Transcription
Documentation & Coding Compliance forOtolaryngology – Head & Neck SurgeryStephen R. Levinson, claimer This presentation is designed to provideaccurate and authoritative information inregard to the subject matter covered. Theinformation includes both reporting andinterpretation of materials in variouspublications, as well as interpretation ofpolicies of various organizations. Thisinformation is subject to individualinterpretation and to changes over time Presenter has personal interests in consulting,presenting, writing about, and developingsoftware in order to help physicians achievecompliant medical records and to help themfacilitate quality patient careASA,LLCAttendee Demographics Physician offices Hospital / Academic MedicalCenter Medicare / Insurers Consultant HIT Other1
Today’s Agenda: Otolaryngology - HNSPrinciples of procedure coding– Selecting appropriate codes– When and how to use procedure modifiers Ear and Balance ProceduresNose & Sinus ProceduresOropharynx & Head & Neck ProceduresPlastic & Reconstructive ProceduresCoding E/M & procedures on same DOS ?– Codes with XXX global designation– E/M modifiers and how to use them compliantly– Office diagnostic procedures (0 & 10 day global)Compliance Tools CPT (AMA) ICD-9 (AMA) RBRVS for Physicians– RVUs– Global periods CCI www. ENTcodingtoday.com,Encoder Pro, or other webbased toolsSetting the Table Discussion is NOT about black &white rules, but about principles& tools and working in the grayzone Format – open dialogue withquestions and critiques– Umpty-three thousand ENT codes;please ask about those of interest– NOT the med school definition of a“lecture”2
Medical Record Formats? – MDs/staff Data Storage– Paper– Electronic EHR Scanning system Data entry– Writing on paper– Dictation Transcription Voice recognition software Using some form of template foroperative reports?– In O.R.– In officeCoding Practices Who does coding for Procedures– Physician primary– Coder primary– Is there review when questions? Who does coding for E/M services– Physician primary– Coder primary– Is there review when questions? Are there educational conferencesscheduled with coders & MDs– Regularly scheduled group sessions– As needed group sessionsCoding Procedure Services3
Coders’ Role in Procedure Coding When coder does primarycoding: Review operative report– Operation performed sectionis only the starting point– Must review details of opreport to confirm accuracy ofoperative designation– Then select appropriatecode(s) If any question ofdocumentation or coding,must review with physician When the physician doesthe primary coding: Coder reviews the report toconfirm that documentationsupports the submittedcodes– And to assess if additionalprocedures were alsoperformed that should becoded If any question ofdocumentation or coding,must review with physicianCoders’ Role as Educator Physicians need understand coding - to appreciate thedetails that must be documented in their dictation tosupport coding of the procedure performed– For example, if physician submits code for totalethmoidectomy (31255) must document performance ofsurgery on the posterior ethmoid cells– (“if it wasn’t documented, it wasn’t done”) Should discuss any discrepancies, add a dated correctionnote if necessary (and if appropriate) Should lead to prevention of discrepancies in futurecasesCoders’ Tools for Auditing Procedures CPT (AMA)ICD-9 (AMA)HCPCS Level IIMedical Dictionary?Anatomy book (e.g., Netter)Photocopy of operative noteHighlighter4
Suggested Architecture (Template)for an Op Note Patient informationSurgeonDate of OperationOperation PerformedPre-op diagnosisPost-op diagnosis Indications for surgery Operative findings Procedure - detailed andprocedure specificdescription of operationUse of Macros ? Which components ofprocedure description areacceptable for macro?The Rubber Stamp– Even for this, need protectionby separate sections forindications and operativefindings Which are not?EHRs, Cloned Documents, & Medical Necessity “Cloned documentation does not meet medicalnecessity requirements for coverage of servicesrendered due to the lack of specific, individualinformation.All documentation in the medical record mustbe specific to the patient and her/his situationat the time of the encounterCloning of documentation is considered amisrepresentation of the medical necessityrequirement for coverage of services.Identification of this type of documentation willlead to denial of services for lack of medicalnecessity and recoupment of all overpaymentsmade.”No Rubber Stamp– Eugene J. Winter, M.D., Medical Director for FirstCoast Service Options, Inc.– materials/medicaid/Medicare Document.pdf5
The Foundation Guidelines for Coding AnyProcedure (CPT Introduction) “Select the name of the procedure orservice that accurately identifies theservice performed. Do not select a CPTcode that merely approximates theservice provided. If no such procedureor service exists, then report the serviceusing the appropriate unlisted procedureor service code” “When necessary, modifying orextenuating circumstances are added” “Any service or procedure should beadequately documented in the medrecord”Guidelines for Coding Multiple Procedures All procedure codes (except thosedesignated XXX) include a CPTdefined surgical package:– Local or topical anesthesia– One related E/M encounter on day of (orone day before) the procedure,subsequent to the decision for surgery– Immediate post-op care, includingdictation and communication withfamily and/or other physicians– Evaluation in recovery area– “Typical postoperative follow-up care”What is Included in “ Typical” Follow-Up? “Follow-up care for therapeuticsurgical procedures includes only thatcare which is usually a part of thesurgical service. Complications,exacerbations, recurrence, or thepresence of other diseases of otherdiseases or injuries requiringadditional services should beseparately reported” Be aware (& wary) of the CMS noncompliant variation on this package– Complications ARE included in theirglobal package6
Modifiers When 1 procedure performed on same date,several modifiers may apply (as defined inAppendix A of CPT) Without the appropriate use of modifiers, insurersoftware will bundle all services into a primary code Do not submit codes for two procedures when one isa component of the other Modifiers: -51, -59Commonly Used Procedure Modifiers -22 unusual services: greater than usually required -50 bilateral procedure: Used to identify performingidentical operations on both sides for services thatare not already identified as bilateral in CPT– E.g., 31254.50– 42826 does not need a modifier since the RVU vignettedescribes this as a unilateral procedure -51 multiple procedures: used only when proceduresare not components– Advises insurer software to pay both services– Also triggers (by convention) a 50% reduction on allsecondary procedures (except add-on & -51 mod exempt)Commonly Used Procedure Modifiers -58 performance of a planned or staged procedureduring the post-operative period -59 distinct procedure service: one procedure thatwould normally be a component of another (&therefore not submitted) is being submitted becauseit was appropriate due to different site, differentencounter, separate lesion, etc– Used only when a different modifier not appropriate -62 two co-surgeons performing distinct parts of aprocedure– What is payment policy of Medicare & insurers on thismodifier?– What are the consequences?7
Commonly Used Procedure Modifiers -76 repeat procedure by same physician -77 repeat procedure by another physician -78 return to O.R. for a related procedure duringpost-op period (usually due to unexpected complics) -79 return to O.R. for unrelated procedure duringpost-op pd -80 assistant surgeon– What is payment policy of Medicare & insurers on thiscode?– What are the consequences?Managed Care Non-Compliant Policies forE/M Codes with Procedure Modifiers Some turn off modifier functionality(i.e., pay only one code regardless ofmodifier) Non-compliant bundling edits thatoverride the correctly used modifier– How many CCI edits?– How many Claim Check edits?– Suggest visiting www.CignaForHCP.comQuestions on Principles for Procedures?8
Ear ProceduresEar Wax 101 CPT code 69210– “Removal impacted cerumen” – define?– (separate procedure), one or both ears”– What is the global period designation for this procedure? How should this be coded when performed with another earprocedure (e.g., 69436 – tube placement)? How should this be coded with E/M service– When cerumen is the only reason for the visit?– When there is another problem addressed as well?– What must be documented in the chart for necessity? Compliance problem when every occurrence of wax is “impacted” (this failsto pass the smell test) How to code for patients impacted every two months?Using the Operating Microscope CPT code 92504This is a separate procedureThis has an XXX global designation0.69 RVUsCan 92504 be billed with cerumen removal code?– CPT Asst 7/2005: permissible if required (document medicalnecessity!); not if used routinely Should 92504 be billed for routine ear examination? Under what circumstances is this service billable? What isthe documentation required? CPT Asst (1/2005) advises use .52 modifier if unilateral9
What About the Add-On Code for Usingthe Operating Microscope? “Surgical microscope is employedwhen using the techniques ofmicrosurgery” Code 69990 should be reported (withoutmodifier –51) in addition to the code forthe primary procedure “Do not report code 69990 where use ofthe operating microscope is an inclusivecomponent” Although CPT’s example list of codes notto add 69990 does not include any earoperations, it is not a comprehensive list The RVU vignettes for ear surgery codesinclude use of the operating microscope!69990Tube Insertion Local anesthesia (office): 69433 / .50 bilat General anesthesia (office): 69436 / .50 bilatTube Removal (the 750tube removals) Tube removal in office: E/M Tube removal general anesthesia (unilat): 69424 (1.6RVU) ? Repair, with or without preparation of perf, with orwithout patch: 69610 (7.73 RVUs) ? Myringoplasty: 69620 (12.49 RVU)10
Coding for Acoustic Neuroma This is NOT a “skull basesurgery” The 2 codes that “accuratelyidentify the procedureperformed are– 61526: craniectomy, bone flapcraniotomy, transtemporal(mastoid) for excision ofcerebellopontine angle tumor;”– 61530: “combined withmiddle/posterior fossacraniotomy/craniectomy”Other Ear Questions? Mastoid? Stapes?Nose & Sinus Procedures11
Diagnostic Endoscopy 92511 is treated as a component of 31231 & 31575 31231 is treated as a component of 31575 Interestingly, as of 2004, 31575 has lower RVUvalue (2.99 RVUs) than 31231 (4.68) or 92511 (4.1)– Prior to 2004, 31575 had the higher RVU value– Why? What do we think about this bundling policy from aclinical, coding, & RVU perspective?Epistaxis Codes 30901: control nasal hemorrhage, anterior, simple(limited cautery &/or packing) any method 30903: control nasal hemorrhage, anterior, complex(extensive cautery &/or packing) any method 30905: control nasal hemorrhage, posterior, withpacks &/or cauterization, any method; initial 30906: control nasal hemorrhage, posterior, withpacks &/or cauterization, any method; subsequent Documentation critical to distinguish correct service– As well as showing separate E/M service whenappropriateEpistaxis Coding How do you code the services?– Initial visit for patient with 3 weeks of intermittent nasalbleeding, usually mild but occasionally moderate. Perform & document level 3 initial visit care Identify left anterior bleeding site and control with silver nitratecautery and Surgicel topical pack Codes?– Called to E.R. at 9 PM to see patient who is bleedingbriskly from the left nostril. Remove old packing andplace a full posterior pack Codes?12
Epistaxis Coding How do you code the services:– Initial visit for patient with 3 weeks of intermittent nasalbleeding, usually mild but occasionally moderate. Perform & document level 3 initial visit care Identify left anterior bleeding site and control with silver nitratecautery and Surgicel topical pack Physician documents use of nasal endoscope during evaluationand requests use of code 31238 Codes?Nasal Trauma Operations Closed reduction nasal dorsumClosed reduction nasal septumOpen reduction septumOpen reduction septum with closedreduction dorsum Open reduction septum & dorsum21315 – 2132021337?2133621336 & 21320.5121335Nasal Septum Operations Repair deviated nasal septum Septal dermatoplasty 30520 3062013
Turbinates Physiology– Warming– Humidification– Appropriate airwayresistance (nasalpulmonary reflex)Turbinate Coding Prior to 2006 CPT changes, insurer software often bundledturbinate surgery into sinus surgery, stating that the middleturbinates are part of the ethmoid bone– And choosing to ignore the fact that the inferior turbinates are notpart of the ethmoid bone Coding ambiguities resolved with 2006 semantics, whichdefine the procedures as relating only to the inferiorturbinatesTurbinate Coding CPT procedure codes (changed 2006 to inf turbs)– 30801: cautery and/or ablation, mucosa of inferior turbinates,unilat or bilat, any method; superficial (3.4 rvu)– 30802: intramural (4.92 rvu) (this includes radiofrequency procedures)– 30930: fracture inferior turbinates, therapeutic (3.02 rvu)– 30130: excision inferior turbinate, partial or complete (7.15 rvu)– 30140: submucous resection of inferior turbinate, partial orcomplete, any method (7.68 rvu) 30801, 30802, & 30930 are components of 30130 & 30140 Middle turbinate Rx (non-endoscopic), including conchabullosa, now coded as 30999 unlisted procedure 31240: endoscopic resection concha bullosa; NOT bundledinto 31254 & 31255 per CCI14
Turbinate Coding for Radiofrequency AAO-HNS position:– “For RFA of the turbinates, use CPT 30802, cautery andor ablation, mucosa or turbinates, unilateral or bilateral,any method (separate procedure); intramural”– “Or CPT 30999, unlisted procedure nose”– Code for “submucous resection of turbinates is not thebest suited code, even when the –52 modifier for reducedservices is applied” Comment: this would NOT be a correct code! – the RFA doesnot involve a surgical resection of bone!Commentary: Turbinate Anatomy & Physiology Turbinates swell and contract allthe time as part of the normalalternating nasal cycle –membranes on one side are morecongested that the those on theother side; then it switches With a significantly deviatedseptum, there may becompensatory hypertrophy on thewide open side; this usuallyresolves spontaneously after theseptum is straightened With chronic sinus infection orallergy, the turbinates congest;this usually resolves withresolution (medical or surgical)of the underlying problemCommentary: Turbinate Controversies ENTs who operate on turbinates seem to do so in every case– Including bilateral inferior turbinate surgery with septoplasty– That is, the procedure is performed routinely, WITHOUTDOCUMENTED MEDICAL INDICATIONS Other ENTs (almost) NEVER operate on turbinates Both groups report similar excellent outcomes with theirnasal and sinus procedures There is no evidence to support a medical benefit toroutine turbinate surgery15
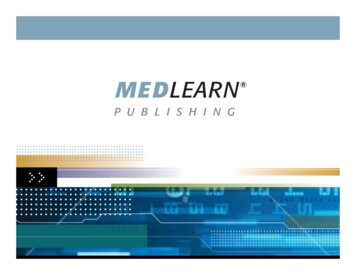
Turbinate Controversies AAO-HNS “Clinical Indicators” state that indications forinferior turbinate surgery must include:– Chronic nasal obstruction due in part to inferior turbinatehypertrophy.– Failure of directed medical management with continued nasalsymptoms (medications, allergy treatment, and duration oftherapy)– Failure of medical treatment of rhinitis medicamentosa.– Symptoms of obstructive sleep apnea The “failure of directed medical management” might beconsidered (particularly if YOU are the patient) to include– Continued obstruction following straightening nasal septum– Continued obstruction following endoscopic sinus surgeryTurbinate Controversies When complications occurfrom turbinate surgery, theycommonly have significantsymptoms, which are chronicand usually cannot beeffectively remedied!– Chronic dryness / crusting– Discharge / PND– Ozena !Surgically removed inferior turbinates bilaterallyTurbinate Controversies That is, from a reviewer’s Opinion: from anperspective, “how can routineauditor’s & coder’sperformance of this procedureperspective, this is notan issue of coding; it is be medically ‘necessary’ whensome physicians achievean issue of medicalsuccessful outcomes withoutnecessityperforming it?”– {The lesson of utilization ofcoronary bypass surgery}16
CPT’s Endoscopic Sinus Surgery Codes Nasal sinus endoscopy, surgical, with––––31254: ethmoidectomy, partial (anterior)31255: ethmoidectomy, total (anterior & posterior)31256: maxillary antrostomy31267: maxillary antrostomy with removal of sinus tissue Note: medically necessary, NOT ROUTINE– 31276: frontal sinus exploration, with or without removal of tissuefrom the frontal sinus– 31287: sphenoidotomy– 31288: sphenoidotomy with removal of sinus tissue Note: medically necessary, NOT ROUTINE– Others for repair CSF leak and orbital decompression These are all unilateral codes – require –50 modifier if bilateralEndoscopic Frontal Sinus (31276) To employ this code, there must beevidence of significant frontal sinuspathology, and significant surgerymust be performed Simply identifying the frontal sinusrecess outlet is insufficient to applythis code Must have documented removal offrontal recess cells and diseasedtissue, or removal of bone betweenfrontal recess & supra-orbitalethmoidEndoscopic Repair of CSF Leak Cerebrospinal fluid leaks may occur spontaneously(rare), following trauma, or following ESS These occur from the bone at the roof of the sinuses, whichseparates sinus from brain CPT 31290: “Nasal/sinus endoscopy, surgical with repair ofcerebrospinal fluid leak, ethmoid region” CPT 31291: “Nasal/sinus endoscopy, surgical with repair ofcerebrospinal fluid leak, sphenoid region” Note: these codes are inclusive of surgical access throughthe ethmoid and sphenoid sinuses17
Potential Insurer Non-Compliance forEndoscopic Sinus Surgery Ignoring –50 modifier in bilateral procedures Bundling inferior turbinate procedures into sinus surgery Bundling nasal septal procedures into sinus surgery(claiming that septum was done only for “exposure”)– MDs need appropriate DOCUMENTATION in the medical recordto support appeal & medical necessity of performing septum– Examples of inadequate documentation of septal status?– Examples of adequate documentation of septal status? Ignoring the 0 day global designation for endoscopic sinussurgery, particularly with regard to debridementsDebridement Controversies CPT code 31237: “Nasal/sinus endoscopy, surgical; with biopsy,polypectomy or debridement (separate procedure)”– 8.63 RVUs– This is a unilateral code. Use –50 modifier if bilateral ENTs who submit for multiple debridements in the post-op period ofESS seem to do so in every case– That is, the procedure is performed routinely, without documented medicalindication other than “routine” post-op care Other ENTs employ 0 – 1 debridement in nearly every case– That is, the procedure appears to be physician specific, not patient specific. Thisfact mitigates against medical necessity Both groups report similar excellent outcomes Contention that mucosal-sparing benefits of micro-debriders eliminatesignificant scarring and therefore reduces indication for debridements There is no evidence to support a medical benefit to frequent routinedebridement surgeryAAO-HNS Survey 2001 60% of respondentsreport usually billingfor 0 – 1 debridements Critique: perhapsmany are performingdebridements & notbilling
30905: control nasal hemorrhage, posterior, with packs &/or cauterization, any method; initial 30906: control nasal hemorrhage, posterior, with packs &/or cauterization, any method; subsequent Documentation critical to distinguish correct service – As well as showing separate E/