Transcription
Principles of AdolescentSubstance Use Disorder Treatment:A Research-Based Guide
Principles of AdolescentSubstance Use Disorder Treatment:A Research-Based GuideThis publication is in the public domain and may be used or reproduced inits entirety without permission from NIDA. Citation of the source is appreciated.
NIDA wishes to thank the following individuals for theirhelpful comments during the review of this publication:Tina Burrell, M.A., Washington State Department of Social and Health ServicesConnie Cahalan, Missouri Department of Mental HealthBarbara Cimaglio, Vermont Department of HealthMichael L. Dennis, Ph.D., Chestnut Health SystemsRochelle Head-Dunham, M.D., Louisiana Department of Health and HospitalsScott W. Henggeler, Ph.D., Medical University of South CarolinaSharon Levy, M.D., M.P.H., Children’s Hospital BostonKenneth J. Martz, Psy.D., CAS, Pennsylvania Department of Drug and Alcohol ProgramsKathy Paxton, M.S., West Virginia Bureau for Behavioral Health and Health FacilitiesPaula D. Riggs, M.D., University of Colorado School of Medicine
ContentsFROM THE DIRECTOR.1I.INTRODUCTION .2II. PRINCIPLES OF ADOLESCENT SUBSTANCE USE DISORDER TREATMENT. 81. Adolescent substance use needs to be identified and addressed as soon as possible. 92. Adolescents can benefit from a drug abuse intervention even if they are not addicted to a drug. 93. Routine annual medical visits are an opportunity to ask adolescents about drug use. 94. Legal interventions and sanctions or family pressure may play an important role in gettingadolescents to enter, stay in, and complete treatment.95. Substance use disorder treatment should be tailored to the unique needs of the adolescent. 96. Treatment should address the needs of the whole person, rather than just focusing on hisor her drug use.107. Behavioral therapies are effective in addressing adolescent drug use. 108. Families and the community are important aspects of treatment. 109. Effectively treating substance use disorders in adolescents requires also identifying andtreating any other mental health conditions they may have.1010. Sensitive issues such as violence and child abuse or risk of suicide should be identifiedand addressed. 1111. It is important to monitor drug use during treatment. 1112. Staying in treatment for an adequate period of time and continuity of care afterward are important. 1113. Testing adolescents for sexually transmitted diseases like HIV, as well as hepatitis B and C,is an important part of drug treatment. 11III. FREQUENTLY ASKED QUESTIONS .121.Why do adolescents take drugs? .132.What drugs are most frequently used by adolescents? .133.How do adolescents become addicted to drugs, and which factors increase risk?. 144.Is it possible for teens to become addicted to marijuana?.145.Is abuse of prescription medications as dangerous as other forms of illegal drug use?. 156.Are steroids addictive and can steroid abuse be treated?.157.How do other mental health conditions relate to substance use in adolescents?. 168.Does treatment of ADHD with stimulant medications like Ritalin and Adderall increaserisk of substance abuse later in life?.169.What are signs of drug use in adolescents, and what role can parents play in getting treatment?. 1610. How can parents participate in their adolescent child’s treatment? . 1711. What role can medical professionals play in addressing substance abuse(including abuse of prescription drugs) among adolescents?.1712. Is adolescent tobacco use treated similarly to other drug use?. 1813. Are there medications to treat adolescent substance abuse? . 1814. Do girls and boys have different treatment needs? .1815. What are the unique treatment needs of adolescents from different racial/ethnic backgrounds?. 1916. What role can the juvenile justice system play in addressing adolescent drug abuse?. 1917. What role do 12-step groups or other recovery support services play in addictiontreatment for adolescents?.19
IV. TREATMENT SETTINGS.20Outpatient/Intensive Outpatient.21Partial Hospitalization.21Residential/Inpatient Treatment.21V. EVIDENCE-BASED APPROACHES TO TREATING ADOLESCENT SUBSTANCEUSE DISORDERS.22BEHAVIORAL APPROACHES.23Adolescent Community Reinforcement Approach (A-CRA).23Cognitive-Behavioral Therapy (CBT).24Contingency Management (CM).24Motivational Enhancement Therapy (MET) .24Twelve-Step Facilitation Therapy.24FAMILY-BASED APPROACHES.25Brief Strategic Family Therapy (BSFT).25Family Behavior Therapy (FBT).25Functional Family Therapy (FFT).26Multidimensional Family Therapy (MDFT).26Multisystemic Therapy (MST).26ADDICTION MEDICATIONS.26Opioid Use Disorders.27Alcohol Use Disorders.27Nicotine Use Disorders.28RECOVERY SUPPORT SERVICES.28Assertive Continuing Care (ACC).28Mutual Help Groups.29Peer Recovery Support Services.29Recovery High Schools.29TREATMENT REFERRAL RESOURCES.31REFERENCES.32
From the DirectorSince its first edition in 1999, NIDA’s Principles of Drug Addiction Treatmenthas been a widely used resource for health care providers, families, and othersneeding information on addiction and treatment for people of all ages. But recentresearch has greatly advanced our understanding of the particular treatmentneeds of adolescents, which are often different from those of adults. I thus amvery pleased to present this new guide, Principles of Adolescent Substance UseDisorder Treatment, focused exclusively on the unique realities of adolescentsubstance use—which includes abuse of illicit and prescription drugs, alcohol,and tobacco—and the special treatment needs for people aged 12 to 17.The adolescent years are a key window for both substance use and thedevelopment of substance use disorders. Brain systems governing emotion andreward-seeking are fully developed by this time, but circuits governing judgmentand self-inhibition are still maturing, causing teenagers to act on impulse, seek new sensations, and beeasily swayed by their peers—all of which may draw them to take risks such as trying drugs of abuse.What is more, because critical neural circuits are still actively forming, teens’ brains are particularlysusceptible to being modified by those substances in a lasting way—making the development of asubstance use disorder much more likely.Addiction is not the only danger. Abusing drugs during adolescence can interfere with meeting crucialsocial and developmental milestones and also compromise cognitive development. For example, heavymarijuana use in the teen years may cause a loss of several IQ points that are not regained even if userslater quit in adulthood. Unfortunately, that drug’s popularity among teens is growing—possibly due in partto legalization advocates touting marijuana as a “safe” drug. Nor do most young people appreciate thegrave safety risks posed by abuse of other substances like prescription opioids and stimulants or newlypopular synthetic cannabinoids (“Spice”)—and even scientists still do not know much about how abusingthese drugs may affect the developing brain.These unknowns only add to the urgency of identifying and intervening in substance use as early aspossible. Unfortunately, this urgency is matched by the difficulty of reaching adolescents who need help.Only 10 percent of adolescents who need treatment for a substance use disorder actually get treatment.Most teens with drug problems don’t want or think they need help, and parents are frequently blind toindications their teenage kids may be using drugs—or they may dismiss drug use as just a normal part ofgrowing up.Historically the focus with adolescents has tended to be on steering young people clear of drugsbefore problems arise. But the reality is that different interventions are needed for adolescents atdifferent places along the substance use spectrum, and some require treatment, not just prevention.Fortunately, scientific research has now established the efficacy of a number of treatment approachesthat can address substance use during the teen years. This guide describes those approaches, as wellas presents a set of guiding principles and frequently asked questions about substance abuse andtreatment in this age group. I hope this guide will be of great use to parents, health care providers, andtreatment specialists as they strive to help adolescents with substance use problems get the help theyneed.Nora D. Volkow, M.D.DirectorNational Institute on Drug AbusePrinciples of Adolescent Substance Use Disorder Treatment: A Research-Based Guide 1
I.Introduction2 Principles of Adolescent Substance Use Disorder Treatment: A Research-Based Guide
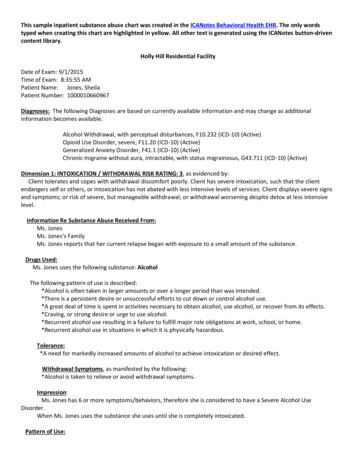
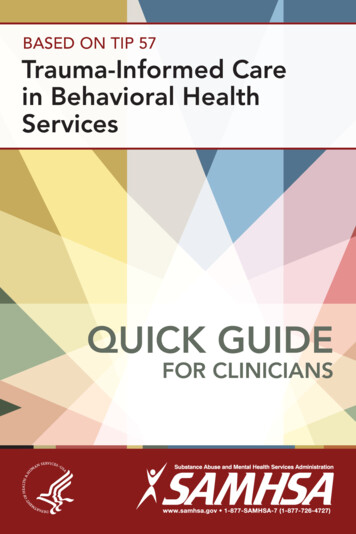
People are most likely to beginabusing drugs*—includingtobacco, alcohol, and illegaland prescription drugs—during adolescence and youngadulthood.‡ By the time they are seniors,almost 70 percent of high school students willhave tried alcohol, half will have taken an illegaldrug, nearly 40 percent will have smoked acigarette, and more than 20 percent will haveused a prescription drug for a nonmedicalpurpose.1 There are many reasons adolescentsuse these substances, including the desirefor new experiences, an attempt to deal withproblems or perform better in school, and simplepeer pressure. Adolescents are “biologicallywired” to seek new experiences and takerisks, as well as to carve out their own identity.Trying drugs may fulfill all of these normaldevelopmental drives, but in an unhealthyway that can have very serious long-termconsequences.Many factors influence whether an adolescenttries drugs, including the availability of drugswithin the neighborhood, community, and schooland whether the adolescent’s friends are usingthem. The family environment is also important:Violence, physical or emotional abuse, mentalillness, or drug use in the household increasethe likelihood an adolescent will use drugs.Finally, an adolescent’s inherited geneticvulnerability; personality traits like poor impulsecontrol or a high need for excitement; mentalThe adolescent brain is often likenedto a car with a fully functioning gaspedal (the reward system) but weakbrakes (the prefrontal cortex).*The brain continues to develop through early adulthood. Mature brain regions at eachdevelopmental stage are indicated in blue. The prefrontal cortex (red circles), which governsjudgment and self-control, is the last part of the brain to mature.Source: PNAS 101:8174–8179, 2004.health conditions such as depression, anxiety,or ADHD; and beliefs such as that drugs are“cool” or harmless make it more likely that anadolescent will use drugs.2The teenage years are a critical window ofvulnerability to substance use disorders,because the brain is still developingand malleable (a property known asneuroplasticity), and some brain areas areless mature than others. The parts of thebrain that process feelings of reward andpain—crucial drivers of drug use—are the firstto mature during childhood. What remainsincompletely developed during the teen yearsare the prefrontal cortex and its connectionsto other brain regions. The prefrontal cortex isresponsible for assessing situations, makingsound decisions, and controlling our emotionsand impulses; typically this circuitry is notmature until a person is in his or her mid-20s(see figure, above).The adolescent brain is often likened to a carwith a fully functioning gas pedal (the rewardsystem) but weak brakes (the prefrontalcortex). Teenagers are highly motivated topursue pleasurable rewards and avoid pain,In this guide, the terms drugs and substances are used interchangeably to refer to tobacco, alcohol, illegal drugs, and prescription medications usedfor nonmedical reasons.‡ Specifying the period of adolescence is complicated because it may be defined by different variables, and policymakers and researchers maydisagree on the exact age boundaries. For purposes of this guide, adolescents are considered to be people between the ages of 12 and 17.Principles of Adolescent Substance Use Disorder Treatment: A Research-Based Guide 3
but their judgment and decision-makingskills are still limited. This affects their abilityto weigh risks accurately and make sounddecisions, including decisions about usingdrugs. For these reasons, adolescents area major target for prevention messagespromoting healthy, drug-free behavior andgiving young people encouragement and skillsto avoid the temptations of experimenting withdrugs.3Most teens do not escalate from trying drugsto developing an addiction or other substanceuse disorder;* however, even experimentingwith drugs is a problem. Drug use can bepart of a pattern of risky behavior includingunsafe sex, driving while intoxicated, or otherhazardous, unsupervised activities. And incases when a teen does develop a pattern ofrepeated use, it can pose serious social andhealth risks, including: school failure problems with family and other relationships loss of interest in normal healthy activities impaired memory increased risk of contracting an infectiousdisease (like HIV or hepatitis C) via riskysexual behavior or sharing contaminatedinjection equipment mental health problems—includingsubstance use disorders of varying severity the very real risk of overdose deathHow drug use can progress to addiction.Different drugs affect the brain differently, buta common factor is that they all raise the levelof the chemical dopamine in brain circuits thatcontrol reward and pleasure.The brain is wired to encourage life-sustainingand healthy activities through the releaseof dopamine. Everyday rewards duringadolescence—such as hanging out withfriends, listening to music, playing sports,*Despite popular belief, willpower aloneis often insufficient to overcome anaddiction. Drug use has compromisedthe very parts of the brain that make itpossible to “say no.”and all the other highly motivating experiences forteenagers—cause the release of this chemical inmoderate amounts. This reinforces behaviors thatcontribute to learning, health, well-being, and thestrengthening of social bonds.Drugs, unfortunately, are able to hijack this process.The “high” produced by drugs represents a floodingof the brain’s reward circuits with much moredopamine than natural rewards generate. Thiscreates an especially strong drive to repeat theexperience. The immature brain, already strugglingwith balancing impulse and self-control, is morelikely to take drugs again without adequatelyconsidering the consequences.4 If the experienceis repeated, the brain reinforces the neural linksbetween pleasure and drug-taking, making theassociation stronger and stronger. Soon, takingthe drug may assume an importance in theadolescent’s life out of proportion to other rewards.The development of addiction is like a viciouscycle: Chronic drug use not only realigns a person’spriorities but also may alter key brain areasnecessary for judgment and self-control, furtherreducing the individual’s ability to control or stoptheir drug use. This is why, despite popular belief,willpower alone is often insufficient to overcomean addiction. Drug use has compromised the veryparts of the brain that make it possible to “say no.”Not all young people are equally at risk fordeveloping an addiction. Various factors includinginherited genetic predispositions and adverseexperiences in early life make trying drugs anddeveloping a substance use disorder more likely.Exposure to stress (such as emotional or physicalabuse) in childhood primes the brain to be sensitiveFor purposes of this guide, the term addiction refers to compulsive drug seeking and use that persists even in the face of devastating consequences;it may be regarded as equivalent to a severe substance use disorder as defined by the Diagnostic and Statistical Manual of Mental Disorders, FifthEdition (DSM-5, 2013). The spectrum of substance use disorders in the DSM-5 includes the criteria for the DSM-4 diagnostic categories of abuse anddependence.4 Principles of Adolescent Substance Use Disorder Treatment: A Research-Based Guide
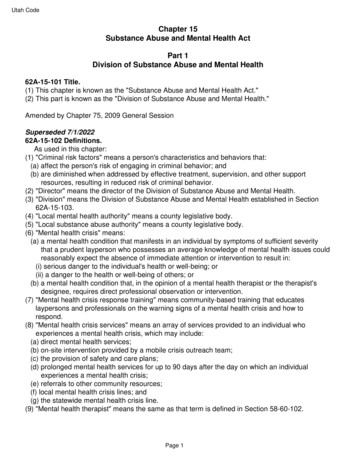
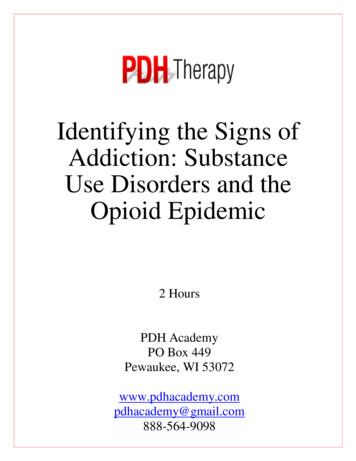
Adolescents Differ from Adults in Substances Most Abused8018 – 257026 rijuana 1.712.43.018.38.61012.62017.1Percent of those who received past-year treatment12 – 17Hallucinogens InhalantsSource: SAMHSA, Center for Behavioral Health Statistics and Quality, National Survey on Drug Use and Health, 2013.to stress and seek relief from it throughoutlife; this greatly increases the likelihood ofsubsequent drug abuse and of starting drug useearly.5 In fact, certain traits that put a personat risk for drug use, such as being impulsiveor aggressive, manifest well before the firstepisode of drug use and may be addressedby prevention interventions during childhood.6By the same token, a range of factors, suchas parenting that is nurturing or a healthyschool environment, may encourage healthydevelopment and thereby lessen the risk of laterdrug use.Drug use at an early age is an importantpredictor of development of a substance usedisorder later. The majority of those who havea substance use disorder started using beforeage 18 and developed their disorder by age 20.7The likelihood of developing a substance usedisorder is greatest for those who begin use intheir early teens. For example, 15.2 percent ofpeople who start drinking by age 14 eventuallydevelop alcohol abuse or dependence (ascompared to just 2.1 percent of those who waituntil they are 21 or older),8 and 25 percent ofthose who begin abusing prescription drugs atage 13 or younger develop a substance usedisorder at some time in their lives.9 Tobacco,alcohol, and marijuana are the first addictivesubstances most people try. Data collectedin 2012 found that nearly 13 percent of thosewith a substance use disorder began usingmarijuana by the time they were 14.10When substance use disorders occur inadolescence, they affect key developmentaland social transitions, and they can interferewith normal brain maturation. These potentiallylifelong consequences make addressingadolescent drug use an urgent matter. Chronicmarijuana use in adolescence, for example, hasbeen shown to lead to a loss of IQ that is notrecovered even if the individual quits using inadulthood.11 Impaired memory or thinking abilityand other problems caused by drug use canderail a young person’s social and educationaldevelopment and hold him or her back in life.The serious health risks of drugs compoundthe need to get an adolescent who is abusingdrugs into treatment as quickly as possible.Also, adolescents who are abusing drugs arelikely to have other issues such as mental healthPrinciples of Adolescent Substance Use Disorder Treatment: A Research-Based Guide 5
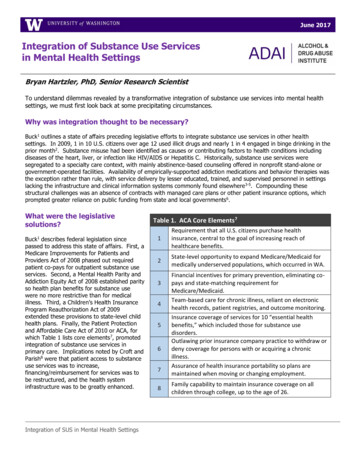
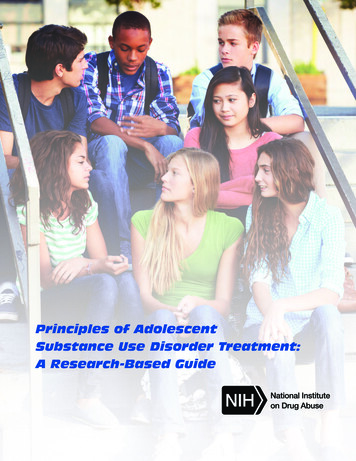
problems accompanying and possibly contributingto their substance use, and these also need tobe addressed.12 Unfortunately, less than onethird of adolescents admitted to substance abusetreatment who have other mental health issuesreceive any care for their conditions.13Adolescents’ drug use and treatment needsdiffer from those of adults. Adolescents intreatment report abusing different substances thanadult patients do. For example, many more peopleaged 12–17 received treatment for marijuanause than for alcohol use in 2011 (65.5 percentversus 42.9 percent), whereas it was the reversefor adults (see figure, page 5). When adolescentsdo drink alcohol, they are more likely than adultsto binge drink (defined as five or more drinks in arow on a single occasion).14 Adolescents are lesslikely than adults to report withdrawal symptomswhen not using a drug, being unable to stopusing a drug, or continued use of a drug in spiteof physical or mental health problems; but theyare more likely than adults to report hiding theirsubstance use, getting complaints from othersabout their substance use, and continuing to usein spite of fights or legal trouble.substance use problems often feel they donot need help, engaging young patients intreatment often requires special skills andpatience.Many treatment approaches are available toaddress the unique needs of adolescents.The focus of this guide is on evidence-basedtreatment approaches―those that have beenscientifically tested and found to be effectivein the treatment of adolescent substanceabuse. Whether delivered in residential orinpatient settings or offered on an outpatientbasis, effective treatments for adolescentsprimarily consist of some form of behavioraltherapy. Addiction medications, while effectiveand widely prescribed for adults, are notgenerally approved by the U.S. Food andDrug Administration (FDA) for adolescents.However, preliminary evidence from controlledtrials suggest that some medications mayassist adolescents in achieving abstinence,so providers may view their young patients’needs on a case-by-case basis in developing apersonalized treatment plan.Adolescents also may be less likely than adultsto feel they need help or to seek treatment ontheir own. Given their shorter histories of usingdrugs (as well as parental protection), adolescentsmay have experienced relatively few adverseconsequences from their drug use; their incentiveto change or engage in treatment may correspondto the number of such consequences they haveexperienced.15 Also, adolescents may have moredifficulty than adults seeing their own behaviorpatterns (including causes and consequences oftheir actions) with enough detachment to tell theyneed help.Whatever a person’s age, treatment is not “onesize fits all.” It requires taking into account theneeds of the whole person—including his orher developmental stage and cognitive abilitiesand the influence of family, friends, and othersin the person’s life, as well as any additionalmental or physical health conditions. Suchissues should be addressed at the same timeas the substance use treatment. When treatingadolescents, clinicians must also be readyand able to manage complications related totheir young patients’ confidentiality and theirdependence on family members who may ormay not be supportive of recovery.Only 10 percent of 12- to 17-year-olds needingsubstance abuse treatment actually receive anyservices.16 When they do get treatment, it is oftenfor different reasons than adults. By far, the largestproportion of adolescents who receive treatmentare referred by the juvenile justice system (seefigure, page 7). Given that adolescents withSupporting Ongoing Recovery—SustainingTreatment Gains and Preventing RelapseEnlisting and engaging the adolescent intreatment is only part of a sometimes long andcomplex recovery process.17 Indeed, treatmentis often seen as part of a continuum of care.When an adolescent requires substance6 Principles of Adolescent Substance Use Disorder Treatment: A Research-Based Guide
Number of Adolescents Aged 12–17 Admitted to Publicly FundedSubstance Abuse Treatment Facilities on an Average Day, by PrincipalSource of Referral: Treatment Episode Data Set 2008*2001841501006350460JuvenileJusticeSystemSelf ProvidersSource: 2008 SAMHSA Treatment Episode Data Set (TEDS)abuse treatment, follow-up care and recoverysupport (e.g., mutual-help groups like 12-stepprograms) may be important for helping teensstay off drugs and improving their quality of life.When substance use disorders are identifiedand treated in adolescence—especially if theyare mild or moderate—they frequently giveway to abstinence from drugs with no furtherproblems. Relapse is a possibility, however, asit is with other chronic diseases like diabetesor asthma. Relapse should not be seen as asign that treatment failed but as an occasionto engage in additional or different treatment.Averting and detecting relapse involves*18OtherHealthCareProfessionalsmonitoring by the adolescent, parents, andteachers, as well as follow-up by treatmentproviders. Although recovery support programsare not a substitute for formal evidence-basedtreatment, they may help some adolescentsmaintain a positive and productive drug-freelifestyle that promotes meaningful and beneficialrelationships and connections to family, peers,and the community both during treatment andafter treatment ends. Whatever services orprograms are used, an adolescent’s path torecovery will be strengthened by support fromfamily members, non-drug-using peers, theschool, and others in his or her life.“Treatment provi
during adolescence and young adulthood.‡ By the time they are seniors, almost 70 percent of high school students will have tried alcohol, half will have taken an illegal drug, nearly 40 percent will have smoked a cigarette, and more than 20 percent will have used a prescription drug for a nonmedical purpose.1 There are many reasons adolescents