Transcription
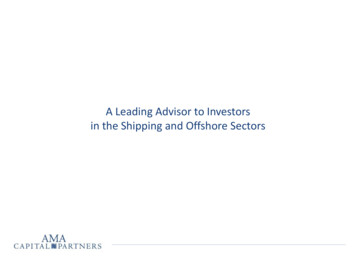
AMA/Specialty Society Relative Value Update Committee (RUC)Final Vote Release – CPT 2023Every year, the RUC holds three meetings to review CPT codes that are either new, revised or consideredpotentially misvalued by either the Centers for Medicare and Medicaid Services (CMS) or the RUC’s ownprocess of identification performed by the Relativity Assessment Workgroup (RAW). In April 2012, the RUCapproved a measure to release the final total RUC voting counts for each code reviewed during the mostrecently completed cycle. The release of these voting records will occur each year following CMSpublication.For the CPT 2023 cycle, the RUC convened meetings on April 21-24, 2021, October 6-9, 2021 and January12-15, 2022 and the Committee’s final recommendations for each meeting are submitted approximatelyone month after the close of each meeting. For the CPT 2023 cycle, CMS will publish all the RUCrecommendations for 2023 in the Medicare Physician Payment Schedule Proposed Rule.Further information about the RUC and its processes can be found at:www.ama-assn.org/about-us/rucBelow is a list of definitions and descriptions of RUC processes to help in the understanding the votinginformation published on the following pages: CPT Code and Long Descriptor: These first two columns simply state each individual CPT codes andLong Descriptor.Pre-Facilitation (Yes/No): Prior to each meeting, RUC members undergo a rigorous review of eachCPT code’s recommendation as submitted by the specialty society(ies). If significant concerns areraised by either the reviewing RUC members or the specialty society(ies) a request for prefacilitation may occur. Pre-facilitation meetings are assigned to a specific subset of RUC membersand Advisors called a facilitation committee (described below) and can occur either by phone or onsite, prior to the presentation of the code(s) during the RUC meeting. During the pre-facilitationmeetings, issues are discussed and the specialty society(ies) have the opportunity (but have noobligation) to revise their recommendations.Specialty Work RVU modified prior to or during Presentation (Yes/No): This field indicateswhether or not the specialty society(ies) involved in surveying a specific code have revised theirwork RVU recommendation prior to during the presentation of the code to the RUC. Thesemodifications are typically made after review of pre-facilitation committee discussion (see above)or after consideration of RUC reviewer comments.Specialty Work RVU passed by RUC (Yes/No): This field indicates whether or not the initiallypresented work RVU recommendation, as presented to the RUC by the specialty society(ies), wasapproved.Specialty Work RVU facilitated by RUC (Yes/No): Each meeting, three facilitation committees areestablished. Each committee consists of a subset of RUC members, specialty society Advisors and amember of the non-MD/DO Health Care Professional Advisory Committee (HCPAC) who, when acode does not meet the required two-third vote for approval, meet with the appropriate specialtysociety(ies) to reach consensus on a revised work RVU and direct practice expense. At theconclusion of a facilitation committee meeting, a report is written providing a rationale for the1
revised recommendations and the RUC again votes to either approve or disapprove these workRVU recommendations.Specialty Work RVU modified by RUC process (Yes/No): This field indicates if, for any reason, thespecialty society(ies) RVU recommendations from initial submissions were modified by the RUCprocess. Modifications can happen for any number of reasons: 1) a pre-facilitation committeemeeting could offer alternative suggestions that the specialties include; 2) comments made duringthe review process or at the table during the presentation of the code could result in modifications;3) a facilitation committee meeting can reach consensus on revised work RVUs.Final RUC Vote- work RVU: This field indicates the final RUC vote total for each code. These votetotals represent the final RUC determinations on each code. CPT code RVU recommendations couldhave changed substantially from the original specialty societies’ recommendation through any ofthe mechanisms laid out in the fields listed in the table and described above. There are 29 votingmembers on the RUC. A vote total may not add up to 29 for two reasons: 1) a voting member canabstain and/or 2) a voting member may not be present at the table during the vote. The RUCrequires that at least 2/3 of the member voting must approve the recommendation in order for itto be submitted to CMS. A quorum, consisting of 17 member of the RUC, must be present toconduct any business.Final RUC Vote- Direct Practice Expense: This field indicates the final RUC vote total for each code’sdirect practice expense inputs (clinical labor, supplies and equipment) as recommended by thePractice Expense (PE) Subcommittee. As with the work RVU recommendations, direct PE inputrecommendations could have changed substantially from the original specialty societies’recommendation. The PE subcommittee meets for a full day prior to the RUC proceeding andreviews specialty society submissions for direct PE inputs and makes recommendations directly tothe RUC. Following each vote on work RVUs, the RUC holds a separate vote to accept the direct PEinputs as modified and/or approved by the PE Subcommittee. The same voting protocol for workRVUs apply to direct PE inputs.2
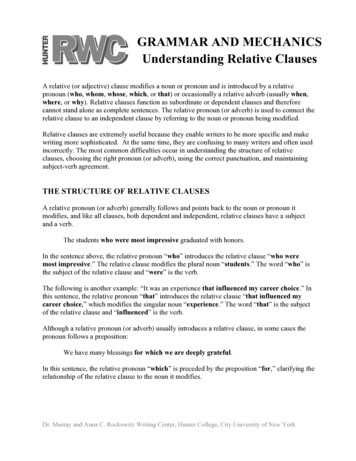
RUC Vote Totals – CPT 2023 Summary(Physician Work ONLY)VoteTotalPercentageof VoteTotalInstancesNumber ofVote 23-5*22-721-820-941121132%1%1%1%1%1%2%46% of all RUCRecommendations to CMSfor CPT 2023 were basedon unanimous votes of theCommittee*Represents vote totals in which a RUC member abstained from vote.3
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC157X1Implantation of absorbable mesh or otherprosthesis for delayed closure of defect(s) (ie,external genitalia, perineum, abdominal wall) dueto soft tissue infection or traumaYesNoNoYesYes29-029-015851Removal of sutures or staples requiring anesthesia(ie, general anesthesia, moderate sedation)YesNoNoYesYes29-029-0158X1Removal of sutures or staples not requiringanesthesia (List separately in addition to E/M code)1YesN/AN/AN/AN/AN/A29-0158X2Removal of sutures and staples not requiringanesthesia (List separately in addition to E/M code)1YesN/AN/AN/AN/AN/A29-022630Arthrodesis, posterior interbody technique,including laminectomy and/or discectomy toprepare interspace (other than for decompression),single interspace; lumbarYesNoYesNoNo28-129-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 1 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC22632Arthrodesis, posterior interbody technique,including laminectomy and/or discectomy toprepare interspace (other than for decompression),single interspace; each additional interspace (Listseparately in addition to code for sis, combined posterior or posterolateraltechnique with posterior interbody techniqueincluding laminectomy and/or discectomy sufficientto prepare interspace (other than fordecompression), single interspace; lumbarYesNoYesNoNo27-229-022634Arthrodesis, combined posterior or posterolateraltechnique with posterior interbody techniqueincluding laminectomy and/or discectomy sufficientto prepare interspace (other than fordecompression), single interspace; each additionalinterspace and segment (List separately in additionto code for primary procedure)YesNoYesNoNo24-529-022857Total disc arthroplasty (artificial disc), anteriorapproach, including discectomy to prepareinterspace (other than for decompression), singleinterspace, lumbarYesN/AN/AN/AN/A29-029-04Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 2 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotes22869Insertion of interlaminar/interspinous processstabilization/distraction device, without opendecompression or fusion, including imageguidance when performed, lumbar; single levelYesNoYesNoNo26-329-022870Insertion of interlaminar/interspinous processstabilization/distraction device, without opendecompression or fusion, including imageguidance when performed, lumbar; second level(List separately in addition to code for primaryprocedure)YesNoYesNoNo28-129-0228XXTotal disc arthroplasty (artificial disc), anteriorapproach,including discectomy to prepare interspace (otherthanfor decompression); second interspace, lumbar(List separately inaddition to code for primary procedure)YesN/AN/AN/AN/A29-0N/A27446Arthroplasty, knee, condyle and plateau; medialOR lateral compartmentYesNoYesNoNo28-129-02, 4PreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUCNotes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 3 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC27447Arthroplasty, knee, condyle and plateau; medialAND lateral compartments with or without patellaresurfacing (total knee arthroplasty)YesNoYesNoNo29-029-030468Repair of nasal valve collapse withsubcutaneous/submucosal lateral wall implant(s)YesNoYesNoNo29-028-1338X3Percutaneous pulmonary artery revascularizationby stent placement, initial; normal nativeconnections, unilateralYesNoYesNoNo27-2N/A338X4Percutaneous pulmonary artery revascularizationby stent placement, initial; normal nativeconnections, bilateralYesNoYesNoNo28-1N/A338X5Percutaneous pulmonary artery revascularizationby stent placement, initial; abnormal utaneous pulmonary artery revascularizationby stent placement, initial; abnormal connections,bilateralYesNoYesNoNo28-1N/ANotes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 4 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC338X7Percutaneous pulmonary artery revascularizationby stent placement, each additional vessel orseparate lesion, normal or abnormal connections(list separately in addition to code for ous arteriovenous fistula creation, upperextremity, single access of both the peripheralartery and peripheral vein, including fistulamaturation procedures (eg, transluminal balloonangioplasty, coil embolization) when performed,including all vascular access, imaging guidanceand radiologic supervision and s arteriovenous fistula creation, upperextremity, separate access sites of the peripheralartery and peripheral vein, including fistulamaturation procedures (eg, transluminal balloonangioplasty, coil embolization) when performed,including all vascular access, imaging guidanceand radiologic supervision and interpretationYesNoYesNoNo29-029-037X01Repair of nasal valve collapse with low energy,temperature-controlled (ie, radiofrequency)subcutaneous/submucosal remodelingYesNoYesNoNo25-428-1Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 5 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotes42XXXDrug induced sleep endoscopy; with dynamicevaluation of velum, pharynx, tongue base, andlargynx for evaluation of sleep disorderedbreathing; flexible, odenoscopy, flexible, transoral;diagnostic, including collection of specimen(s) bybrushing or washing, when performed gogastroduodenoscopy, flexible, transoral;with deployment of intragastric bariatric denoscopy, flexible, transoral;with removal of intragastric bariatric balloon(s)YesNoYesNoNo29-029-049436Delayed creation of exit site from embeddedsubcutaneous segment of intraperitoneal cannulaor catheterYesN/AN/AN/AN/AN/A29-01PreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUCNotes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 6 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC49X01Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),initial including placement of mesh or otherprosthesis, when performed total length ofdefect(s); less than 3 cm, reducibleYesNoYesYesNo26-329-049X02Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),initial including placement of mesh or otherprosthesis, when performed total length ofdefect(s); less than 3 cm, incarcerated orstrangulatedYesNoYesYesNo27-229-049X03Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),initial including placement of mesh or otherprosthesis, when performed total length ofdefect(s); 3 cm to 10 cm, reducibleYesNoYesYesNo28-129-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 7 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC49X04Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),initial including placement of mesh or otherprosthesis, when performed total length ofdefect(s); 3 cm to 10 cm, incarcerated orstrangulatedYesNoNoYesYes29-029-049X05Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),initial including placement of mesh or otherprosthesis, when performed total length ofdefect(s); greater than 10 cm, reducibleYesNoNoYesYes29-029-049X06Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),initial including placement of mesh or otherprosthesis, when performed total length ofdefect(s); greater than 10 cm, incarcerated orstrangulatedYesNoNoYesYes29-029-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 8 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC49X07Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),recurrent, including placement of mesh or otherprosthesis, when performed total length ofdefect(s); less than 3 cm, reducibleYesNoYesYesNo29-029-049X08Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),recurrent, including placement of mesh or otherprosthesis, when performed total length ofdefect(s); less than 3 cm, incarcerated orstrangulatedYesNoYesYesNo27-229-049X09Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),recurrent, including placement of mesh or otherprosthesis, when performed total length ofdefect(s); 3 cm to 10 cm, reducibleYesNoYesYesNo28-129-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 9 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC49X10Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),recurrent, including placement of mesh or otherprosthesis, when performed total length ofdefect(s); 3 cm to 10 cm, incarcerated orstrangulatedYesNoNoYesYes29-029-049X11Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),recurrent, including placement of mesh or otherprosthesis, when performed total length ofdefect(s); greater than 10 cm, reducibleYesNoNoYesYes29-029-049X12Repair of anterior abdominal hernia(s) (ie,epigastric, incisional, ventral, umbilical, spigelian),any approach (ie, open, laparoscopic, robotic),recurrent, including placement of mesh or otherprosthesis, when performed total length ofdefect(s); greater than 10 cm, incarcerated orstrangulatedYesNoNoYesYes29-029-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 10 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC49X13Repair of parastomal hernia, any approach (ie,open, laparoscopic, robotic), initial or recurrent,including placement of mesh or other prosthesis,when performed; reducibleYesNoNoYesYes29-029-049X14Repair of parastomal hernia, any approach (ie,open, laparoscopic, robotic), initial or recurrent,including placement of mesh or other prosthesis,when performed; incarcerated or strangulatedYesNoNoYesYes29-029-049X15Removal of mesh or other prosthesis at the time ofinitial or recurrent anterior abdominal hernia repairor parastomal hernia repair, any approach (ie,open, laparoscopic, robotic) (List separately inaddition to code for primary procedure)YesNoYesYesNo29-029-050080Percutaneous nephrolithotomy or pyelolithotomy,lithotripsy, stone extraction, antegradeureteroscopy, antegrade stent placement andnephrostomy tube placement, when performed,including imaging guidance; simple (eg, stone[s]up to 2 cm in single location of kidney or renalpelvis, nonbranching stones)YesNoNoNoYes28-129-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 11 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC50081Percutaneous nephrolithotomy or pyelolithotomy,lithotripsy, stone extraction, antegradeureteroscopy, antegrade stent placement andnephrostomy tube placement, when performed,including imaging guidance; complex (eg, stone[s] 2 cm, branching stones, stones in multiplelocations, ureter stones, complicated anatomy)YesNoYesNoNo23-629-055821Prostatectomy (including control of postoperativebleeding, vasectomy, meatotomy, urethralcalibration and/or dilation, and internalurethrotomy); suprapubic, subtotal, 1 or 2 stagesYesNoYesYesNo29-029-055831Prostatectomy (including control of postoperativebleeding, vasectomy, meatotomy, urethralcalibration and/or dilation, and internalurethrotomy); retropubic, subtotalYesNoYesYesNo29-029-055866Laparoscopy, surgical prostatectomy, retropubicradical, including nerve sparing, includes roboticassistance, when performedYesNoNoYesYes29-029-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 12 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC558XXLaparoscopy, surgical prostatectomy, simplesubtotal (including control of postoperativebleeding, vasectomy, meatotomy, urethralcalibration and/or dilation, and internalurethrotomy), includes robotic assistance, whenperformedYesNoNoYesYes29-029-063020Laminotomy (hemilaminectomy), withdecompression of nerve root(s), including partialfacetectomy, foraminotomy and/or excision ofherniated intervertebral disc; 1 interspace, cervicalYesNoYesNoNo29-029-063030Laminotomy (hemilaminectomy), withdecompression of nerve root(s), including partialfacetectomy, foraminotomy and/or excision ofherniated intervertebral disc; 1 interspace, lumbarYesNoYesNoNo29-029-063035Laminotomy (hemilaminectomy), withdecompression of nerve root(s), including partialfacetectomy, foraminotomy and/or excision ofherniated intervertebral disc; each additionalinterspace, cervical or lumbar (List separately inaddition to code for primary procedure)YesNoYesNoNo29-0N/ANotes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 13 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC630XXLaminectomy, facetectomy, or foraminotomy(unilateral or bilateral with decompression of spinalcord, cauda equina and/or nerve root[s] [eg, spinalor lateral recess stenosis]), during posteriorinterbody arthrodesis, lumbar; single vertebralsegment (List separately in addition to code forprimary procedure)YesNoYesNoNo29-029-064400Injection(s), anesthetic agent(s) and/or steroid;trigeminal nerve, each branch (ie, ophthalmic,maxillary, mandibular)YesNoYesNoNo27-229-064405Injection(s), anesthetic agent(s) and/or steroid;greater occipital nerveYesNoYesNoNo27-229-064408Injection(s), anesthetic agent(s) and/or steroid;vagus nerveYesNoYesNoNo27-229-064415Injection(s), anesthetic agent(s) and/or steroid;brachial plexus, including imaging guidance, whenperformedYesNoYesNoNo20-929-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editorial Panel4 - RUC recommended referral to next RUC meeting5 - The RUC was unable to provide a recommendation due to the lack of clarity on the purpose, use of and reporting of the code.CPT five-digit codes, two-digit modifiers, and descriptions only are copyright by the American Medical Association.Page 14 of 49
RUC Vote Totals – CPT 2023CPTCodeCPT Long DescriptorNotesPreSpecialty workInitiallySpecialtySpecialtyFinalFinal RUCFacilitation RVU modifiedpresentedwork RVUwork RVURUCVote: PEprior to orSpecialty work facilitated by modified byVote:DirectduringRVU passed byRUCRUC process Work RVUCostspresentationRUC64416Injection(s), anesthetic agent(s) and/or steroid;brachial plexus, continuous infusion by catheter(including catheter placement) including imagingguidance, when performedYesNoYesNoNo27-229-064417Injection(s), anesthetic agent(s) and/or steroid;axillary nerve, including imaging guidance, , anesthetic agent(s) and/or steroid;suprascapular nerveYesNoYesNoNo27-229-064420Injection(s), anesthetic agent(s) and/or steroid;intercostal nerve, single levelYesNoYesNoNo27-229-064421Injection(s), anesthetic agent(s) and/or steroid;intercostal nerve, each additional level (Listseparately in addition to code for n(s), anesthetic agent(s) and/or steroid;ilioinguinal, iliohypogastric nervesYesNoYesNoNo27-229-0Notes Legend1 - Reviewed for direct PE inputs only2 - RUC recommended carrier pricing3 - RUC recommended referral to CPT Editori
AMA/Specialty Society Relative Value Update Committee (RUC) Final Vote Release - CPT 2023 . approved a measure to release the final total RUC voting counts for each code reviewed during the most recently completed cycle. The release of these voting records will occur each year following CMS publication. For the CPT 2023 cycle, the RUC .