Transcription
October 2016Improving Community Health ThroughPolicy ResearchTREATMENT &RECOVERY FORSUBSTANCE USEDISORDERS IN INDIANA 2016 Center for Health Policy (16-H80)IU Richard M Fairbanks School of Public Health at IUPUIIndiana University-Purdue University Indianapolis (IUPUI)1050 Wishard Blvd, 5th floorIndianapolis, IN 46202
The mission of the Center for Health Policy is to conduct research on critical health-related issues andtranslate data into evidence-based policy recommendations to improve community health. The CHP facultyand staff collaborate with public and private partners to conduct quality data driven program evaluation andapplied research analysis on relevant public health issues. The Center serves as a bridge between academichealth researchers and federal, state and local government as well as healthcare and community organizations.Please direct all correspondence and questions to: Center for Health Policy, IU Richard M Fairbanks Schoolof Public Health at IUPUI, 1050 Wishard Blvd, RG5163, Indianapolis, IN 46202; Email: iuchp@iupui.edu;Phone: (317)278-5907.AUTHORSEDIT & LAYOUT2Harold Kooreman, MA, MSWMarion Greene, MPH, PhD(c)Lyndy Kouns
TABLE OFCONTENTS3Executive Summary.4Substance Abuse.4Prevalence of SUDs.5Demographic Characteristics of Persons with SUDs.6Consequences of SUDs.7Health & Social Consequences.7Economic Consequences.8Treatment.8Types of Treatment.8Treatment Admissions.9Demographic Characteristics.9Patterns of Drug Use.11Availability of Formal Treatment Services in Indiana.12Treatment Utilization – Needs and Barriers.14Outcomes of Treatment.15Recovery.19Introduction.19Definitions of Recovery.19Recovery Oriented Systems of Care.19Recovery in Indiana – A Qualitative Analysis.20Introduction.20Study Description.20Data Collection and Analysis.20Participants and Their Organizations.21Perspectives on Recovery.21Organizational-Level Definitions of Recovery.21Organizationa Views on Indiana’s Definition of Recovery.22Recovery Facilitators.23Changing Requirements for SUD Service Grants.23National-Level Policies Related to SUDs.23The Opiate Crisis in Indiana.24Recovery Barriers.24Stigma & Conservativism.24Lack of Awareness & Information.25SUD Service System Structure.25Funding.26Availability of Services.26Recovery Workforce.26Lack of Recovery Advocates.27Policy Recommendations.27Spread Accurate Messages about Addiction & Recovery.27Involve the Recovery Community in Policy Making.28Promote Recovery-Oriented Systems Change.28Support Expansion and Use of Recovery Services.29Follow Best Practices for Recovery.30Support Recovery for Individuals who are Incarcerated.30Enhance Employment Opportunities for Peer Workers.30Conclusions.31References.32
EXECUTIVESUMMARYSUBSTANCEABUSE4Substance abuse is a significant public healthconcern. When drug or alcohol use regularlycauses a person substantial life consequences,he/she has likely transitioned from occasional,potentially problematic, use to having asubstance use disorder (SUD). In 2014, almosthalf a million Hoosiers (8.5%) met the criteriafor SUD.SUDs are associated with significantmorbidity, mortality, and social and economicconsequences. For example, Indiana’s druginduced mortality rate quadrupled from 4.8 per100,000 persons in 2000 to 19.2 per 100,000persons in 2014. The staggering social andeconomic costs of SUDs suggest that moreeffort needs to be placed in not only preventingthe development of SUDs, but also inproviding timely and appropriate treatment foraffected individuals.Indiana had 294 active substance usetreatment providers in 2013. Most of thesetreatment facilities had outpatient treatmentcenters (93.1%); a small percentage providedresidential (10.5%) and hospital inpatient care(12.0%).In 2013, there were nearly 26,000 admissionsto substance abuse treatment programs inIndiana. The substances most frequentlyabused by the state’s substance abuse treatmentpopulation were alcohol (57.3%), marijuana(48.3%), and opiates/synthetics (22.0%).Treatment systems have traditionally used anacute-care approach to address SUDs. The newparadigm proposed by the Substance Abuseand Mental Health Services Administration(SAMHSA) is a continuing-care model. Itacknowledges the long-term nature of SUDsand emphasizes the need for ongoing access toservices built around the concept of recovery.Recovery-oriented systems of care (ROSC)require agencies and providers to develop a fullcontinuum of SUD services. This continuumof services should include not only traditionalinpatient, residential, and outpatient services,but also nontraditional services, such as recoverymaintenance, peer services, and communitybased recovery support services.Key informants interviewed for this studymade policy recommendations to addressexisting barriers and allow for a recoveryoriented system of care to emerge more rapidlyin Indiana. They suggested the creation ofpolicies to:Substance abuse is a significant public healthconcern. The National Household Survey onDrug Use and Health (NSDUH) estimatedthat in 2014 approximately 9.8% of the U.S.population 12 years of age or older usedillicit substances, including nonmedical use ofprescription drugs, and 22.9% of Americansengaged in binge alcohol use in the pastmonth.1 Although the majority of individualswho occasionally participate in risky drinking orillegal substance use never experience seriousconsequences, others may find that over timetheir alcohol or drug use escalates to the pointwhere it impairs their day-to-day functioning.When drug or alcohol use regularly causes aperson substantial life consequences, she orhe has likely transitioned from occasional,potentially problematic use, to having asubstance use disorder (SUD).The American Psychiatric Association(APA)2 describes the primary characteristicof a SUD as continued use of a substance inspite of significant substance-related problems.Individuals with SUDs can have symptoms thatare cognitive, behavioral, and physiological innature. These symptoms result from underlyingchanges in brain circuits or brain chemistryand serve to support ongoing substance use.Examples of symptoms include:1. Promote accurate information about addiction and recovery, using the language orterminology of recovery.2. Mandate inclusion of representatives fromthe recovery community in all aspects ofrecovery-related planning.3. Promote a recovery-oriented system ofcare approach.4. Tie funding to the use and expansion ofrecovery services.5. Require the use of best practices for recovery.6. Provide recovery services for individuals inthe correctional system during incarceration and after they return to the community.7. Improve employment opportunities forpeer recovery workers and integrate theminto organizations that serve individualswho are in recovery from SUDs. having strong drug cravings or urges touse; ignoring responsibilities in order to use; spending more and more time using; developing tolerance (i.e. needing more ofthe drug to achieve the same effect); or
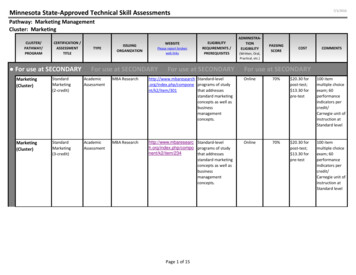
experiencing withdrawal (i.e. having significant physical discomfort when bloodor tissue levels of the drug decline belowa certain threshold).2The APA has discontinued the practice ofusing the categories of substance abuse andsubstance dependence to demarcate the severityof a SUD,i preferring to view them as falling ona continuum of impairment ranging from mildto moderate to severe.This technical report will discuss prevalencerates of SUDs both nationally and in Indiana;examine trends and critical issues related tothe treatment of SUDs; describe the conceptof recovery and how incorporating recoveryinto interventions for individuals with SUDscan result in better long-term outcomes; andprovide a qualitative analysis of how recoveryis being addressed in Indiana, along with policyrecommendations to include a recovery-relatedfocus into Indiana’s SUD service system.Prevalence of SUDsThe NSDUH provides prevalence estimates forSUD at both the national and state level.iiAccording to findings from their 2014 survey,21.5 million U.S. citizens, or 8.1% of thepopulation 12 years of age or older, had metthe criteria for any SUD in the past year. Ofthose, over 17.2 million met the criteria for analcohol use disorder (6.5%), 6.9 million met thecriteria for an illicit-drug-use disorder (2.6%),and 2.7 million (1.0%) exhibited signs of both.Past-year prevalence rates were similar in Indianawith 464,108 Hoosiers (8.5%) meeting criteriafor any SUD; 365,826 (6.7%) having an alcoholuse disorder; 152,882 (2.8%) having an illicitdrug-use disorder; and 54,601 (1.0%) estimatedto have both. Since 2004, there has been littlechange in either the national or state SUDprevalence rate (see Figure 1).Figure 1. Changes in Prevalence Rates of SUDs over Time (NSDUH %0.0%Any SUD - 20108.9%20118.4%20128.3%20138.4%20148.1%Any SUD- INAlcohol SUD - USAlcohol SUD - 2%6.6%7.0%8.8%6.7%7.0%8.5%6.5%6.7%Illicit Drug SUD - USIllicit Drug SUD - 2.8%3.0%2.7%2.4%2.7%2.5%2.7%3.0%2.6%2.8%Alcohol use disorder is the most prevalentSUD in the U.S. In terms of illicit drugs,marijuana use disorder is the most common,impacting 4.2 million (1.6%) citizens 12 andolder annually followed by SUDs tied to theuse of prescription opioid analgesics, whichaffect 1.9 million persons (0.9%) annually.iii5SUDs related to cocaine, heroin, hallucinogens,inhalants, stimulants, tranquilizers, and sedativestogether affect less than one percent of the U.S.population over 12 years of age.1 Estimates forthe prevalence of SUDs resulting from the useof specific illicit substances are not currentlyavailable for Indiana.Until 2013, substance abuse was defined as a maladaptive pattern of substance use leading to clinically significantimpairment or distress and manifested by at least one of the following symptoms occurring within a 12-month period:recurrent substance use resulting in failure to fulfill major role obligations; recurrent substance use in situations inwhich it is physically hazardous; recurrent substance-related legal problems; or continued use despite persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance. Substance dependencewas defined as a maladaptive pattern of substance use leading to clinically significant impairment or distress and demonstrated by three or more of the following in the same 12-month period: tolerance; withdrawal; taking a substanceoften in larger amounts or over a longer period than was intended; or having a persistent desire or unsuccessful effortsto cut down or control substance use (APA, 2004).To maintain consistency across time, the NSDUH continues to use the DSM-IV definition for SUDs which distinguishes between substance abuse and substance dependence.
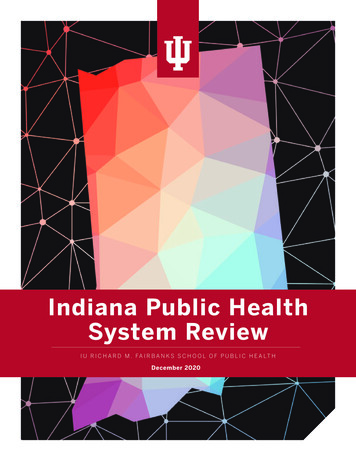
National prevalence estimates based on theNational Epidemiologic Survey on Alcoholand Related Conditions-III (NESARC-III) relyon the DSM-V definition for SUDs. Basedon the NESARC-III, in 2013 13.9% and 3.9%of US adults 18 years or older met criteria fora past year alcohol or illicit-drug-use disorderrespectively. The NESARC-III’s estimatesare significantly higher than the 7.1% and2.6% estimates for alcohol or illicit-drug-usedisorders for persons 18 and older reportedby the NSDUH. The difference between theestimates is attributed to underdiagnosing ofSUDs, particularly substance dependence, whenusing the DSM-IV criteria.3-5Demographic Characteristics of Personswith SUDsThe prevalence of SUDs in the U.S. variedaccording to demographic characteristics suchas age, gender, and race/ethnicity. Young adultswere significantly more likely to experience thesedisorders than any other age group; males hada higher prevalence of SUDs than females; andnon-Hispanic Blacks had a significantly higherprevalence of illicit substance use disorders thanother racial/ethnic groups (see Tables 1A and1B).6Table 1A. Differences in Prevalence Rates of Alcohol and Illicit Drug Use Disorders by Age, Gender, andRace/Ethnicity (NSDUH, 2014)Alcohol UseDisorders1NAge Group Under 18678,000Illicit Drug UseDisorders1(%)NIllicit Drugs ORAlcohol(%)N(%)Both Illicit Drugsand )297,000(1.2)18-254,285,000 (12.3)2,320,000(6.6)5,696,000 )6,491,000 )6,326,000(7.4)422,000(0.5) 422,0002,655,000(3.4) 13,731,000 (10.7)(1.9) 7,749,000 cor Latino11,059,000(6.5)4,133,000(2.4) ,180,000(2.8)3,614,000(8.5)481,000(1.1)Table 1B. Differences in Prevalence Rates of Alcohol and Illicit Drug Use Disorders by Age (NESARC-III,2013)Alcohol UseDisorders1NAge Group(%)N(%)Illicit Drugs ORAlcoholN(%)Both Illicit Drugsand AlcoholDisordersN(%)18-2930-445,834,000 (11.2)4,772,000 (7.9)3,197,0001,548,000(6.2)(2.6)8,104,000 (15.6)5,751,000 4)1,114,000(2.5)25,000( 0.1) 656Illicit Drug UseDisorders1(1.8)(0.9)
Grant et al.3,4 reported higher prevalenceestimates for alcohol use and drug usedisorders based on data from the NESARCIII. However, the pattern of prevalence rateswas similar to the NSDUH with males andyounger individuals having higher rates ofalcohol use and drug use disorders. In terms ofrace, Grant et al.3 determined that White andNative Americans had similar rates of alcoholuse disorders and both rates were higherthan those for other racial/ethnic groups.The rate of drug use disorders was estimatedto be similar for Non-Hispanic Whites, NonHispanic Blacks, and Native Americans and allwere significantly higher than rates of drug usedisorders among Asian/Pacific Islanders andHispanics.4 Prevalence estimates of alcohol useand other substance use disorders based ondemographic characteristics are not availablefrom either the NSDUH or the NESARC-III atthe state level.Consequences of SUDsHealth & Social ConsequencesSubstance use disorders are associated withsignificant morbidity, mortality, and social andeconomic consequences. Individuals who haveSUDs are at increased risk for numerous healthproblems compared to the general population,with the na
Please direct all correspondence and questions to: Center for Health Policy, IU Richard M Fairbanks School of Public Health at IUPUI, 1050 Wishard Blvd, RG5163, Indianapolis, IN 46202; Email: iuchp@iupui.edu; Phone: (317)278-5907. Harold Kooreman, MA, MSW Marion