Transcription
FANTA 2001 BROCHURE9/19/013:02 PMPage 1HIV/AIDS:A Guide For Nutrition,Care and SupportJuly 2001
FANTA 2001 BROCHURE9/19/013:02 PMPage 2This guide was made possible throughsupport provided to the Food andNutrition Technical Assistance (FANTA)Project by the Office of Health andNutrition of the Bureau for GlobalPrograms Field Support and Research atthe US Agency for InternationalDevelopment, under terms of CooperativeAgreement No. HRN-A-00-98-00046-00awarded to the Academy for EducationalDevelopment (AED). The opinionsexpressed herein are those of the authorand do not necessarily reflect the views ofthe US Agency for InternationalDevelopment.Recommended citation:HIV/AIDS: A Guide For Nutrition,Care and Support. Food and NutritionTechnical Assistance Project, Academy forEducational Development, WashingtonDC, 2001.Published September 2001Copies of the Guide canbe obtained from:Food and Nutrition Technical Assistance(FANTA) ProjectAcademy for Educational Development1825 Connecticut Ave. NW,Washington DC, 20009-5721Tel: 202-884-8000Fax: 202-884-8432Email: fanta@aed.orgWebsite: www.fantaproject.org
FANTA 2001 BROCHURE9/19/013:02 PMPage 3ContentsPage number 7788INTRODUCTIONPurposeAudienceHow To Use This Guide1.1010111112121313131414141415151516MODULE 1.Nutrition and HIV/AIDS: Basic FactsWhat is HIV? What is AIDS?How HIV Is TransmittedHow HIV Is NOT TransmittedHIV Cases in AfricaNutrition and HIV/AIDSAnorexiaDiarrheaFeverNausea/Frequent VomitingThrushAnemiaOther Nutritional Impacts of HIVHow to Maintain Good NutritionMacronutrientsMicronutrientsReferences
FANTA 2001 BROCHURE9/19/013:02 PMPage 4Contents - continued1818181821212121212122222222232323MODULE 2.Coping with HIV: Nutrition and Other Strategies for Living PositivelyGood Nutritional PracticesEat Small but Frequent MealsEat a Variety of FoodsGrowth Promotion and Preventive Health Care for ChildrenSafe Hygienic Practices: Proper Storage and Handling of Food and WaterWaterAnimal ProductsFruits and VegetablesGeneral Foods Storage and HandlingSafer Sexual and Reproductive Health PracticesPhysical ActivityImmediate Attention for IllnessesEating During and After IllnessPsychosocial SupportInvolvement in Community ActivitiesReferences24272829MODULE 3.FOOD MANAGEMENT FOR ADULTS LIVING WITH AIDS-RELATEDSYMPTOMS AND ILLNESSESPlanning Meals for PLWHAsNutritional Counseling and SupportReferences2.3.
FANTA 2001 BROCHURE9/19/013:02 PMPage 5303131333334343435353536MODULE 4.Nutritional Issues Associated with Modernand Traditional TherapiesModern MedicationsTraditional TherapiesDiarrheaFeverCoughHeadachesSore ThroatsSores in the Mouth and ThrushShinglesOther Skin RashesReferences4.37384142MODULE 5.Nutrition and Care Recommendations for Infants/ChildrenMessages for Health Workers and Promoters Working withMothers Whose Status is Unknown or HIV-NegativeRecommendations for Health Workers and Promoters Workingwith HIV-Infected MothersReferences5.43434444444851545455MODULE 6.A Food-Based Approach to Support HIV/AIDS AffectedHouseholds and CommunitiesIntroductionCommunity-Based Care and SupportFacilitating a Community-Led Situation AssessmentDesigning and Implementing a Food ProgramSelecting Ration Size and CompositionLinking Communities with Other ServicesInstitution-Based Feeding ProgramsInstitutional Care for Severely Malnourished IndividualsReferences6.
FANTA 2001 BROCHURE9/19/013:02 PMPage 6AcknowledgementsSerena Rajabiun was the principal author.Many people and organizations contributed to this guide. An early draft ofthe guide was reviewed by organizations in Malawi, Uganda and Zimbabwe.These organizations included: Malawi- Catholic Relief Services, LighthouseClinic, NAPHAM, Network for People Living with HIV/AIDS, US PeaceCorps/Agricultural Research Center and Save the Children; Uganda- TheAIDS Support Organization, Catholic Relief Services and The RegionalQuality of Care Center; Zimbabwe- Catholic Relief Services, The MutareCatholic Health Services.Additional technical input was provided by: Bruce Cogill, Tony Castleman,Paige Harrigan, Marya Khan, Sandra Remancus, Anne Swindale andCaroline Tanner (Food and Nutrition Technical Assistance Project); ReneBerger, Paurvi Bhatt, Eunyong Chung, Paul Delay, Miriam Labbok, JoanLaRosa, Linda Sussman and John Williamson (USAID); Dorcas Lwanga,Micheline Ntiru and Ellen Piwoz (SARA/SANA Project, AED); Mary Kroegerand Jay Ross (Linkages Project, AED); Leslie Elder (World Bank).
FANTA 2001 BROCHURE9/19/013:02 PMPage 7IntroductionApproximately 36 million persons are living with HIV/AIDSworldwide, 25 million of them in Africa. This guide providesinformation for affected households and communities on how to livea healthy life from the time of infection with HIV through the progression ofthe disease. Because a majority of people may not know their HIV status, thefood/diet messages included are appropriate to help all adults and childrenlead healthier, more productive lives. The guide does not cover drugtreatment and preventive practices, but complements other references on thistopic.PurposeThis guide is intended to help development program managers makerecommendations on food management and nutritional issues for householdswith members who are HIV-infected or living with AIDS. The informationfocuses on dietary and care practices for adults during different stages of HIVand also provides suggestions for all household and community memberscoping with the infection and trying to maintain their health and nutritionalstatus.The guide refers to the nutritional care and support needs of individualsinfected with HIV; that is, they have the virus with or without signs of AIDS.The guide is also designed for individuals, families and communities affectedby HIV; that is, they may or may not be HIV-infected but are experiencing thesocial, economic and often health consequences of the virus. The guide isdesigned with the view that sound nutrition practices will benefit bothinfected and affected populations.Since little research is available on nutritional interventions for HIV-infectedchildren, the guide provides general recommendations for improving their7
FANTA 2001 BROCHURE9/19/013:02 PMPage 8nutritional status. Feeding recommendations for both adults and childreninclude using locally available food products, balancing food and nutritionwith medications and selecting appropriate foods through external donationprograms (such as US Title II1 and the World Food Program).Audience Program managers and technical staff working with food aid andfood security programs in HIV-affected areas who seek to designprograms to meet the dietary needs of households coping with infection;Community-based organizations working with care and support issuesfor HIV-affected households who need information on appropriate foodand nutrition practices;Institutions caring for persons living with HIV/AIDS or for children whohave lost one or more parents/guardians to HIV/AIDS; andDistrict health leaders and community and health workers in areasaffected by HIV who are assessing the needs of their communities andtargeting resources to those needs.How To Use This GuideThe guide highlights thematic issues related to HIV/AIDS and nutrition. Thesix modules are organized to allow program managers to select the issuesmost relevant to their programs and incorporate the information as needed.In addition, the modules can be translated and adapted and shared withcommunities and households as a reminder of the simple practices necessaryto maintain a healthy lifestyle. The six modules are:Module 1: Nutrition and HIV/AIDS: Basic FactsThis module provides basic information on HIV/AIDS, the relationshipbetween HIV/AIDS and nutrition and basic elements of good nutrition.Module 2: Coping With HIV: Nutrition and Other Strategies ForLiving PositivelyThis module provides guidelines for helping HIV-infected adults who arenot showing signs of illness maintain good nutrition and health status.1The United States Title II Program is managed by the US Agency for InternationalDevelopment (USAID) Bureau for Humitarian Response, Office of Food for Peace. Privatevoluntary organizations and nongovernmental organizations can solicit requests fordonated US food commodities to use in their development programs. For information,contact USAID’s Bureau for Humanitarian Response at www.usaid.gov/bhr.8
FANTA 2001 BROCHURE9/19/013:02 PMPage 9I N T RO D U C T I O NModule 3: Food Management For Adults Living With AIDS-RelatedSymptoms and IllnessesThis module provides dietary recommendations for adults who arecoping with AIDS-related symptoms and illnesses.Module 4: Nutritional Issues Associated With Modern andTraditional TherapiesThis module describes the nutritional issues associated with therapiesto treat HIV-related illnesses and symptoms. Many people may takemodern medications, such as antibiotics, or use traditional therapiessuch as food and herbs to manage AIDS-related symptoms.Module 5: Nutrition and Care Recommendations For Infants andChildrenThis module provides feeding and care recommendations for infants andchildren regardless of HIV status.Module 6: A Food-Based Approach To Support HIV/AIDS AffectedHouseholds and CommunitiesThis module provides information on the selection, composition and size offood commodities, to program managers who address HIV-affectedpopulations at the community and institutional level.9
MODULEFANTA 2001 BROCHURE1.9/19/013:02 PM1.Page 10Nutrition and HIV/AIDS:Basic FactsThis module provides basic facts onHIV/AIDS, the relationship betweenHIV/AIDS and nutrition and basicelements to maintain good nutrition inadults. This module is designed to provideprogram managers with basic informationto share directly with households andcommunities. The information is focusedon sub-Saharan Africa.What is HIV? What is AIDS?H I V A Human (who is affected)Immunodeficiency (the result)Virus (the causal agent)Acquired (from bodily fluidsthrough a behavior or action,including from the mother duringpregnancy, during delivery orthrough breastmilk)Immune (where the virus attacks)Deficiency (resulting effect of virus)Syndrome (series of illnesses; notjust one)This is why the infections and cancersseen in HIV-infected individuals are called“opportunistic”.Acquired Immune Deficiency Syndrome,or AIDS, is a disease caused by a retrovirusknown as the Human ImmunodeficiencyVirus (HIV), which attacks and impairs thebody’s natural defense system againstdisease and infection. HIV is a slow-actingvirus that may take years to produce illnessin a person. During this period, anHIV-infected person’s defense systemis impaired, and other viruses, bacteriaand parasites take advantage of this“opportunity” to further weaken the bodyand cause various illnesses, such aspneumonia, tuberculosis and oral thrush.There is no cure for HIV/AIDS. Sometherapies can prevent, treat or even curemany of the opportunistic infections andrelieve the symptoms associated withthem, which include fever, coughing,itching, difficulty in breathing orswallowing and chronic diarrhea. Otherdrugs, developed more recently, directlyattack HIV. These antiretroviral (ARV)drugs attack the virus and may slow itsreplication in the body, but they are notcures. The cost of the ARV drugs isdecliningbut,unfortunately,thetreatments are not affordable or accessibleI D S 10When a person starts having opportunisticinfections, he/she has AIDS. The amountof time it takes from HIV infection tobecome full-blown AIDS depends on thegeneral health and nutritional statusbefore and during the time of HIVinfection. The average time for an adult isapproximately ten years.
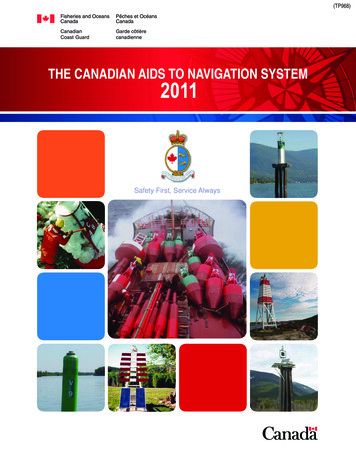
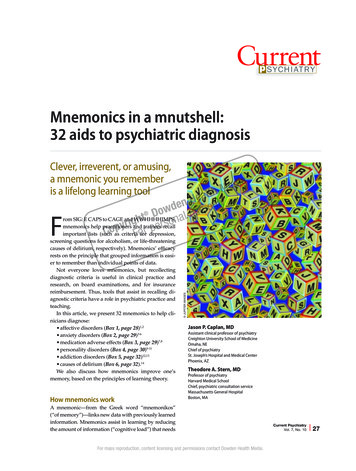
FANTA 2001 BROCHURE9/19/013:02 PMPage 11N U T R I T I O N A N D H I V / A I D S : B A S I C FAC T Sfor most people living with HIV/AIDS(PLWHA). One of the cost-effective drugs(nevirapine), used to prevent mother toMODULE 1.child transmission of the virus duringdelivery, currently costs approximatelyUS 138 per case.How HIV Is TransmittedHIV is transmitted through three primaryroutes: Having unprotected sex with aperson already carrying theHIV virus; Transfusions of contaminatedblood and its by-products; oruse of non-sterilized instrumentssuch as sharing non-sterilizedneedles, razors and otherinstruments for surgical procedures; From infected mother to herchild (mother-to-child transmission,MTCT) during pregnancy, childbirthor breastfeeding.Of children who become infected, 25-40percent will contract HIV duringpregnancy or during labor, and 15 percentthrough breastfeeding.In most of the developing world, HIV ismostly transmitted through sexual contactwith an infected person. Women are morelikely to be infected with HIV than men.Children are also at risk. A pregnantwoman who is HIV-infected has about a15-40 percent risk of infecting her babywith HIV in the absence of antiretrovirals.In other words, of 100 women, 20 will be HIVinfected. Of the 20 who are infected, 12 willnot pass the virus to their infant. Of the 8infants that are HIV-infected, about 3 gotinfected by breastmilk. The remainder wereinfected during pregnancy and delivery.HIV Infected BabiesHow many babies will become HIV-infected if about20% of the mothers are HIV-infected?In a high HIV prevalence community, 20% ofmothers are HIV-infected, the number of babiesinfected by breastmilk will be less than 4percent.Conclusion:The vast majority of babies and mothersare not HIV-infected. Breastfeeding is a safe optionfor this majority.How HIV Is Not TransmittedHIV is not transmitted through: Handshakes, Hugging, Eating from the plate of an HIVinfected person, Mosquitoes or other insects, Kissing, Latrines.Many people do not know that they areinfected with the virus. They may appearhealthy, but still be capable of transmittingthe virus through unprotected sexualintercourse or by reusing contaminatedneedles, razors or other devices, or in thecase of a pregnant or lactating mother,during labor and delivery or throughbreastfeeding her child.REMINDER!HIV is only contracted through the exchange ofbodily fluids. Anyone who suspects that he orshe has been exposed to HIV should consult thenearest health center for voluntary counselingand testing services.111.
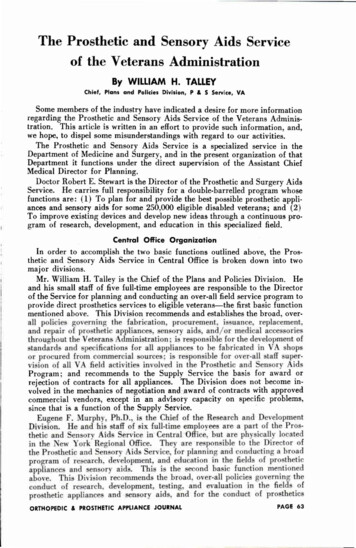
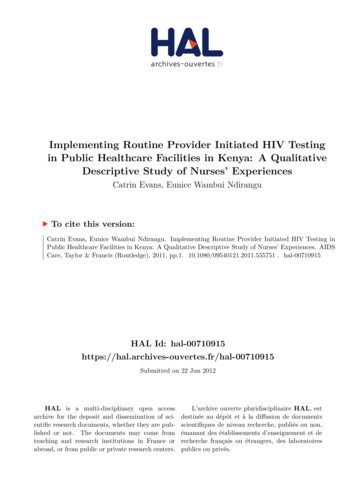
FANTA 2001 BROCHURE9/19/013:02 PMPage 12HIV Cases in AfricaOf the 36 million cases of AIDS worldwidein 2000, two thirds of the cases are in subSaharan Africa.Biologic, economic,cultural and social factors contribute to awoman’s greater risk for HIV infection.Children are also greatly affectedædirectlyand indirectlyæ by AIDS. They maycontract HIV from the mother duringdelivery or via breastmilk, developpediatric AIDS and die. Or they may loseone or both parents to the disease.Children orphaned by AIDS are morelikely to suffer serious nutritional andhealth problems, as well as emotionalstress.Nutrition and HIV/AIDS1.Nutrition and HIV are strongly related toeach other: any immune impairment as aresult of HIV/AIDS leads tomalnutrition, and malnutrition leads to immuneimpairment, worsens the effect ofHIV and contributes to more rapidprogression to AIDS.Thus malnutrition can both contribute toand result from the progression of HIV. Aperson who is malnourished and thenacquires HIV is more likely to progressfaster to AIDS, because his/her body isalready weak and cannot fight infection. Awell-nourished person has a stronger bodyfor coping with HIV and fighting illness.Figure 1 illustrates the relationshipbetween HIV and malnutrition.While people with HIV and AIDS havespecial nutritional needs, it is important tonote that all people will benefit fromadequate nutrition.Good nutritionincreases resistance to infection anddisease, improves energy, and thus makesa person generally stronger and moreproductive.Figure 1. Relationship Between HIV/AIDS and NutritionHIVImmune Impairments“Weak body”“Body can’t fight Illness”Malnutrition“Swollen body and feet”“Pale skin, eyes, hair”“Lack of blood”“Underweight”“Thinness”“Muscle wasting”12Infectious DiseaseDiarrheaTuberculosis(TB)MalariaPneumonia
FANTA 2001 BROCHURE9/19/013:02 PMPage 13N U T R I T I O N A N D H I V / A I D S : B A S I C FAC T SAn HIV-infected person is more at risk formalnutrition for the following reasons:1. Reduced food intake. Adults withHIV/AIDS suffer from appetite loss(anorexia) and have difficulty eating;thus they eat less and fail to meet theirdietary requirements. There are severalreasons for a person to reduce theirintake in food. The person may besuffering from an infection, such asmouth sores or fever. Side effects frommedications used to treat an illness maycause a reduction in appetite.Depression from dealing with a fataldisease and possible social stigma canalso cause people to lose their appetiteand reduce their food intake.2. Poor absorption. HIV/AIDS affectshow the body uses the foods that areconsumed, resulting in poor absorptionof nutrients (protein, carbohydrates,fats, vitamins, minerals and water).Poor absorption of nutrientsaccompanies diarrhea, which iscommon with HIV infection. Parasiteslike giardia and other infections causedby bacteria and viruses cause diarrheaand reduce absorption. HIV may alsodamage intestinal cells that affect theabsorption of fats and carbohydrates.Poor fat absorption also affectsabsorption of micronutrients likeVitamins A and E, which are importantfor the proper functioning of theimmune system.3. Changes in metabolism. With poornutrient absorption, individuals maynot be able digest foods efficiently andtherefore the body may not be able touse the nutrients properly, particularlyfats, carbohydrates and proteins.4. Chronic infections and illnesses.Fevers and infections that accompanyan HIV infection lead to greater nutrientrequirements and poor use of thenutrients by the body. Furthermore,people who are chronically ill may alsohave a reduced appetite, which leads toreduced food intake and weight loss.MODULE 1.The results of these factors include weightloss, loss in lean muscle tissue andincreased damage to the immune system.These factors are most common for adultsbut they are also prevalent in childreninfected with HIV.A number of other symptoms and illnessescommonly caused by HIV infection havenutritional consequences that can lead tomalnutrition.AnorexiaAnorexia, or loss of appetite, occurs duringmany different infections and when fever ispresent. It leads to general weight loss, andis common when individuals aredepressed or are living in socially andemotionally unfavorable environments.DiarrheaDiarrhea occurs when a person hasseveral watery or loose bowel movementsin a day. There are several causes fordiarrhea: unclean drinking water,infections, parasites or even some medicaltreatments. It results in losses of water,nutrients and minerals and leaves a personat greater risk of dehydration. Diarrheaalso reduces appetite and leads to poornutrient absorption. If diarrhea continuesfor a prolonged period of time, severemalnutrition results.FeverFever means that the body feels warmerthan normal. People with fever may havethe chills, sweat more, have muscle andjoint aches or be fatigued. Fever iscommon in people living with HIV/AIDS,and does not necessarily indicate a seriousillness. There are many reasons for fever,and it is often hard to determine whetherfever is due to HIV or to other illnessessuch as malaria. From a nutritional pointof view, fever may result in increasednutrient requirements, since the bodyutilizes nutrients poorly when fever ispresent.131.
FANTA 2001 BROCHURE9/19/013:02 PMPage 14Nausea/Frequent VomitingNausea and frequent vomiting can resultfrom the drugs used to treat HIV/AIDS orfrom the opportunistic infections. Nauseaalso leads to reduced appetite and poorutilization of the food consumed.ThrushThrush is a fungal (candida yeast)infection common in HIV-infected peoplewho have damaged immune systems.Thrush refers to whitish spots on the insideof the mouth, tongue, vagina or anus.Although these sores are uncomfortable,they are not life threatening. The danger isthat these sores can result in difficultyeating foods, loss of appetite and reducedfood intake and thus lead to weight loss.1.AnemiaAnemia results from an inadequatenumber or quality of red blood cells in thebody. This is most often due to a lack ofiron in the diet and to infections such asmalaria and hookworm, which destroy redblood cells and may lead to bleedingand/or loss of blood. Women and childrenare especially prone to anemia. Personswho are anemic often experience tirednessand weakness and may have pallor(paleness) in the eyes, tongue, palms andnail-beds. The relationship between HIVand anemia is not clearly understood,although it is known that HIV-infectedpersons who are anemic generallyprogress faster to AIDS than those who arenot.Summary of Nutritional Imacts of HIVPoor food intakePoor nutrient absorption Disruption of metabolism Chronic infection Muscle wasting or loss in lean bodytissue Illnesses Associated with NutritionalImpacts Anorexia Diarrhea Fever Nausea Thrush AnemiaExcerpted from Network of African PeopleLiving with AIDS (November 1997).Other Nutritional Impacts of HIVIn households with HIV-infected members,others may also experience nutritionalimpacts, particularly young children andorphans. Sometimes when adults becomeinfected with the virus, they are too sick towork and cannot continue to provide forthemselves and their families. This canresult in reduced income for the14household-—and hence fewer resources(labor and money) to obtain food. Inaddition, other family members suddenlyfind themselves working more, either toproduce income or to provide care for theHIV-infected individual, which can alsolead to a deterioration in nutritional statusfor themselves and their children.
FANTA 2001 BROCHURE9/19/013:02 PMPage 15N U T R I T I O N A N D H I V / A I D S : B A S I C FAC T SMODULE 1.How to Maintain Good NutritionGood nutrition for all individuals, butespeciallyPLWHAs,requirestheconsumption of an adequate amount of: macronutrients (proteins,carbohydrates and fats), andmicronutrients (vitamins andminerals).MacronutrientsA deficiency in macronutrients, alsoknown as “protein-energy malnutrition,”manifests itself in the weight loss andwasting that is typical of AIDS patients.These symptoms occur as a result ofreduced food intake; poor absorption ofnutrients; and changes in metabolism thataffect cell growth, enzymatic processes andimmune system reactions.Because of these effects, an HIV-infectedperson has additional nutrient requirements: 10-15 percent additional energyintake and 50 to 100 percent increase inprotein intake as compared to a non HIVinfected person. (Module 6 gives someexamples of calculating additional nutrientneeds for HIV-affected households.)Energy NeedsAn active non-HIV-infected adult requiresapproximately 2070 kcal/day.An HIV-infected adult requires 10 to 15percent more energy per day (or approximately 400 additional kcal for men and 300kcal for women).Protein needs:A non-HIV-infected man requires about 57grams/day of protein and a woman requires 48grams/day.MicronutrientsConsuming micronutrients (especiallyVitamins A, B6 and B12, iron and zinc) isimportant for building a strong immunesystem and fighting infections.Forexample, Vitamin A deficiency isassociated with higher maternal-childtransmission rates, faster progression fromHIV to AIDS, higher infant mortality andchild growth failure.The B-groupvitamins play important roles in immuneregulations, and deficiencies play a role indisease progression.Micronutrient consumption can beincreased through eating specific foods orthrough special supplements. In manysettings,establishinghomeandcommunity gardens to grow local foodsand vegetables is important to improveintake of vitamin and mineral rich foods.Also, raising small animals (e.g., chickens)should be considered to help improve theconsumption of protein, fat, as well asmicronutrients such as iron and Vitamin A.The impact of taking micronutrientsupplements on HIV infection is not wellknown. The most promising results arefor Vitamin A and the B-group vitamins.Vitamin B6 (niacin) and B12 supplementation have been shown to improvesurvival and reduce disease progression,although only in healthy populationswhere micronutrient deficiencies are notcommon and when intakes were high.Vitamin B6 (10 mg daily) supplementationis also recommended for TB patients beingtreated with isoniazid.Vitamin Asupplementation for children of HIVinfected mothers has been shown toreduce illness, particularly diarrhea.Vitamin A supplements are alsorecommended for mothers immediatelyafter delivery and for infants 6 months andolder.An HIV-infected adult needs approximately 50to 100 percent more protein for a total of85 grams/day for men and 72 grams/day forwomen.Sources: Woods (1999); James and Shofield(1990);WHO (1985).151.
FANTA 2001 BROCHURE9/19/013:02 PMPage 16Multiple Positive Impacts For PLWHAAdequate nutrition has multiple positive effectsfor a PLWHA:Prevents malnutrition and wasting,Achieves and maintains optimalbody weight and strength, Enhances the body’s ability to fightopportunistic infections, May help delay the progression ofHIV, Improves the effectiveness of drugtreatments, Improves the quality of life. Yet in many African settings, takingmicronutrient supplements may bedifficult due to lack of availability and highcost. Establishing links to health servicesand private-sector sources for a regularsupply of micronutrient supplements isbeneficial to communities. Optimal nutrition helps all people feelbetter, stay healthier and live longer,whether they are HIV-infected or not.References1.Bijlsma, Marlou. July 2000 (draft).“Nutritional Care and Support for Peoplewith HIV: Review of the Literature,Initiatives and Educational Materials inSub-Saharan Africa and RecommendationsforDevelopingNationalProgrammes.” Report to FAO.James, W.P.T., and E. C. Schofield 1990.Human Energy Requirements: A Manualfor Planners and Nutritionists. Oxford:Oxford University Press. Food andAgriculture Organization.Joint United Nations Program onHIV/AIDS (UNAIDS) and WorldHealthOrganization(WHO).December 2000. AIDS Epidemic Update.Document No.: UNAIDS/00.44E orWHO/CDS/CSR/EDC/2000.9. Geneva.Marseille, E., J. Kahn, F. Mmiro, et al.“Cost Effectiveness of Single DoseNevirapine Regimen for Mothers andBabies to Decrease Vertical HIV-1Transmission in Sub-Saharan Africa.”Lancet. 354, No. 9181, September 4, 1999, p.803-809.16Ministry of Agriculture, AnimalIndustry and Fisheries, Republic ofUganda,andUnitedNationsDevelopment Programme (UNDP).1998. “Nutrition and HIV/AIDS: AHandbook for Field Extension Agents.”National AIDS Control Program,Ministry of Health and Population,Malawi. 2000 (draft). “Home-Based CareProviders Handbook.” Lilongwe.Network of African People Living withHIV/AIDS. November, 1997. “A HealthyDiet for Better Nutrition for People Livingwith HIV/AIDS.” Nairobi, Kenya.Piwoz, E.G., and E.A. Preble. November2000. HIV/AIDS and Nutrition: A Review ofthe Literature and Recommendations forNutritional Care and Support in Africa.Washington, DC: Academy for EducationalDevelopment.
FANTA 2001 BROCHURE9/19/013:02 PMPage 17N U T R I T I O N A N D H I V / A I D S : B A S I C FAC T SSemba, R., 1999. Micronutrients andMicronutrient-Replacement Therapy. In T.Miller, and S. Gorbach. Nutritional Aspectsof HIV Infection. New York: OxfordUniversity Press.United States Peace Corps, Center forFieldAssistanceandAppliedResearch. July 2000. “Life Skills Manual.”Publication M0061. Washington DC:Information Collection and Exchange.Woods M.N. 1999. Dietarydations for the HIV/AIDST. Miller and S. Gorbach,Aspects of HIV Infection.Oxford University Press.MODULE 1.WebsitesUNAIDS:www.unaids.orgUSAID, Office of Population, Health,and Nutrition (PHN):www.usaid.gov/pop health/aids/index.htmlWHO Department of HIV/AIDS:www.who.int/HIV AIDS/index.htmlRecommenPatient. InNutritionalNew York:1.17
MODULEFANTA 2001 BROCHURE9/19/013:02 PM2.Page 18Coping with HIV:Nutrition and OtherStrategies for LivingPositivelyFor an HIV-infected person, the goal ofliving “positively” is to be free of illness, tobe productive and to stay emotionally andphysically healthy. This module offersdietary and related recommendationsprogram managers can promote to helpPLWHAs live a healthy life.Good Nutritional Practices2.Dietary practice plays an important role inmaintaining a healthy lifestyle. An HIVinfected person already has a weakenedimmune system. A nutritious diet can helpto maintain the proper functioning of theimmune system and provides neededenergy, protein and micronutrients.Program managers can promote a numberof nutritional practices that HIV-infectedindividuals and their families can take tomaintain health. The following suggestions are provided as general principles inresponding to the nutritional needs of HIVaffected populations.Eat Small but Frequent MealsMaintaining good nutritional status helpsto build and maintain the immune system,allowing the body to fight infection. Tolead a healthier life all people, whetherHIV-infected or not, need to meet theirdaily energy, protein and micronutrientrequirements. Persons with HIV mayexperience difficulties with food intake dueto illnesses such as thrush (mouth sores)or to poor nutrient absorption. To ensure18that PLWHAs receive sufficient nutrients, itis important that they eat smaller portions(so that the stomach can absorb foods) andmore frequently throughout the day.Encourage snacking throughout the day toincrease intake of food. It is helpful toprepare special softer foods for those whoare ill. Softer foods are more moist andmay be tolerated better during periods ofillness.Eat a Variety of foodsMaintaining adequate nutritional statusmeans consuming a variety of foods to besure the body is getting the necessaryenergy, protein and micronutrients itneeds. PLWHAs should eat a “balanced”diet consisting of beans, nuts, animal foods,starchy staples (rice, potato, maize), fruitsa
There is no cure for HIV/AIDS. Some therapies can prevent, treat or even cure many of the opportunistic infections and relieve the symptoms associated with them, which include fever, coughing, itching, difficulty in breathing or swallowing and chronic diarrhea. Other drugs, developed more