Transcription
Original ContributionsHerding Cats: TheChallenges of EMRVendor SelectionSamuel W. McDowell, PhD, Regi Wahl, and James Michelson, MDA B S T R A C TThe selection of an enterprise-wide electronic medical record(EMR) by a medical center is a major undertaking that willdefine its future clinical processes for many years. Theparameters that drive the selection include the clinicalrequirements, the financial needs of the medical center, thegeographic setting, the need for outreach into the community,and an analysis of the existing and predicted flow ofinformation and work within the clinical systems.K E Y W O R D SElectronic medical ical processesThe evolution of an electronic medical record (EMR) in a medical centervaries depending on the preexisting medical record system. In some instances, theprocess may represent only an incremental change in a partially developed computerized EMR. In other cases, it comescloser to a revolution, as it is part of acomplete overhaul of a minimally computerized medical record system.In the latter circumstance, the implementation of the EMR involves muchmore than simply automation of preexisting processes. Strategically it requiresanalysis of, and change to, the underlying clinical information processes.Tactically, the transformation from amixed, predominantly paper record to anenterprise-wide EMR consists of threemain stages: First, and most important, is the enlistment of the medical center communityin the process. The management level(clinical chiefs, administration) andstaff level (physicians, nurses, ancillarymedical, clerical) personnel must beinvolved in developing the strategicgoals and the implementation process. The second tactical objective is selection of a vendor for the EMR. The final tactical goal is the successfulimplementation of the new EMR. Thisarticle describes this developmentprocess, with an emphasis on criticalgeneralizable components/milestonesof the process and potential barriersto success.Current Situation AnalysisFletcher Allen Health Care (FAHC) is atertiary care academic medical center,located in Burlington, Vermont. The service area includes most of Vermont,fringes of New Hampshire, and portionsof upstate New York. Fletcher Allen inthe last year had approximately 23,000inpatient visits and 398,000 hospital outpatient visits. FAHC employs approximately 6,000 employees, which includes700 medical staff and 2,000 nurses.Fletcher Allen Health Care’s coreclinical information system is primarilyan in-house developed legacy system,with results review provided throughOACIS (Open Architecture ClinicalInformation System). It has interfaces toJournal of Healthcare Information Management — Vol. 17, No. 363
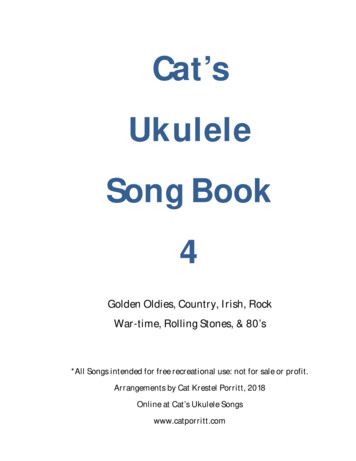
Original ContributionsFigure 1. FAHC Clinical Information Systems Strategycurrent technology ancillary systems suchas IDX-Rad in radiology and SunQuest inthe laboratory.The existing systems are highly interfaced, and poorly integrated. Real-timeclinician performance monitoring is lacking, and system conformance is highlymanual and redundant. There is no significant integration among these information systems, with separate log-insrequired for each. In addition, the vendor of OACIS has ceased supportingtheir product due to company dissolution following bankruptcy. There is nocomputer-based clinical documentationsystem for outpatient care, and only asemi-automated legacy system exists inthe inpatient setting.In part due to the impending demiseof the results-reporting system support,FAHC began in the summer of 2000 toexplore the options for introducing anenterprise-wide EMR. From a clinical perspective, such an EMR had to fulfill threestrategic goals: The first goal was to select a vendorthat will provide the core clinical systems necessary for Fletcher Allen toachieve its clinical and strategic objectives. These were: (1) supporting the64work of Fletcher Allen clinicians; (2)supporting the work of non-FletcherAllen clinics and hospitals, some ofwhom are affiliated, the remainder ofwhich are primarily referral sources ofpatients; and (3) supporting theVermont community with a statewidelongitudinal patient healthcare record. The second goal was to create an enterprise clinical patient record with theattributes (Figure 1) identified by theComputer-Based Patient Record Institutefor content and functionality. It wasunderstood that any plan for implementing the system would encompasssignificant capital requirements, operating requirements, and process changesover a long-term rollout. The third goal in selecting and implementing a system was to initiate achange management process withinthe clinical arena. By this, we are really talking about two different issues:First, the identification of critical clinical process flows so they can be modeled, replicated, and improved; andsecond, the actual management ofimplementing the workflow changesnecessary to launch the EMR. To agreat extent, Fletcher Allen has a man-Journal of Healthcare Information Management — Vol. 17, No. 3ual, paper-based clinical care process.We did not want to simply replicatethe existing paper processes on thecomputer. In analyzing the workflowprocesses, a balance has to be struckbetween fulfilling the perceived needsof the users and actually changingthose processes for the better. Doingso requires the active involvement ofall the constituencies concerned sothat the best possible design isachieved, and to ensure the acceptance of the final product by all themajor groups of users.Return on Investment ExpectationsAs with any such expensive undertaking, it was necessary to explicitly addressthe issue of the expected return on investment (ROI) for an enterprise-wide EMR.ROI analysis fell into three categories —financial, clinical, and operational.The financial returns are tangible, butdifficult to measure. Financial improvements are related to: (1) reduced lengthof stay, (2) cost reductions associatedwith risk reduction of adverse drugevents, (3) reduced pharmaceutical costsderived from having information available at the time it is needed, (4) expanded technical capability and support ofspecialty services as needed, (5)improved case-mix analysis to improvereimbursement that is based on averageseverity index of cases treated at FAHC,(6) improved billing accuracy and chargecapture, and (7) improved materials management and supply chain management.The second category of ROI expectation is clinical, which has two components: improved patient care and standardized care. Reduced adverse drugevents and improved decision makingcan directly demonstrate improvedpatient care. An underlying decision support (DS) capability that evolves overtime should provide a substantialimprovement in care delivered, both interms of quality and cost. The secondclinical component, standardized care, isa way of managing outcomes by use ofevidence-based clinical guidelinesembedded in the decision support component of the EMR.
Original ContributionsThe third ROI expectation is operational, which is specific to FAHC. FletcherAllen has two clinical systems — onelegacy system and OACIS. Both productsneed to be replaced due to their inabilityto provide adequate clinical support inthe present healthcare environment.While this is not an overriding driver ofthe replacement decision, it is a strongjustification for investing in an integratedcore clinical information system.Underlying Assumptions in Selectionof an EMRBefore considering any vendors orproducts, considerable effort was expended developing the overall structure of anEMR that would fulfill our functionalrequirements. What resulted (Figure 1)defined the elements critical to our concept and the inter-relationships that werenecessary. The core of the EMR is anenterprise-wide clinical data repositorythat is closely linked to the major documentation, order-entry, and schedulingcomponents. This permits disseminationof timely, accurate data throughout themedical care process, and provides theopportunity for effective decision support.Data, in the form of text and images,is fed into the core through standardinterfaces to laboratory, radiology, pharmacy, and other systems. In many cases,the data exchange between the ancillarysystems and the core is bi-directional inorder to provide for clinical alerts, decision support, clinical task creation, etc.The clinical core is accessible to clinicians through multiple modalities (workstations, PDAs, etc.).The initial stages of this process highlighted the fact that the success of animplementation strategy would be dependent on clearly articulated clinical/organizational objectives. Identification of theseaims would keep the organizationfocused and help guide the vendor selection process. The prime clinical goal is toimprove care. Commitment to this resulted in the functional requirements of coreclinical system integration to facilitate theprovision of accurate, real-time clinicaldata, as well as a decision-support mechanism to identify and promote optimalclinical decisions.Figure 2. Voting TableOther important clinical goals includeimproving the satisfaction of patientswith their encounters at FAHC, improvethe ease of clinical documentation andsystem use by the clinicians, improvecost accounting methodology withrespect to clinical (e.g., critical pathways,best practices implementations) and nonclinical functions (e.g., supply chainmanagement, revenue cycle management), and develop an effective mechanism to deliver healthcare to a geographically dispersed community.Initiation of the EMR SelectionProcessOnce the medical center leadershipidentified the potential need for a significant change in the health informationmanagement system, the InformationServices Department was tasked todevelop a conceptual framework for anEMR that would be appropriate forFAHC. The first activity following thiswas a presentation of the program scopeto corporate officers of FAHC. Corporateofficers are the executive committee ofFletcher Allen consisting of chief executive officer, chief nursing officer, chiefmedical officer, chief operating officer,chief information officer, senior vicepresident of human resources, andsenior vice president of business andplanning, who make all policy and significant operational decisions.Once approved by the corporate officers, the concept was presented to theStrategic Management Committee, whichconsists of the corporate officers plus thedepartment chairs of the medical departments. Fletcher Allen, as an academichospital, is affiliated with the Universityof Vermont College of Medicine. Themedical faculty has joint responsibility tothe College of Medicine and to FletcherAllen. It was important to engage theclinical and business leadership as earlyas possible in the decision-makingprocess to enlist their aid in progressingwith the project.A small decision team was established,which would be the focus of the ongoing analysis and vendor selection decision process. It consisted of a representative team of leadership from within theorganization, which included the chiefmedical officer, the chief nursing officer,the chief information officer, and severalphysicians spanning inpatient and outpatient practices, specialty, and generalmedicine. Two of the physicians also hadtraining in informatics. In addition, theJournal of Healthcare Information Management — Vol. 17, No. 365
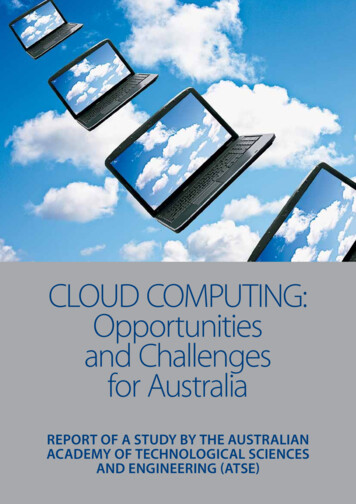
Original ContributionsTable 1. RFP Subject Areas1.0Description of System2.0Technical Section3.0Application Section4.0General Questions5.0Specifications andWarranties6.0Scope of License7.0Deliverables and SiteRequirements8.0Implementation 9.0Training10.0Support11.0Personnel12.0Preliminary Cost Estimate13.0Payment14.0Due Diligence15.0Contract Issuesteam had a registered nurse informaticist,a senior technical architect, and a seniorproject manager to ensure adherence tobudgets, schedules, and project objectives. The project had continuing highvisibility with the corporate leadershipthroughout the selection process.Three other groups within FletcherAllen worked with the key leadership,and provided analysis as they participated in the process. First there was a nursing informatics group, consisting ofapproximately 15 Fletcher Allen nurseswhose primary objective was to reviewthe clinical aspects of the vendors’ products. Second, there was participationfrom business and clinical departmentleadership as needed. In addition to clinical leaders, leadership from humanresources, budget and finance, patientfinancial services, registration, and scheduling were also involved in the process.Third, all Fletcher Allen employees wereinvited to, and participated in, variouspresentations. While it was understoodthat this was not a voting process,employee feedback was strongly encouraged and presented as a way for everyone involved to contribute to the decision as well as help outline the clinicaland functional requirements for the recommended system.As a complement to the expertise within Fletcher Allen, a number of externalresources were used. Among those wereVHA Consulting, who provided high-levelinsight about clinical vendors; TheGartner Group, who provided domainexpertise as well as process advice;Accenture (formerly AndersenConsulting), who helped with implementation strategies and domain expertise;and KLAS, who provided extensive analysis of vendors’ service and support capabilities. On an ad hoc basis, FAHC alsodiscussed its directions and mutual opportunities with other OACIS customers.*The value of identifying the strategicissues at the inception of the project hadtwo major benefits. First, it highlightedexisting process issues necessary to beresolved prior to implementation. Second,it generated an initial implementationstrategy consisting of pro forma projectplans, which remained a useful baselineagainst which to evaluate vendor proposals throughout the selection process.Selection MilestonesSeven significant milestones wereidentified in the selection process:1. Establishing the decision team.While the membership of the teamevolved over time, the core of theteam remained constant.2. Establishing and agreeing upon theselection criteria. This had beendone at the beginning of the project,but it was not until toward the endof the project that serious consideration was given to the relative rankingof criteria. Establishing the importance of each criterion, along withrefining the criteria, permitted meaningful comparisons between vendors.3. Developing a pro forma clinical strategy as well as an implementation4.5.6.7.strategy. This helped to substantiallyfocus the team’s thoughts and gavethe team a baseline against which toevaluate the vendor offerings.Conducting product demonstrations.Demonstrations occurred at severaljunctures throughout the process,each with a different focus.Distributing requests for proposal.Five addenda to the RFP wereissued for further clarification on significant issues, requiring documented responses and cross-vendor comparison. As the vendors becameaccustomed to the format of the RFP,they were able to respond rapidly,frequently within a few days.Conducting site visits. There wereseveral types of site visits, includingvisits to customer sites and vendorheadquarters.Recommending a vendor. The finalmilestone was a recommendation tothe corporate officers with the vendor of choice.Preliminary Vendor ScreeningCriteriaThe initial screening of vendors wasaimed at getting to a short list as quickly aspossible. A request for proposal (RFP) wasdistributed to only four vendors. FAHCstarted with a small group of vendors, eachof whom met five key requirements:1. Product employed current technology2. Product was a fully integrated suiteof core clinical components3. Applications were available for inpatient, ambulatory, and outreachenvironments4. Vendor demonstrated financial andmanagement stability5. Vendor had experience with largetertiary care and academic customersA short list of five vendors was developed using the five criteria, with theassistance of the external consultants.Each of the consultants had vendors thatthey felt met our criteria. By comparingall the recommendations from all the*OACIS is a product that is substantially a development tool used for developing clinical information systems. The OACIS vendor made a business decision to nolonger develop or support their product. Fletcher Allen worked with other OACIS customers who had similar needs, to share experiences and better prepare usfor the vendor analysis and selection process.66Journal of Healthcare Information Management — Vol. 17, No. 3
Original Contributionsconsultants, it was fairly easy to identifythe five vendors who were representedmost often.A comprehensive RFP was issuedearly in the process. The RFP was verydirective in the format in which the vendors were asked to respond, and verydirective in the time frame for turningthe RFP around. The vendors didrespond to the RFP in a very short period of time (six weeks), and they allresponded exactly to the format andstructure that was requested. In so doing,FAHC’s comparison of vendors’ responses across proposals was facilitated.At the same time a detailed technicalRFP was issued as an addendum to theoriginal RFP. Over the course of the following months several RFP addendawere issued when fairly specific questions /issues required a lengthy and/orwritten response.Product DemonstrationsThree types of product demonstrationsoccurred. The first type of productdemonstration was called a “drive-by.”This was held at Fletcher Allen in theemployee cafeteria. Over a five-day period, each vendor had one day wherethey were allowed to set up in one corner of the cafeteria and essentially hold aone-vendor exhibit. The exhibits wereunstructured, in that the vendors wereallowed to conduct product demos,demonstrate product futures, distributepromotional materials, and display banners. The exhibits resulted in a numberof key benefits, including: (1) it allowedFAHC employees to see, hear, and touchwhat a new system might look like, and(2) it facilitated building a comfort leveland relationship with the vendor at thestart of what would be a long process.Note that these demonstrations werethe vendor’s first and last unstructuredsales presentations.The second type of product demonstration was a controlled on-site presentation at Fletcher Allen. The presentations were two-day sessions. The firstday was a scripted corporate presentation. FAHC provided the vendor with ascript, which they were required to follow. Although it allowed them to make aTable 2. Vendor Assessment Summary Subset2.1 Expert Engine2.1 Expert EngineRating2.2 MedicalDictionary2.2 MedicalDictionary Rating2.3 ResearchVendor 1 Rules/alerts(assumes OE) – Yes drug-allergy drug-drug drug-disease critical paths clinical guidelines usability of clinicalworkstation goodVendor 2 Smartsets Rules/alerts(assumes OE) –pre-made Smartsets drug-allergy drug-drug lab results critical paths clinical guidelines Health maintenancenotification engine usability of clinicalworkstation excellentVendor 3 CA-DB Expert Rules/alerts(assumes OE) –Simple only drug-allergy drug-drug lab results critical paths / clinical guidelines / Health maintenancenotificationengine / usability of clinicalworkstation fair174 SNOMED/RT, ICD9,CPT, LOINC, Medcin clinical chart OE billing/E&M coding Medcin, SNOMED,ICD9, CPT, NIC, NOC,NANDA, UMLS, LOINC clinical chart OE billing/E&M coding 47 Database structure/language Oracle Query language SQL Database structure/language – M/Cache Query language –SQL Ease of customreporting good,Crystal reports UNMC (12k), ICD9,SNOMED, NANDA,DRG. Note: Medcin,etc cannot beincorporated CPT add-on OE - billing/E&M coding 3rd party1 Database structure/language –proprietary Query language –(proprietary) Ease of customreporting Poor2
Vendor Selection ABSTRACT The selection of an enterprise-wide electronic medical record (EMR) by a medical center is a major undertaking that will define its future clinical processes for many years.The parameters that drive the selection in