of personnel at all levels of Crisis Intervention (TCI) system and Childrenchild serving organizations. The RCCP’s intent and Residential Experiences (CARE): Creatingfor both programs is to promote more positive Conditions for Change program model with resioutcomes for children, families, and staff with a dential care centers across the USA.special emphasis on developing healthy relationships and safer environments.THERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University3
PrefaceChildren and Residential Experiences and Neglect, began disseminating TCI to residen(CARE): Creating Conditions for Change tial child care organizations throughout the USA.The TCI system assists organizations in preventing crises from occurring, de-escalating potentialCARE is a multi-level program model for imcrises, managing acute physical behavior, reducingproving services for children in out-of-home care.potential and actual injury to children and staff,CARE is listed on the California Evidence Basedteaching children adaptive coping strategies, andClearinghouse (CEBC) as of 2017 with a Sciendeveloping a learning organization. This modeltific Rating of 3 (Promising Research Evidence)gives organizations a framework for implementand a High Child Welfare System Relevanceing a crisis prevention and management systemRating.3 The CARE program model is built onthat reduces the need to rely on high-risk intersix principles that form the foundation for creventions.ating conditions for change in residential care.CARE is: (a) developmentally focused, (b) familyTCI addresses six general domains:involved, (c) relationship based, (d) competencecentered, (e) trauma informed, and (f) ecologi- 1. Leadership and program supportcally oriented. These principles have a strong re2. Child and family inclusionsearch and/or theoretical relationship to positivechild outcomes, and can be incorporated into a 3. Clinical participationwide variety of programs and treatment models. 4. Supervision and post-crisis responseCARE enables child caring agencies to orga5. Training and competency standardsnize and deliver quality care of children according to research-informed principles based on the 6. Documentation, incident monitoring, andfeedbackbest interest of the child. The aim of CARE is tobring agencies’ current practices closer to wellThese domains are required to establish effectiveresearched best practices in residential care and tocrisis prevention and management in a residentialhelp them achieve congruence among all levelssetting.These six domains are congruent with theof the organization in order to improve how thesix core strategies outlined by the National Asagency works as a whole.sociation of State Mental Health Program Directors4 and the Child Welfare League of America.5The Therapeutic Crisis InterventionSystemTherapeutic Crisis Intervention (TCI), a traumainformed crisis prevention and management system first developed in the early 1980’s for NewYork State’s voluntary child care agencies, incorporates findings from the social science literatureand is implemented through research informedstrategies such as organizational assessment, activeand targeted data analysis, training, and technicalassistance. Also, in the 1980s, the RCCP, under agrant from the National Center on Child Abuse4Many children who have experienced toxic stressand trauma have never learned effective emotional regulation skills and constructive ways of coping with or responding to internal or interpersonal stress, upset, or pain. The skills necessary toimplement TCI are neither intuitive nor natural;staff must be fully trained and supervised in coregulation skills and strategies that are based onself-awareness, active listening, behavior supporttechniques, emotional first aid, crisis co-regulation, and the Life Space Interview.Since the curriculum’s inception there have beenTHERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University
Prefacesix major revisions. The revision process generallyincludes (a) examining the evaluation results andresearch conducted by the RCCP, (b) reviewingrelated literature and research, (c) conducting surveys of organizations using the TCI system, and(d) convening experts for consultation and review. TCI has been disseminated successfully forfour decades and is now operating in more than1,800 residential child care agencies, foster caresettings, juvenile justice programs, hospitals, andschools across the U.S. and internationally.The RCCP supports vigorous and ongoing inhouse evaluation of TCI training and implementation efforts through testing participants’knowledge and skills, offering a trainer certification program, conducting agency TCI quality improvement and fidelity assessments, and establishing a TCI agency registration process designed toformally recognize organizations that have implemented the TCI system at the highest standard.The RCCP seeks to maintain a leadership rolein discovering new knowledge, establishing newapproaches to knowledge dissemination, and developing innovative programs to enable child caring agencies to serve children and families moreeffectively by building strong linkages among research, outreach activities, and evaluation efforts.Past and Present ContributorsThe TCI curriculum was first developed in 1980by Michael J. Budlong and Andrea J. Mooney.Over the years, the TCI system and curriculumhave been reviewed and revised with the assistance and support of many organizations andindividuals. The Residential Child Care Projectand the BCTR at Cornell University wish tothank the following people and organizations fortheir contributions, service, advice, and professional commitment to the project:The Seventh EditionCraig Bailey, Manager, Organization Development and Learning, Hillside Family of Agencies,Rochester NYJohn Gibson, Doc. P.W., Owner, Secure Attachment Matters, IrelandNicola Jackson MCSP, MHCPC, OccupationalHealth Physiotherapist, UKBen Jones, Training and Development Coordinator, TACT, AustraliaMichael Nunno, DSW, Senior Extension Associate, Bronfenbrenner Center for Translational Research, Ithaca NYNick Pidgeon, Director, NJP Consultancy &Training, LTD Consulting, Bridge of Allan, ScotlandSusan Sullivan, RN, Medical Program Director,Waterford Country School, Waterford, CTZelma Smith-Pressley, LMSW, Child WelfareConsultant and Trainer, Atlanta, GAAngela Stanton-Greenwood, MA, MEd, CQSW,Director of Quality Assurance and WorkforceDevelopment, Hesley Group, and The ListeningPost, EnglandThe Early YearsBatshaw Youth and Family Services, Montreal,QuebecThe Bradley Center, Pittsburgh, PAHillside Family of Agencies, Rochester, NYThe House of the Good Shepherd, Utica, NYKinnark Child & Family Services, Toronto, CanadaHoward Bath, Children’s Commissioner, Northern Territory, AustraliaTHERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University5
PrefaceNicholas F. Quarrier, Department of PhysicalTherapy, Ithaca College, Ithaca, NYNotesOffice of Children and Family Services, State ofNew YorkOffice of Mental Health, State of New YorkPressley Ridge School, Pittsburgh, PASt. Vincent’s Center and Villa Maria Continuumof Catholic Charities, MDTiesha D. Johnson, MS, NPP, RN, Rochester, NYPreface Endnotes61.Hamilton, 2015.2.Nunno, Sellers, & Holden, M. J., 2014.3.For additional information, please go idential-experiences-care/detailed4.National Association of State Mental HealthProgram Directors, 2013.5.Bullard, Fulmore, & Johnson, K., 2003.THERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University
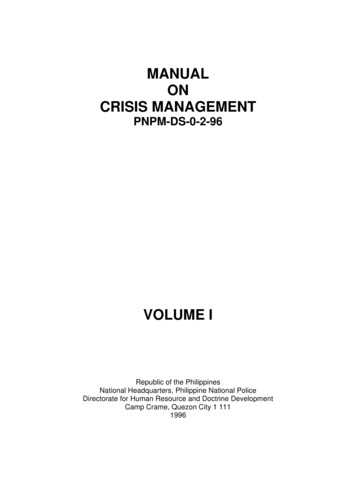
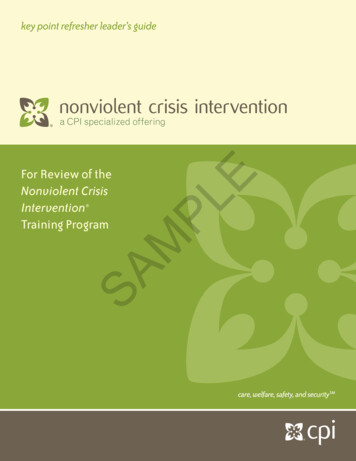
Research Foundations of TCITCI Implementation StudyResearch Foundations of TCIAs a result of the implementation of TCI, the facilitywould see: fewer physical restraint episodes after implementation and trainingThe purpose of the implementation and evaluation fewer injuries to children and staff as a result ofproject involving Cornell University’s Family Lifephysical restraintsDevelopment Center and a residential facility in the increased knowledge and skill on the part of facilityNortheastern Region of the United States was to inpersonnel to handle crisis episodes effectively, andtroduce a crisis prevention and management program, an attitude change among staff and supervisors onTherapeutic Crisis Intervention (TCI), into a residenthe use of physical action in crisis situationstial setting and evaluate its effect.It was recognized that, immediately after TCI trainDeveloped by Cornell University under a grant from ing and implementation, the facility might see anthe National Center on Child Abuse and Neglect in increase in the numbers of incident reports due tothe early 1980s, TCI is a crisis prevention and inter- better reporting, documentation, and monitoring ofvention model for residential child care facilities that incidents.assists organizations in preventing crises from occurring, de-escalating potential crises, managing acutephysical behavior, and reducing potential and actual What Was Cornell’s Implementation andinjury to children and staff. This model gives child and Evaluation Plan?youth care staff the skills, knowledge, and attitudes to The implementation and evaluation project washelp children when they are at their most destructive. designed to be completed in three phases over 18It also provides child care workers an appreciation of months, from October 1994 to March 31, 1996 (Seethe influence that adults have with children who are Figure 3 on page 10).troubled, and the sensitivity to respond to both thefeelings and behavior of a youth in crisis. In all phases The pre-implementation phase: During the firstof this process, from prevention, to de-escalation, to phase of this project (October, 1994 to March, 1995)therapeutic crisis management, the program is ori- prior to implementation of TCI, Cornell staff colented toward residential child care personnel helping lected incident reports, and developed a computerthe child learn developmentally appropriate and con- based data collection instrument to facilitate analysisstructive ways to deal with feelings of frustration, fail- and record incidents.ure, anger, and pain.The training and implementation phase: Duringthe second phase of this project (March 1995 to SepWhat Did Cornell Expect TCI To Accomplish?tember 1995), Cornell staff met with the residentialAs a result of implementing TCI, it was anticipated care staff to administer pre-tests, conduct interviewsthat agency staff would be able to prevent, de-escalate, (all tests and interviews were confidential and anonyand manage crisis situations with children in residen- mous). Four trainers from the organization attendedtial care. More specifically, child care workers and Training of Trainers in Therapeutic Crisis Intervention workshops sponsored by the Residential Childsupervisors would:Care Project. Throughout the training and imple more effectively manage and prevent crisis situationsmentation phase all levels of residential child carewith childrenpersonnel attended TCI training conducted by the feel more confident in their ability to manage crisisCornell-trained residential staff. In addition, supersituations, andvisors attended special sessions conducted by Cornell work as a team to prevent, de-escalate, and managestaff to consider implementation, monitoring, andacute crisessupervisory issues.Project OverviewTHERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University7
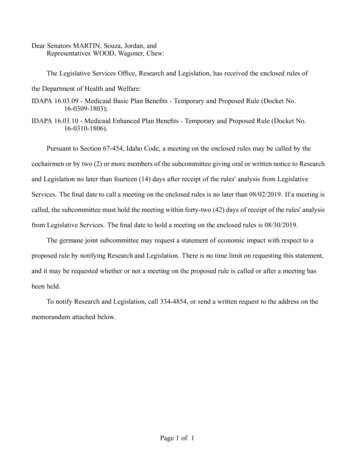
Research Foundations of TCIOverview of Evaluation Design and TimelineMonth:1612 Incident baselinedata (6 months beforeimplementation andtraining) Interviews with childcare staff Pre-implementationconfidence dataImplementation and TrainingPre-post to test mastery of crisisintervention training18 Incident post-data(6 months after fullimplementation) Post-implementationconfidence and knowledgedataFigure 2. Overview of Evaluation Design and TimelineThe post-implementation phase: The post-implementation phase (October 1995 to March 1996) beganafter staff had been trained and the program had beenimplemented. Cornell staff administered post-tests andconducted interviews. Technical assistance was available throughout the life of the project as needed bothvia telephone and on-site. Incident data were collectedfrom October 1, 1995 to March, 1996 and contrastedto the incident data collected prior to implementation.Confidence scales and knowledge based post-tests datacollection continued at periodic intervals.Throughout the life of this 18-month project, incidents were input in a data collection set in order totrack the types and numbers of incidents and the effectsof TCI implementation. An advisory/implementationgroup selected by the agency’s director, and made upof supervisors and clinical staff, met with Cornell staffthroughout the project to help facilitate the project.Integral to the implementation of this TCI methodology was a multi-method evaluation design which (a)provided baseline and follow-up data on crisis episodeswithin the residential care agency for an 18-monthperiod; and (b) evaluated the effectiveness of both thecrisis intervention methodology and the strategy forits implementation via training and technical assistance (See Figure 4). The evaluation design was a mixof qualitative and quantitative methods designed todiscover current crisis intervention practices and toassess whether the project had reached its goals. Thismulti-method approach gave the implementation8team methods to check and recheck the reliability ofboth qualitative and quantitative data gathered. It alsooffered the project team tools to study the phenomenon of crisis events within an organization.Methodology: Evaluation of OutcomesThe incident reports, the pre- and post-implementation interviews with staff and supervisors, the confidence scale and the pre- and post-training knowledgetests were the principal data collection methods forevaluating the effectiveness of the crisis interventionmethodology. The effectiveness of the project’s implementation process was measured by positive changesin staff confidence levels, a decrease in the number ofrestraint episodes, and an increase in the knowledgeand skill levels of staff ( See Table 1 on page 12).What Did Cornell Learn?Multi-Method EvaluationLearning andConfidenceTestsIncidentReviewInterviewsFigure 3. Multi-Method EvaluationTHERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University
Research Foundations of TCIDuring the 18-month implementation period inwhich Cornell worked with the residential agency, thefollowing results were evident: increased staff confidence, greater consistency in approaching children incrisis, documented reductions in incidents, increasedstaff knowledge of crisis dynamics, and an in-housetraining system (See Table 2 on page 13).Confidence Staff members were more confident in their abilityto manage crisis situations. Staff members increased their confidence as a teamin handling crisis situations.Consistency in approaching children in crisis Staff members and supervisors indicated a moreconsistent approach to children in crisis.Reductions in incidents Evidence of reductions in fighting, serious verbalabuse, restraints, and assaults was documented in thethree units that implemented TCI. Statistically significant reductions in physicalrestraints occurred in Unit B.Increased staff knowledge and the developmentof an in-house training system Staff members increased their knowledge of crisisintervention, and this increase in knowledge persisted up to 10 months after training was completed. Selected supervisory staff members learned basicand sophisticated techniques to conduct effectiveand long-lasting training programs.system simply because it was ready to incorporate anagency-wide program.Other fundamental questions remain, for example,about whether the incidence reductions were dueto TCI’s prevention and de-escalation strategies, orwhether the existing leadership through tighter supervision and monitoring alone could have producedthe same reduction. What is necessary is a methodology that incorporates a more sophisticated pre- andpost-design with a sample of organizations in differing geographic areas throughout North America.The basic pre-post design might follow a staggeredschedule of training for units within an agency, as wellas for differing agencies. Implementing this designcan help maintain the internal validity of the project,while supporting its evaluation and monitoring strategies. Such a staggered approach to training is oftennecessitated by institutional concerns of schedulingand resources, but can be used to the advantage of theevaluation effort. The strength of this design derivesfrom the ability to compare baseline data with followup data within each group, but also adds a meaningfulcomparison between the follow-up data of like agencies and units. If these two comparisons yield similar results, then rival hypotheses regarding differencesbetween the groups or temporal changes other thanthe training can be ruled out.Future evaluation design could well be carried outby independent evaluation staff. The introduction ofcontrol or comparison organizations into the evaluation methodology, and an independent evaluatorwould provide more confidence in any results.Study LimitationsThere are limitations with the evaluation methodologyin this study. Although the agency appears representative of numerous small to medium-sized not-forprofit organizations throughout North America, amajor question remains about the process of implementation and the incidence reduction results beinggeneralizable to other organizations. The agency didvolunteer for TCI implementation, and by doing sois a self-selected group. An argument could be madethat this agency would have achieved the same resultswith any other crisis prevention and managementProject SuccessesLeadership. Despite the limitations of our evaluation methodology, the success of this project points tothe necessary elements of leadership, cooperation, andcollaboration among executive, clinical, and supervisory staff within an organization. Through the executive leadership the project gained remarkable accessto the inner workings of a residential agency. Theexecutive director clearly understood and supportedthe notion that any crisis prevention and managementsystem needed to be consistent with the organization’sTHERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University9
Research Foundations of TCIOverview of the Evaluation DesignImplementing, Monitoring, and Evaluating a Therapeutic Crisis Intervention Methodology in a Residential Child CareFacilityInformationDomainsAgency amworkRestraintEpisodesIncreasedKnowledgeand naireand InterviewGuideGeneralQuestionnaireand InterviewGuideGeneralQuestionnaireand InterviewGuideIncidentReportMultipleChoice PrePost-testType of DataGatheredDemographicDataQualitative &Quantitative(Likert scale)Qualitative &Quantitative(Likert scale)Qualitative &Quantitative(Likert scale)QuantitativeQuantitativeNumber ofCorrectResponsesType of ScoreProducedSingle ItemIndicatorsTotal ScoreTotal ScoreTotal ScoreTotalEpisodesItem Analysisand TotalScoreComparedfrom Pre- toPost-testingData Synthesis and Findings Summary1. Report findings which support or refute projected outcomes or hypotheses.2. Report on questions raised that warrant further study.3. Develop an information management system to assess incidents for a residential child care agency.Table 1. Overview of the Evaluation Design10THERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University
Research Foundations of TCIResults of Implementation and Evaluation ProjectINTERVIEWSTESTSINCIDENTSSupervisors report: an increase in staff skills a consistent strategy for intervention higher level of practice standardsConfidence: Tests indicate significantlyincreased levels of confidence in: managing crisis working with co-workers to managecrisis knowledge of agency policy andprocedures helping children learn to copeDocumented reductions over the 18month study in: fighting serious verbal threats physical assaults runawaysfor the entire agencyTraining: Knowledge tests indicate: a significant increase from pre- topost-test in learning scores only a 5% drop in learning after 10months after training, 87% of participantsplan to use the knowledge and skills after training, 93% reported theywere able to use the knowledge andskillsStatistically significant reductions inphysical restraint reports in Unit B overthe 18 month periodWorkers report: more consistent incident reporting consistency in follow-upSupervisors and workers reporteddiffering perceptions of whether adebriefing session occurred and howeffective it was TCI was implemented in Units B, C,D TCI was not implemented in Unit AStatistically significant increases inphysical restraint reports occurred inUnit A (contrast group) over the 18month periodTable 2. Results of Implementation and Evaluation ProjectTHERAPEUTIC CRISIS INTERVENTION SYSTEM: Residential Child Care Project, Cornell University11
Research Foundations of TCImission and philosophy of child care, and had to besupported through clear and well-known policies andprocedures. Through the executive director’s leadership, time and money were allocated to allow the entireresidential services staff to attend TCI training delivered by agency TCI trainers. Supervisors supportedthe project by implementing the behavior management and intervention strategies on a unit basi
that called attention to the large number of envi-ronmental and societal influences on child devel-opment. A Cornell alumnus and Cornell profes-sor, Urie Bronfenbrenner helped form the Head Start Program in the United States in 1965. The BCTR’s mission is to improve pr