Transcription
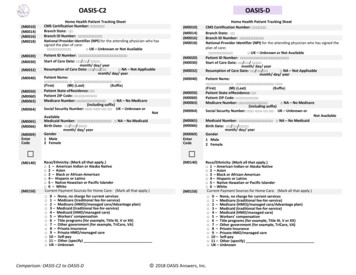
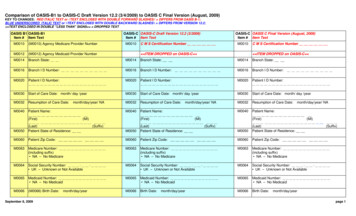
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item TextOASIS-C OASIS C Final Version (August, 2009)Item # Item TextOASIS-C OASIS-C Draft Version 12.2 (3/2009)Item # Item TextM0010(M0010) Agency Medicare Provider NumberM0012(M0012) Agency Medicaid Provider NumberM0014Branch State:M0016Branch I D Number:M0020Patient I D Number:M0010////C M S Certification NumberM0010 ITEM DROPPED on OASIS-C //M0014Branch State:M0016Branch I D Number:M0020Patient I D Number://////C M S Certification Number ITEM DROPPED on OASIS-C //M0014Branch State:M0016Branch I D Number:M0020Patient I D Number:M0030Start of Care Date: month/ day /yearM0030Start of Care Date: month/ day /yearM0030Start of Care Date: month/ day /yearM0032Resumption of Care Date:M0032Resumption of Care Date:M0032Resumption of Care Date:M0040Patient Name:M0040Patient Name:month/day/year/ NA(First)(MI)M0050(Last)Patient State of Residence:M0060month/day/year/ NA(First)M0040M0050(Last)Patient State of Residence:Patient Zip Code:M0060M0063Medicare Number:(including suffix) NA – No MedicareM0064month/day/year/ NAPatient st)Patient State of Residence:Patient Zip Code:M0060Patient Zip Code:M0063Medicare Number:(including suffix) NA – No MedicareM0063Medicare Number:(including suffix) NA – No MedicareSocial Security Number: - - UK – Unknown or Not AvailableM0064Social Security Number: - - UK – Unknown or Not AvailableM0064Social Security Number: - - UK – Unknown or Not AvailableM0065Medicaid Number: NA – No MedicaidM0065Medicaid Number: NA – No MedicaidM0065Medicaid Number: NA – No MedicaidM0066(M0066) Birth Date:M0066Birth Date:M0066Birth Date:September 8, yearpage 1
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item TextOASIS-C OASIS C Final Version (August, 2009)Item # Item TextOASIS-C OASIS-C Draft Version 12.2 (3/2009)Item # Item TextM0069(M0069) Gender: 1 - Male 2 - FemaleM0069M0072(M0072) Primary Referring Physician id: (UPIN#)M0018Gender: 1 - Male 2 - FemaleM0069Gender: 1 - Male 2 – FemaleNational Provider identifier (NPI) for the attendingphysician who has signed the plan of care: UK – Unknown or Not AvailableM0018National Provider identifier (NPI) for the attendingphysician who has signed the plan of care: UK – Unknown or Not AvailableRace/Ethnicity:(Mark all that apply.) 1 - American Indian or Alaska Native 2 - Asian 3 - Black or African-American 4 - Hispanic or Latino 5 - Native Hawaiian or Pacific Islander 6 – WhiteM0140//// UK - Unknown or Not AvailableM0140M0150(M0140) Race/Ethnicity (as identified by patient): (Mark allthat apply.) 1 - American Indian or Alaska Native 2 - Asian 3 - Black or African-American 4 - Hispanic or Latino 5 - Native Hawaiian or Pacific Islander 6 - White UK – UnknownM0140(M0150) Current Payment Sources for Home Care: (Markall that apply.) 0 - None; no charge for current services 1 - Medicare (traditional fee-for-service) 2 - Medicare (HMO/managed care) 3 - Medicaid (traditional fee-for-service) 4 - Medicaid (HMO/managed care) 5 - Workers' compensation 6 - Title programs (e.g., Title III, V, or XX) 7 - Other government (e.g., CHAMPUS, VA, etc.) 8 - Private insurance 9 - Private HMO/managed care 10 - Self-pay 11 - Other (specify) UK – UnknownM0150September 8, 2009////// DROPPED: UK – Unknown //Race/Ethnicity:(Mark all that apply.) 1 - American Indian or Alaska Native 2 - Asian 3 - Black or African-American 4 - Hispanic or Latino 5 - Native Hawaiian or Pacific Islander 6 – White//Current Payment Sources for Home Care: (Mark all thatapply.) 0 - None; no charge for current services 1 - Medicare (traditional fee-for-service) 2 - Medicare (HMO/managed care Advantage plan) 3 - Medicaid (traditional fee-for-service) 4 - Medicaid (HMO/managed care) 5 - Workers' compensation 6 - Title programs (e.g., Title III, V, or XX) 7 - Other government (e.g., TriCare, VA, etc.) 8 - Private insurance 9 - Private HMO/managed care 10 - Self-pay 11 - Other (specify) UK - Unknown/////M0150 DROPPED: UK – Unknown //Current Payment Sources for Home Care: (Mark all thatapply.) 0 - None; no charge for current services 1 - Medicare (traditional fee-for-service) 2 - Medicare (HMO/managed care Advantage plan) 3 - Medicaid (traditional fee-for-service) 4 - Medicaid (HMO/managed care) 5 - Workers' compensation 6 - Title programs (e.g., Title III, V, or XX) 7 - Other government (e.g., TriCare, VA, etc.) 8 - Private insurance 9 - Private HMO/managed care 10 - Self-pay 11 - Other (specify) UK – Unknown/////page 2
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item TextOASIS-C OASIS C Final Version (August, 2009)Item # Item TextOASIS-C OASIS-C Draft Version 12.2 (3/2009)Item # Item TextM0080(M0080) Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OTM0080Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OTM0080Discipline of Person Completing Assessment: 1-RN 2-PT 3-SLP/ST 4-OTM0090(M0090) Date Assessment Completed:month/day /yearM0090Date Assessment Completed:month/day/yearM0090Date Assessment Completed:month/day/yearM0100(M0100) This Assessment is Currently Being Completed forthe Following Reason:Start/Resumption of Care1 – Start of care—further visits planned3 – Resumption of care (after inpatient stay)Follow-Up4 – Recertification (follow-up) reassessment [ Go toM0110 ]5 – Other follow-up [ Go to M0110 ]Transfer to an Inpatient Facility6 – Transferred to an inpatient facility—patient notdischarged from agency [ Go to M0830 ]7 – Transferred to an inpatient facility—patient dischargedfrom agency [ Go to M0830 ]Discharge from Agency — Not to an Inpatient Facility8 – Death at home [ Go to M0906 ]9 – Discharge from agency [ Go to M0200 ]M0100This Assessment is Currently Being Completed for theFollowing Reason:Start/Resumption of Care1 – Start of care—further visits planned3 – Resumption of care (after inpatient stay)Follow-Up4 – Recertification (follow-up) reassessment [ Go toM0110 ]5 – Other follow-up [ Go to M0110 ]Transfer to an Inpatient Facility6 – Transferred to an inpatient facility—patient notdischarged from agency [ Go to M1040 ]7 – Transferred to an inpatient facility—patient dischargedfrom agency [ Go to M1040 ]Discharge from Agency — Not to an Inpatient Facility8 – Death at home [ Go to M0906 ]9 – Discharge from agency [ Go to M1032 ]M0100This Assessment is Currently Being Completed for theFollowing Reason:Start/Resumption of Care1 – Start of care—further visits planned3 – Resumption of care (after inpatient stay)Follow-Up4 – Recertification (follow-up) reassessment [ Go toM0110 ]5 – Other follow-up [Go to M0110]Transfer to an Inpatient Facility6 – Transferred to an inpatient facility—patient notdischarged from agency [ Go to M1040 ]7 – Transferred to an inpatient facility—patient dischargedfrom agency [ Go to M1040 ]Discharge from Agency — Not to an Inpatient Facility8 – Death at home [Go to M0903 ]9 – Discharge from agency [Go to M1040 ]New item on OASIS-CM0102Date of Physician-ordered Start of Care (Resumption ofCare): If the physician (or physician designee)indicated a specific start of care (resumption of care)date when the patient was referred for home healthservices, record the date specified./ /month / day / year(Go to M0110, if date entered)NA –No specific SOC date ordered by physician (orphysician designee)M0102//////////September 8, 2009\\//\\\\\\Date of Physician-ordered Start of Care (Resumption ofCare): If the physician DROPPED: (or physiciandesignee) indicated a specific start of care(resumption of care) date when the patient was referredfor home health services, record the date specified./ /month / day / year(Go to M0110, if date entered)NA –No specific SOC date ordered byphysician DROPPED: (or physician designee) ////\\\\//\\\\page 3
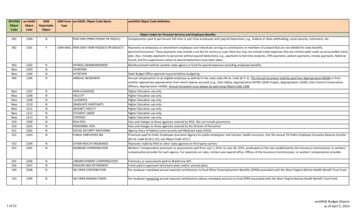
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item Text/OASIS-C OASIS-C Draft Version 12.2 (3/2009)Item # Item TextNew item on OASIS-C//M0104OASIS-C OASIS C Final Version (August, 2009)Item # Item TextDate of Referral: Indicate the date that the written ordocumented orders from the physician or physiciandesignee for initiation or resumption of care werereceived by the HHA./ /month / day / yearM0104//Date of Referral: Indicate the date that the written or DROPPED: documented orders from the physicianor physician designee verbal referral for initiation orresumption of care was received by the HHA./ /month / day / year//\\//\\////M0110(M0110) Episode Timing: Is the Medicare home healthpayment episode for which this assessment will define acase mix group an “early” episode or a “later” episode inthe patient’s current sequence of adjacent Medicare homehealth payment episodes? 1 - Early 2 - Later UK - Unknown NA - Not Applicable: No Medicare case mix group to bedefined by this assessment.M0110Episode Timing: Is the Medicare home health paymentepisode for which this assessment will define a case mixgroup an “early” episode or a “later” episode in the patient’scurrent sequence of adjacent Medicare home healthpayment episodes? 1 - Early 2 - Later UK - Unknown NA - Not Applicable: No Medicare case mix group to bedefined by this assessment.M0110Episode Timing: Is the Medicare home health paymentepisode for which this assessment will define a case mixgroup an “early” episode or a “later” episode in the patient’scurrent sequence of adjacent Medicare home healthpayment episodes? 1 - Early 2 - Later UK - Unknown NA - Not Applicable: No Medicare case mix group to bedefined by this assessment.M0175(M0175) From which of the following Inpatient Facilitieswas the patient discharged during the past 14 days? (Markall that apply.) 1 - Hospital 2 - Rehabilitation facility 3 - Skilled nursing facility 4 - Other nursing homeM1000From which of the following Inpatient Facilities was thepatient discharged during the past 14 days? (Mark all thatapply.)1 - Long-term nursing facility2 - Skilled nursing facility (S N F / T C U)3 - Hospital emergency department4 - Short-stay acute hospital (I P P S)5 - Long-term care hospital (L T C H)6 - Inpatient rehabilitation hospital or unit ( I R F)7 - Psychiatric hospital or unit8 - Other (specify)NA - Patient was not discharged from an inpatient facility[Go to M1016 ]M1000From which of the following Inpatient Facilities was thepatient discharged during the past 14 days? (Mark all thatapply.)1 - Long-term nursing facility ( N F )2 - Skilled nursing facility ( S N F / T C U)Inpatient Discharge Date (most recent):month/day/year UK – UnknownM1005////M0180(M0180) Inpatient Discharge Date (most recent):month/day/year UK - UnknownSeptember 8, 2009M1005\\\\//// DROPPED: 3 - Hospital emergency department //\\3 - Short-stay acute hospital ( I P P S )4 - Long-term care hospital ( L T C H )5 - Inpatient rehabilitation hospital or unit ( I R F)6 - Psychiatric hospital or unit7 - Other (specify)NA - Patient was not discharged from an inpatient facility[Go to M1016 ]\\// 5 - Other (specify) NA - Patient was not discharged from an inpatient facility[If NA, go to M0200 ]//\\Inpatient Discharge Date (most recent):month/day/year UK – Unknownpage 4
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item TextM0190(M0190) List each Inpatient Diagnosis and ICD 9 CM codeat the level of highest specificity for only those conditionstreated during an inpatient stay within the last 14 days (nosurgical, E codes, or V codes):Inpatient Facility Diagnosis ICD-9-CMa. ( )b. ( )M1010List each Inpatient Diagnosis and ICD-9-CM code at thelevel of highest specificity for only those conditions treatedduring an inpatient stay within the last 14 days (no E codes,or V codes):Inpatient Facility DiagnosisICD-9-CM Codea.b.c.d.e.f.////New item on OASIS-C//M1012NA - Not applicableUK - UnknownSeptember 8, 2009//////M1012.//List each Inpatient Procedure and the associated ICD9-CM procedure code relevant to the plan of care.Inpatient ProcedureProcedure Code//a.b.c.d.NA - Not applicableUK - Unknown//(M0200) Medical or Treatment Regimen Change WithinPast 14 Days: Has this patient experienced a change inmedical or treatment regimen (e.g., medication, treatment,or service change due to new or additional diagnosis, etc.)within the last 14 days? 0 - No [ If No, go to M0220; if No at Discharge, go toM0250 ] 1 – Yes.List each Inpatient Diagnosis and ICD-9-CM code at thelevel of highest specificity for only those conditions treatedduring an inpatient stay within the last 14 days (no E codes,or V codes):Inpatient Facility DiagnosisICD-9-CM Codea.b.c.d.e.f.//List each Inpatient Procedure and the associated ICD9-CM procedure code relevant to the plan of care.Inpatient ProcedureProcedure CodeM1010.//a.b.c.d.M0200OASIS-C OASIS C Final Version (August, 2009)Item # Item TextOASIS-C OASIS-C Draft Version 12.2 (3/2009)Item # Item Text// ITEM DROPPED on OASIS-C (incorporated as NA in M1016)//// ITEM DROPPED on OASIS-C (incorporated as NA in M1016)////page 5
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item TextM0210(M0210) List the patient's Medical Diagnoses and ICD 9CM codes at the level of highest specificity for thoseconditions requiring changed medical or treatment regimen(no surgical, E codes, or V codes)::OASIS-C OASIS C Final Version (August, 2009)Item # Item TextOASIS-C OASIS-C Draft Version 12.2 (3/2009)Item # Item TextM1016Diagnoses Requiring Medical or Treatment RegimenChange Within Past 14 Days: List the patient's MedicalDiagnoses and ICD-9-CM codes at the level of highestspecificity for those conditions requiring changed medicalor treatment regimen within the past 14 days. (no surgical,E codes, or V codes):Changed Medical Regimen Diagnosis ICD-9-CMChanged Medical Regimen Diagnosisa.b.c.d.a.b.c.d.e.f.( )( )( )( )//M1016ICD-9-CMCodeChanged Medical Regimen Diagnosis.a.b.c.d.e.f.//NA - Not applicable (no medical or treatment regimenchanges within the past 14 days)(M0220) Conditions Prior to Medical or Treatment RegimenChange or Inpatient Stay Within Past 14 Days: If thispatient experienced an inpatient facility discharge orchange in medical or treatment regimen within the past 14days, indicate any conditions which existed prior to theinpatient stay or change in medical or treatment regimen.(Mark all that apply.) 1 - Urinary incontinence 2 - Indwelling/suprapubic catheter 3 - Intractable pain 4 - Impaired decision-making 5 - Disruptive or socially inappropriate behavior 6 - Memory loss to the extent that supervision required 7 - None of the above NA - No inpatient facility discharge and no change inmedical or treatment regimen in past 14 days UK - UnknownSeptember 8, 2009M1018Conditions Prior to Medical or Treatment Regimen Changeor Inpatient Stay Within Past 14 Days: If this patientexperienced an inpatient facility discharge or change inmedical or treatment regimen within the past 14 days,indicate any conditions which existed prior to the inpatientstay or change in medical or treatment regimen. (Mark allthat apply.)1 - Urinary incontinence2 - Indwelling/suprapubic catheter3 - Intractable pain4 - Impaired decision-making5 - Disruptive or socially inappropriate behavior6 - Memory loss to the extent that supervisionrequired7 - None of the aboveNA - No inpatient facility discharge and no change inmedical or treatment regimen in past 14 daysUK - UnknownICD-9-CMCode.NA - Not applicable (no medical or treatment regimenchanges within the past 14 days)//M0220Diagnoses Requiring Medical or Treatment RegimenChange Within Past 14 Days: List the patient's MedicalDiagnoses and ICD-9-CM codes at the level of highestspecificity for those conditions requiring changed medical ortreatment regimen within the past 14 days. (no surgical, Ecodes, or V codes)://M1018Conditions Prior to Medical or Treatment Regimen Changeor Inpatient Stay Within Past 14 Days: If this patientexperienced an inpatient facility discharge or change inmedical or treatment regimen within the past 14 days,indicate any conditions which existed prior to the inpatientstay or change in medical or treatment regimen. (Mark allthat apply.)1 - Urinary incontinence2 - Indwelling/suprapubic catheter3 - Intractable pain4 - Impaired decision-making5 - Disruptive or socially inappropriate behavior6 - Memory loss to the extent that supervisionrequired7 - None of the aboveNA - No inpatient facility discharge and no change inmedical or treatment regimen in past 14 daysUK - Unknownpage 6
Comparison of OASIS-B1 to OASIS-C Draft Version 12.2 (3/4/2009) to OASIS C Final Version (August, 2009)KEY TO CHANGES: RED ITALIC TEXT or //TEXT ENCLOSED WITH DOUBLE FORWARD SLASHES// DIFFERS FROM OASIS B-1;BLUE UNDERSCORED ITALIC TEXT or \\TEXT ENCLOSED WITH DOUBLE BACKWARD SLASHES\\ DIFFERS FROM VERSION 12.2; TEXT ENCLOSED IN DOUBLE “LESS THAN” SIGNS DROPPED TEXTOASIS B1 OASIS-B1Item # Item TextM0230M0230/240/246 Diagnoses, Severity Index, and PaymentDiagnoses: List each diagnosis for which the patient isreceiving home care (Column 1) and enter its ICD-9-CMcode at the level of highest specificity (nosurgical/procedure codes) (Column 2) . Rate eachcondition (Column 2) using the severity index. (Choose onevalue that represents the most severe rating appropriate foreach diagnosis.) V codes (for M0230 or M0240) or Ecodes (for M0240 only) may be used. ICD-9-CMsequencing requirements must be followed if multiplecoding is indicated for any diagnoses. If a V code isreported in place of a case mix diagnosis, then optionalitem M0246 Payment Diagnoses (Columns 3 and 4) maybe completed. A case mix diagnosis is a diagnosis thatdetermines the Medicare PPS case mix group.OASIS-C OAS
comparison of oasis-b1 to oasis-c draft version 12.2 (3/4/2009) to oasis c final version (august, 2009) key to changes: red italic text or //text enclosed with double forward slashes// differs from oasis b-1; blue underscored italic text or \\text enclosed wi