Transcription
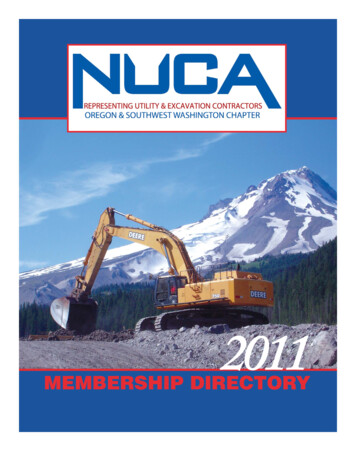
UnderstandingAnterior Segment OCTWhat Does Anterior Segment OCT Do?Clinical Applications ofAnterior Segment OCTSarah Moyer, CRA, OCT-CDirector of Ophthalmic ImagingKenneth L. Cohen, MDProfessor of OphthalmologyKittner Eye CenterDepartment of OphthalmologyUniversity of North Carolina at ChapelHillSchool of Medicine 2-dimensional cross section image of theanterior segment– Conjunctiva– Cornea– Anterior chamber– Iris/Angle– Lens– Sclera VendorsHow does AS-OCT work?Technical aspectsWhat does AS-OCT measure?How is AS-OCT used clinically?No financial interestImage Anterior Segment Low magnification imageImage Anterior Segment High magnification imageAnterior Segment OCT optigenCourtesy of Sunita Sayeram and Joseph VanceHeidelberg SpectralisOpko Spectral OCT SLOCourtesy of OpkoCourtesy of John CarpentierCourtesy of Tim SteffensHandheld OCTSpectralis- AAO 2011?Spectral OCT SLORT-Vue with CAMiVueAAO 2011?Visante and Cirrus
Optovue RT-Vue with CAMZeiss CirrusZeiss Stratus4mm scan lengthInternal opticsSoftware upgrade neededCourtesy of Bruno Bertoni, CRA, OCT-C and Tamera Davis, CRAThis is not FDA approved!Courtesy of OptovueZeiss Stratus1 Week After Phaco and1-Piece Posterior Chamber IOLZeiss VisanteCourtesy of ZeissCourtesy of Alexis Smith, OCT-C, CRADislocated IOLIOL in the Capsular BagTecnis One-PieceCauses of the Dislocted IOL IOL not in capsular bag but in ciliarysulcus Ruptured zonules Hole in posterior capsule Broken haptic Crimped haptic
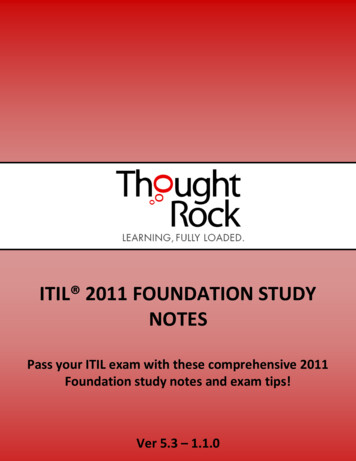
Relationship Betweenthe IOL and the Capsular Bag?Relationship Betweenthe IOL and the Capsular Bag?Ultrasound Biomicroscopy (UBM) 2-dimensional cross-sectional image ofanterior segment Multiple meridians How can I obtain a 2-dimensionsal crosssectional image of the anterior segment ofthe eye?Anterior segment OCTImmersion B-scan ultrasound4 o’clockIOL haptic truncatedDislocated IOL UBM4:004:00IOL haptic truncatedWhat Are the Technical Aspectsof Anterior Segment OCT?OCT Versus UBMOCT Versus UBM 2-dimensional cross-sectional imagesof anterior segment Multiple meridians OCT provides more fine detail andmagnified image OCT non-contact versus UBM contact(water bath) OCT more useful to the anteriorsegment surgeon because easy to use MD or photographer performs UBM Photographer performs OCT OCT and UBM require communicationbetween MD and photographerAnatomic structure(s)LocationMagnificationImaging protocolOCT Specifications ComparisonTime and Spectral Domain imeSpectralTimeSpectralSLD Wavelength8208401310840Scan SpeedA-Scans/sec40027,0002,00026,000Axial Resolution 10 μm5 μm18 μmTransverse Res20 μm15 μm60 μmScan Depth2mm2mm6mmOptical Power750 μW 725 μW 6500 µW 750µWVisante is designed specifically for Anterior Segment OCT.5.0µm15µm2-2.3mm
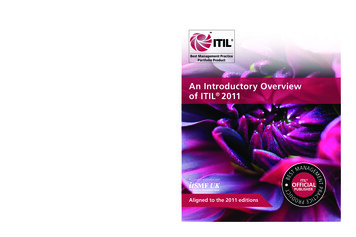
Anterior Segment SpecificationsSpecificationsVisanteRT-VueSLD Wavelength1310840Optical Power 6500 µW750µWAnterior Segment SpecificationsSpecificationsVisanteRT-VueSLD Wavelength1310840Higher Wavelength allows for deeperscan depth and longer scan lengthScan Depth3mm,6mm2-2.3mmMore scan depth is able to imagecornea to lensScan Length10mm,16mm1-2,1-6Longer scan length can image limbusto limbus.OCT Image ComparisonStratus 10mmVisante 16mmRT-Vue 8mmRT-Vue 1mm6x163x10The shorter wavelength of light and lower optical power make itpossible for the SD technology to also image the retinaWhy is Scan Length Important? DSEKStratus 3mmGraphic modifiedfrom Zeiss graphicThe longer wavelength of light and stronger optical power allow TDtechnology to penetrate deeper into the angle.2x62x1Longer scan length gives overviewShorter scan length gives more resolutionSlipped DSEK ComparisonLonger vs Shorter Scan Length16mm10mm6mm6mmVisante 10mmCirrus 4mmScleral Contact Lens– Limbus to Limbus Imaging is necessary toensure proper attachment of the donor tissue Scleral Contact Lens Fitting– Needed to view the entire lens in one image Glaucoma– Able to measure both angles from one image.Courtesy Team Doheny EyeGlaucomaWhy Do I Image the Cornea? Analysis of new corneal transplantationtechniques Management of postop complications Document healing of surgical incisions Plan operations Management of corneal ulcers Evaluate extent of tumors of the ocular surface Measurements of the anterior segmentTextFuchs Corneal Dystrophy Fuchs dystrophyInherited disease of corneal endotheliumEndothelium dysfunctionalCorneal edemaVision decreases Guttae obscure endotheliumSpecular microscopy
Corneal EndotheliumFunction Pumps H2O out of the cornea into theanterior chamber Keeps corneal stroma at 78% H2O Transparent at thickness 550 μ Pachymetry is a measurement of cornealthickness Gauges health of corneaPenetrating KeratoplastyEpithelial defectOCT to Monitor Health of DSEK PositionAttachment of graft to recipientQuality of interfaceCorneal thicknessFuchs DystrophyTreatmentCorneal Edema Hazy corneaCorneal foldsPenetrating keratoplasyFull thickness recipient cornea removedFull thickness donor cornea sutured into place360 full thickness corneal wound1 year for visual rehabilitationIrregular healing of wound results invariable visual results due to astigmatismDSEK: Descemet’s StrippingEndothelial KeratoplastyPenetrating Keratoplasty Diseased endothelium removed (30 μ) Donor endothelium and stroma inserted( 150 μ) Small incision (5 mm) Rapid healing and visual rehabilitation in30 to 60 daysIrregular healing of full thickness incisionDSEKDSEK 4 Weeks Post-op1D1038 μ1W618 μ1M687 μUltrasound pachymetry 549 μ
Ultrasound Pachymetry IncorrectDSEK 4 Weeks PostopVisante Flap Tool Normal thickness 550 μ 30 μ endothelium and Descemet’smembrane removed 180 μ donor cornea implanted Pachymetry after DSEK should be at least700 μCorneal thickness 769 μDetached DSEK 1 Day PostopAnterior Segment OCTDSEK Reattachment DESK attachment 360 would indicateprimary donor failureRequire graft replacement DSEK detachmentReattach graft with airMalpositioned DSEKMalpositioned DSEK1 day postop7 weeks postop1 week postop4.5 months postopAutomated Global Pachymetry180 meridian770 μ90 meridianSlipped inferiorly
Available Measurements Corneal ThicknessPachymetry Data PointsGlobal Pachymetry– 16 line scansCorneal thicknessAnterior chamber depthAnterior chamber angleIncisionTumor– 2048 data points in one mapPachmate Pachymetry1 data pointCorneal thickness 769 μAnterior Chamber DepthPre-Op3.61 mmMeasuring AnglesMeasuring Angles AOD: angle-opening distance TIA: trabecular-iris angle TISA: trabecular-iris space areaPost-Op5.16 mmClear Corneal IncisionClear Corneal IncisionDescemet’s detachmentEndothelial gapeEndothelial misalignmentEpithelial misalignmentEpithelial gapeLoss of coaptationTumors / CystsUnable to use measurement features in Raw Mode
ArtifactsMust understand what is real andwhat is artifact on the scanArtifacts Corneal ReflexCorneal ReflexInverted Image (in Spectral Domain)ShadowingImage AveragingAlgorithm Failure– Pachymetry: Corneal surface lines– Pachymetry: LidsInverted ImageSpectral DomainShadowing?ShadowingImage AveragingAveragingMeasuring with AveragingEnhanced High Res Cornea ModeEnhanced High Res Cornea ModeTop: Non-averaged ScansBottom: Averaged Scans
DewarpingEnhanced ModeAlgorithm FailureDue to Corneal Surface LinesAlgorithm Failure Due to LidsAlgorithm Failure Due to LidsinferiorsuperiorAlgorithm FailureDue to Corneal Surface LinesAlgorithm FailureDue to Corneal Surface LinesVisualize Depth of Corneal ScarVisualize Depth of Corneal ScarHow Else Does AnteriorSegment OCT Help Me WithPatients?DSEK with a scarExcellent detail of cornea
Ocular Surface TumorsCorneal and ConjunctivalIntraepithelial NeoplasiaCorneal and ConjunctivalIntaepithelial NeoplasiaFungal Corneal UlcerAnterior Chamber Depth Does the tumor extend into the cornea,sclera, and anterior chamber angle? Plan operative procedureInfectious Keratitis Hazy cornea Difficult to see extent of corneal involvement Monitor response to medical therapyPre-op Phaco IOL CalculationAnterior Chamber DepthIOLMaster Important for IOL calculation Theoretical prediction formula: Haigis Required to predict the post-opposition of the IOL Correct IOL power can be inserted 0.05 mm ACD error 0.03 diopterIOL power errorIrregular PupilGonioscopyVisante4.10 mmACD difference 1.8 mm 1.08 dioptersPeripheral anterior synechiaeHoles in iris
Coverage Status for Anterior Segment OCTAs of September 2009OCTNHVTWAPASMTMENDMNMAORWISDIDNYMIWYWhat Are the Issues for BillingAnterior Segment OCT?PAIANENVUTCOCAILOHINMORIDCDEWVVAKSNJ CTKYMDNCTNAZUBMOKNMSCARMSHITXALGALAFLAKCoverage and payment for 0187T (28 states)Coverage based on medical necessity (4 states)Coverage may be gained after MAC transition (8 states)PASNormal ciliary bodyIn progress of requesting coverage via KOLS (4 states)Carrier declined to cover (6 states)Billing 0187-T: Temporary Code, Medicarereimbursement varied according to Medicareregions 92132: AMA established CPT code, Medicarecovers this code. Some states may have aLocal Medical Review Policy (LMRP) where onlyspecific diagnosis are covered. SCANNING COMPUTERIZED OPHTHALMIC DIAGNOSTICIMAGING, ANTERIOR SEGMENT, WITH INTERPRETATION ANDREPORT, BILATERAL 364.71 POSTERIOR SYNECHIAE OF IRIS364.72 ANTERIOR SYNECHIAE OF IRIS364.73 GONIOSYNECHIAE364.74 ADHESIONS AND DISRUPTIONS OF PUPILLARY MEMBRANES364.75 PUPILLARY ABNORMALITIES364.76 IRIDODIALYSIS364.77 RECESSION OF CHAMBER ANGLE OF EYE364.81 FLOPPY IRIS SYNDROME364.82 PLATEAU IRIS SYNDROME364.89 OTHER DISORDERS OF IRIS AND CILIARY BODY365.02 ANATOMICAL NARROW ANGLE BORDERLINE GLAUCOMA365.20 PRIMARY ANGLE-CLOSURE GLAUCOMA SPECIFIED365.21 INTERMITTENT ANGLE-CLOSURE GLAUCOMA365.22 ACUTE ANGLE-CLOSURE GLAUCOMA365.23 CHRONIC ANGLE-CLOSURE GLAUCOMA365.24 RESIDUAL STAGE OF ANGLE-CLOSURE GLAUCOMA365.41 GLAUCOMA ASSOCIATED WITH CHAMBER ANGLE NOMALIES \365.42 GLAUCOMA ASSOCIATED WITH ANOMALIES OF IRIS365.43 GLAUCOMA ASSOCIATED WITH OTHER ANTERIOR SEGMENTANOMALIES365.44 GLAUCOMA ASSOCIATED WITH SYSTEMIC SYNDROMESMedicare leads to . Cigna Government Services: (TN, NC, ID)Highmark Medicare Services: (PA, DC, MD, DE, NJ)National Government Service, Inc.: (IN, KY, NY, CT)First Coast Service Options, Inc.: (FL, Puerto Rico, USVirgin Islands)NHIC, Corp.: (ME, MA, VT, NH, RI) Palmetto GBA: (HI, CA, NV) Noridian Administrative Services (WA, OR, AK, AZ,UT, WY, MT, ND, SD) Cahaba (TN, MS, AL, GA)Billing Codes Billing Codes 190.0 190.4224.0 .59364.60364.61364.62364.63364.64364.70364.71 Billing Codes 03371.71371.72371.73379.31PHACOLYTIC GLAUCOMAPSEUDOEXFOLIATION GLAUCOMAGLAUCOMA ASSOCIATED WITH OTHER LENS DISORDERSGLAUCOMA ASSOCIATED WITH UNSPECIFIED OCULAR DISORDERGLAUCOMA ASSOCIATED WITH PUPILLARY BLOCKGLAUCOMA ASSOCIATED WITH OCULAR INFLAMMATIONSGLAUCOMA ASSOCIATED WITH VASCULAR DISORDERS OF EYEGLAUCOMA ASSOCIATED WITH TUMORS OR CYSTSGLAUCOMA ASSOCIATED WITH OCULAR TRAUMAHYPERSECRETION GLAUCOMAGLAUCOMA WITH INCREASED EPISCLERAL VENOUS PRESSUREAQUEOUS MISDIRECTIONOTHER SPECIFIED GLAUCOMAHYPOPYON ULCERMYCOTIC CORNEAL ULCERPERFORATED CORNEAL ULCERCENTRAL OPACITY OF CORNEACORNEAL ECTASIADESCEMETOCELECORNEAL STAPHYLOMAAPHAKIAMALIGNANT NEOPLASM OF EYEBALL EXCEPT CONJUNCTIVA CORNEARETINA AND CHOROIDMALIGNANT NEOPLASM OF CORNEABENIGN NEOPLASM OF EYEBALL EXCEPT CONJUNCTIVA CORNEARETINA AND CHOROIDBENIGN NEOPLASM OF CORNEAESSENTIAL OR PROGRESSIVE IRIS ATROPHYIRIDOSCHISISPIGMENTARY IRIS DEGENERATIONDEGENERATION OF PUPILLARY MARGINMIOTIC CYSTS OF PUPILLARY MARGINDEGENERATIVE CHANGES OF CHAMBER ANGLEDEGENERATIVE CHANGES OF CILIARY BODYOTHER IRIS ATROPHYIDIOPATHIC CYSTS OF IRIS AND CILIARY BODYIMPLANTATION CYSTS OF IRIS AND CILIARY BODYEXUDATIVE CYSTS OF IRIS OR ANTERIOR CHAMBERPRIMARY CYST OF PARS PLANAEXUDATIVE CYST OF PARS PLANAADHESIONS OF IRIS UNSPECIFIEDPOSTERIOR SYNECHIAE OF IRISBilling Codes 379.31 APHAKIA379.32 SUBLUXATION OF LENS379.33 ANTERIOR DISLOCATION OF LENS379.39 OTHER DISORDERS OF LENS996.51 MECHANICAL COMPLICATION OF PROSTHETIC CORNEAL RAFT996.53 MECHANICAL COMPLICATION OF PROSTHETIC OCULAR LENSPROSTHESIS996.69 INFECTION AND INFLAMMATORY REACTION DUE TO OTHERINTERNAL PROSTHETIC DEVICE IMPLANT AND RAFT
Thanks for your help!UNC DoctorsBruce Baldwin, OD, Ph.DCraig Fowler, MDDavid Russell, MDGeorge Escaravage, MDGraham Lyles, MDIsaac Porter, MDJonathan Dutton, MDKenneth Cohen, MDUNC PhotographersDebra Cantrell, COARona Lyn Esquejo-Leon,CRAPhotographersDoheny Eye InstituteBruno Bertoni, CRA, OCT-CTamera Davis, CRAHenry Ford Health SystemsAlexis Smith, OCT-C, CRAUniversity of California- DavisEllen Redenbo, CRA, ROUBKarishma ChandraUniversity of Florida Eye InstituteJohn Carpentier, CRA, OCT-CWills Eye InstituteSandor Ferenczy, CRASusan ProiettaBioptigenEric Buckland, Ph.DSunita Sayeram, MSJoseph VanceHeidelbergTim SteffensOptovueBill DillworthMark ThomasCarl Denis, CRAZeissGreg HoffmeyerRick TorneyTracy MooreGary Michalec, CRA, COACherri RitterKenneth L. Cohen, MDProfessor of OphthalmologySarah Moyer, CRA, OCT-CDirector of Ophthalmic Imagingsmoyer@gmail.comKittner Eye Center, University of North Carolina Chapel Hill, NC
Kittner Eye Center Department of Ophthalmology University of North Carolina at Chapel Hill School of Medicine Clinical Applications of Anterior Segment OCT No financial interest What Does Anterior Segment OCT Do? 2-dimensional cross section image of the anterior segment – Conjunctiva –Cornea – Anterior chamber – Iris/Angle – Lens .